Mortality in Ventilator‐Associated Tracheobronchitis and Pneumonia in Oncology Patients: The Impact of Microbiological Aspects
Vitor Falcao de Oliveira, Débora de Oliveira Lopes, Valdirene Santos Folli Cabral, Luiz Dalfior Junior, Simone Siqueira Matos, Luciana Alexandra Antônia de Almeida, Larissa Vasconcelos Barreto, João Manoel da Silva Junior, Ana Paula Cury, Odeli Nicole Encinas Sejas

TL;DR
This study examines the mortality and microbiological factors in ventilator-associated tracheobronchitis and pneumonia among cancer patients in an ICU.
Contribution
The study provides insights into the microbiological profile and mortality factors specific to oncology ICU patients with ventilator-associated infections.
Findings
Tracheobronchitis was more common than pneumonia in the studied ICU population.
P. aeruginosa, K. pneumoniae, and S. maltophilia were the most frequent pathogens.
VAP and positive blood cultures were independently associated with higher 14-day mortality.
Abstract
Most evidence on ventilator‐associated pneumonia (VAP)–related and ventilator‐associated tracheobronchitis (VAT)–related mortality comes from general ICU settings, with limited data on critically ill cancer patients. This study aimed to characterize the microbiological profile and resistance patterns in an oncology hospital and evaluate their impact on 14‐day mortality. We conducted a retrospective analysis of VAP and VAT cases in an oncology ICU in Brazil (Jan–Dec 2024), assessing bacterial frequency, multidrug‐resistant organisms (MDRO), and mortality. Multivariate analysis was used to identify the variables significantly associated with mortality. Among 85 ICU patients, tracheobronchitis was more frequent (59%) than pneumonia (41%). Most were male (61%) with a median age of 62 years and had solid tumors (85%), mainly in the lungs and neck. Of 109 samples, P. aeruginosa (27%), K.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
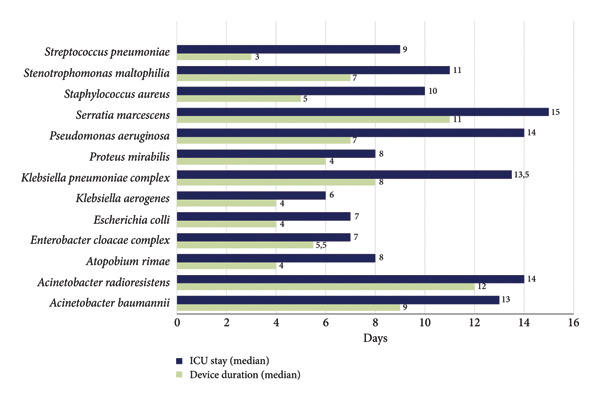 Figure 2
Figure 2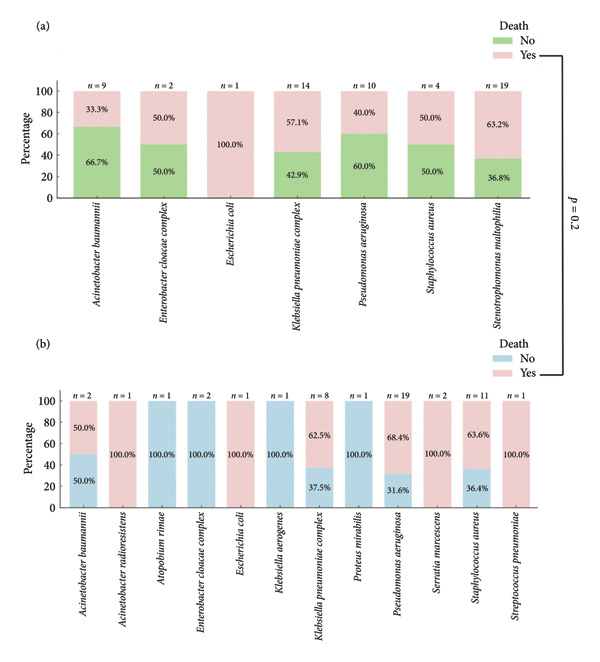 Figure 3
Figure 3| Characteristic | Number (%) |
|---|---|
| Age (years), median (IQR) | 62 (53–70) |
| Male sex | 52 (61) |
| Pneumonia | 35 (41) |
| Tracheobronchitis | 50 (59) |
| Solid tumor | 72 (85) |
| Neck cancer | 11 (15) |
| Mediastinal cancer | 3 (4) |
| Breast cancer | 6 (8) |
| Kidney cancer | 2 (3) |
| Bladder cancer | 2 (3) |
| Bone cancer | 2 (3) |
| Central nervous system cancer | 5 (6) |
| Prostate cancer | 7 (10) |
| Uterus and ovarian cancer | 5 (6) |
| Testicular cancer | 2 (3) |
| Gastrointestinal cancer | 7 (10) |
| Lung/bronchial cancer | 13 (18) |
| Liver cancer | 2 (3) |
| Undefined | 2 (3) |
| Other | 3 (4) |
| Hematological malignancy | 13 (15) |
| Acute leukemia | 3 (23) |
| Multiple myeloma | 3 (23) |
| Lymphoma | 6 (46) |
| Ambiguous phenotype | 1 (8) |
| Multidrug‐resistant infection | 30 (35) |
| 14‐day mortality | 47 (55) |
| Microorganisms | Total ( | MDR (%) | Death (%) |
|---|---|---|---|
|
| 11 (10) | 9 (82) | 4 (36) |
|
| 1 (1) | 0 (0) | 1 (100) |
|
| 1 (1) | 0 (0) | 0 (0) |
|
| 4 (4) | 2 (50) | 1 (25) |
|
| 2 (2) | 1 (50) | 2 (100) |
|
| 1 (1) | 0 (0) | 0 (0) |
|
| 22 (20) | 14 (64) | 13 (59) |
|
| 1 (1) | 0 (0) | 0 (0) |
|
| 29 (27) | 10 (38) | 17 (58) |
|
| 2 (2) | 0 (0) | 2 (100) |
|
| 15 (14) | 4 (27) | 9 (60) |
|
| 19 (17) | 100 (19) | 12 (63) |
|
| 1 (1) | 0 (0) | 1 (100) |
| Characteristic | Survivors ( | Nonsurvivors ( |
|
|---|---|---|---|
| Age (years), median (IQR) | 61 (44–69) | 62 (55–70) | 0.4 |
| Male sex | 22 (59%) | 30 (65%) | 0.6 |
| Respiratory tract infection |
| ||
| Pneumonia | 9 (24%) | 26 (55%) | |
| Tracheobronchitis | 29 (76%) | 21 (45%) | |
| Type of malignancy | > 0.9 | ||
| Solid tumor | 32 (84%) | 40 (85%) | |
| Hematological malignancy | 6 (16%) | 7 (15%) | |
| Positive blood culture | 3 (8%) | 13 (28%) |
|
| SAPS III, median (IQR) | 63 (48–73) | 63 (54–71) | 0.8 |
| Multidrug resistant | 16 (42%) | 14 (30%) | 0.2 |
| Bacteria | |||
|
| 4 (11%) | 2 (4%) | 0.4 |
|
| 8 (21%) | 8 (17%) | 0.6 |
|
| 7 (18%) | 7 (15%) | 0.7 |
|
| 2 (5%) | 4 (9%) | 0.7 |
|
| 6 (16%) | 9 (19%) | 0.7 |
| Polymicrobial | 8 (21%) | 14 (30%) | 0.4 |
| Appropriateness of initial antibiotic therapy | 21 (55%) | 23 (49%) | 0.6 |
| Characteristics | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI |
| OR | 95% CI |
| |
| Pneumonia | 4.20 | 1.63–11.7 |
| — | — | — |
| Malignancy | 1.54 | 0.41–5.85 | 0.5 | 1.82 | 0.47–7.91 | 0.4 |
| Positive blood culture | — | — | — | 5.38 | 1.43–28.1 |
|
| Multidrug resistant | 0.61 | 0.23–1.58 | 0.3 | 0.6 | 0.23–1.51 | 0.3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNosocomial Infections in ICU · Tracheal and airway disorders · Antibiotic Resistance in Bacteria
1. Introduction
Ventilator‐associated pneumonia (VAP) and ventilator‐associated tracheobronchitis (VAT) often occur as a complication in critically ill patients [1–4]. In the context of healthcare‐associated infections, VAP is the most frequent and severe infection affecting patients hospitalized in intensive care units (ICUs) [5–7]. The incidence of VAP varies widely in the international literature, ranging from 8% to 30%. This variability reflects differences in patient profiles, duration of mechanical ventilation, diagnostic criteria, and surveillance contexts [2, 8–11].
The overall reported mortality from VAP ranges between 20% and 60%, in addition to its impact on prolonged hospitalization and increased cost per episode [12–14]. However, establishing a direct causal link is challenging due to the severity of the underlying conditions, particularly malignancies [8, 15].
Current scientific literature identifies several risk factors associated with increased mortality from VAP in oncology patients. These factors can be grouped into three main categories: clinical, microbiological, and treatment‐related [6, 16, 17]. From a microbiological perspective, infections caused by multidrug‐resistant (MDR) pathogens, particularly Acinetobacter baumannii, and the presence of bilateral pulmonary infiltrates are associated with worse outcomes.
Despite these findings, most of the available evidence on risk factors for VAP‐related mortality originates from studies conducted in general ICU populations and does not fully reflect the specificities of oncological patients. Individuals with cancer often present distinct clinical features, such as persistent immunosuppression and greater prior exposure to broad‐spectrum antimicrobials, which may significantly alter both microbiological profiles and clinical outcomes [16, 18].
Moreover, the high incidence of MDR pathogens in this group poses additional challenges for therapeutic management. A significant gap remains in the literature regarding the impact of these pathogens and their resistance patterns on short‐term mortality in critically ill cancer patients, highlighting the need for targeted studies in this population [16, 18]. Our objectives in this study were to characterize the microbiological profile of patients with VAP and VAT in oncological ICU and to assess the impact of the isolated microorganisms and their resistance pattern on 14‐day mortality.
2. Methods
2.1. Setting and Study Design
We performed a retrospective analysis of prospectively collected data from adult patients consecutively diagnosed with VAP and VAT in an oncological ICU in a Brazilian public hospital between January and December 2024.
Instituto do Câncer do Estado de São Paulo (ICESP) is a tertiary hospital with 490 beds and an ICU, with 85 beds, dedicated to adult oncological medical and surgical patients.
Ethical approval for this study was granted by the local committee. Confidential and sensitive data were removed, and all identification codes were anonymized. The ethics review board waived the requirement for informed consent.
2.2. Diagnosis and Definitions
The diagnosis of VAP and VAT was based on the CDC/NHSN diagnostic criteria, summarized in the supporting information (Table S1) [19, 20]. The bacteriologic diagnosis was obtained by quantitative culture using a positive threshold of 10^5^ and 10^4^ colony forming units (CFU/mL) for endotracheal aspirates and bronchoalveolar lavage (BAL) fluids, respectively. Cultures were considered as polymicrobial if > 1 microorganisms grew.
MDR organisms (MDRO) were defined as bacteria which exhibited resistance to one or more categories of antimicrobial drugs. These encompass methicillin‐resistant Staphylococcus aureus (MRSA), carbapenem‐resistant Enterobacterales (CRE), Gram‐negative bacteria producing extended‐spectrum ß‐lactamase, and organisms such as Stenotrophomonas maltophilia that are intrinsically resistant to the broadest‐spectrum antimicrobial agents [21].
Bacterial isolates were identified using matrix‐assisted laser desorption/ionization time of flight mass spectrometry (MALDI‐TOF MS) (bioMerieux). Antimicrobial susceptibility testing was performed using an automated system (Vitek 2 XL, bioMerieux) for the majority of isolates and complemented by disk diffusion for nonfermenting Gram‐negative bacilli, in accordance with the criteria and breakpoints established by the Clinical and Laboratory Standards Institute (CLSI). In cases of MDRO or discrepant results, additional confirmatory testing was performed as needed.
2.3. Collected Data
The following patient data were collected at diagnosis: age, sex, malignancies, duration of mechanical ventilation, ICU stay until the diagnosis of infection, culture of blood and respiratory samples (BAL or endotracheal aspirates), antimicrobial susceptibility test, severity score (SAPS III), appropriateness of initial antibiotic therapy, and mortality within 14 days.
Initial antibiotic therapy was considered appropriate when the bacteria identified in vitro were susceptible to at least one of the antibiotics administered within 48 h of the infection diagnosis. Empirical antimicrobials were selected based on the physician’s clinical judgment and internal ICU protocols.
2.4. Statistical Analysis
Analyses were performed using RStudio software Version 1.4. The frequency of bacteria, MDROs, types of malignancies, and deaths was assessed using total counts and percentages for categorical variables, while the median and interquartile range (IQR) were used for continuous variables, such as age and SAPS III.
We conducted comparisons between the survival and nonsurvival groups, as well as compared the clinical and microbiological characteristics of patients with VAT and VAP. For this analysis, categorical variables were assessed using Fisher’s exact test and Pearson’s chi‐squared test as appropriate, while the Mann–Whitney test was applied to continuous variables. Multivariable logistic regression analysis was performed to identify factors independently associated with mortality. The model included the type of malignancy, MDR status, and variables that were statistically significant in the group comparisons. Statistical significance was defined by a p value < 0.05.
3. Results
A total of 85 patients presented VAT and VAP during ICU stay. Tracheobronchitis was diagnosed in 50 cases (59%), while pneumonia was identified in 35 cases (41%). The majority was male (n = 52, 61%), and the median age was 62 years (IQR 53–70). VAT and VAP patient clinical characteristics are summarized in Table 1. Most patients had solid tumors (n = 72, 85%), primarily located in the neck (n = 11, 15%) and lungs/bronchi (n = 13, 18%). Among the hematological malignancies, almost half of the cases were lymphomas (n = 6).
We isolated 109 bacterial strains from these 85 respiratory infections, 22 of which (26%) were polymicrobial. The most common microorganisms were Pseudomonas aeruginosa (27%), followed by Klebsiella pneumoniae (20%) and S. maltophilia (17%) (Table 2). The most frequent microorganism combinations isolated in polymicrobial infections were K. pneumoniae + P. aeruginosa (n = 4), P. aeruginosa + S. maltophilia (n = 3), and P. aeruginosa + S. aureus (n = 3).
Fifty‐nine (54%) of the bacterial isolates were classified as MDR. Among the MDROs, the bacteria with higher proportion of resistance, apart from Stenotrophomonas, were A. baumannii (82%), K. pneumoniae (64%), Enterobacter cloacae complex (50%), and Escherichia coli (50%). All cases of S. maltophilia were susceptible to trimethoprim–sulfamethoxazole and levofloxacin.
Ninety‐five microorganisms were isolated from respiratory samples, with a predominance of Gram‐negative bacteria, including P. aeruginosa, S. maltophilia, and K. pneumoniae as the most frequent (Figure 1(a)). The main type of sample collected was tracheal aspiration (n = 93, 98%), while only two patients underwent BAL sampling.
Figure 1. Frequency of microorganisms isolated from samples of patients with ventilator‐associated tracheobronchitis and pneumonia. (a) Respiratory samples and (b) blood samples.(a)(b)
Nineteen microorganisms were isolated from blood samples, also predominantly Gram‐negative, with K. pneumoniae being the most common (n = 9, 50%) (Figure 1(b)). The same microorganisms were isolated in blood and respiratory in four patients.
Patients infected with S. maltophilia, Acinetobacter spp., Serratia marcescens, P. aeruginosa, and K. pneumoniae presented longer hospital stays, with a median duration of more than 10 days. Device use was also prolonged in patients with infections caused by S. marcescens, K. pneumoniae, and Acinetobacter spp., with a median duration exceeding 7 days (Figure 2). Additionally, regarding the type of airway device, 27% (23/85) of patients had a tracheostomy, while 73% (62/85) were intubated with an orotracheal tube.
Device duration and intensive care unit length of stay by microorganism for patients with ventilator‐associated tracheobronchitis and pneumonia.
The 14‐day mortality was 55% (47/85). Evaluating the deaths according to isolated microorganisms, we detected the highest rates associated to Acinetobacter radioresistens (n = 1, 100%), E. coli (n = 2, 100%), P. aeruginosa (n = 17, 58%), S. marcescens (n = 2, 100%), Streptococcus pneumoniae (n = 1, 100%), S. maltophilia (n = 12, 63%), S. aureus (n = 9, 60%), and K. pneumoniae complex (n = 13, 59%) (Table 2).
Nonsurvivors and survivors showed similar distributions of age, sex, type of malignancy, SAPS III score, bacterial prevalence, and appropriateness of initial antibiotic therapy. Notably, there was no significant association between MDR and mortality (p = 0.2) (Figure 3 and Table 3). Mortality was 47% (14/30) among patients with MDR infections and 60% (33/55) among those with non‐MDR infections. However, patients with positive blood cultures had significantly higher mortality compared to those with only respiratory samples (28% versus 8%, p = 0.02).
Frequency of mortality within 14 days of hospitalization related to ventilator‐associated tracheobronchitis and pneumonia according to isolated microorganism. (a) MDR infection and (b) non‐MDR infection.
In the comparison between patients with VAP and VAT, mortality was significantly higher in the VAP group (74% vs. 42%, p = 0.003). In contrast, the prevalence of MDR pathogens, the distribution of bacterial species, the median duration of device use, and ICU length of stay were similar between the groups, with no statistically significant differences (Table S2).
In the multivariate analysis, positive blood cultures and VAP were analyzed separately because both variables showed high collinearity based on the diagnostic criteria (all patients with positive blood cultures had VAP). Positive blood cultures (OR 5.38, 95% CI: 1.43–28.1, p = 0.023) and VAP (OR 4.20, 95% CI: 1.63–11.7, p = 0.004) were independently associated with mortality, whereas MDR infection was not associated with mortality in either model (p = 0.3) (Table 4).
4. Discussion
Mortality among oncological patients with VAP and VAT was high, exceeding 50%, primarily associated with Gram‐negative bacteria isolated from respiratory and blood samples. Patients with positive blood cultures had higher mortality than those with only respiratory samples, although this was not significantly associated with the MDRO status. A. baumannii showed the highest resistance, but mortality was greater among patients infected with S. maltophilia or S. aureus.
As observed in our study, respiratory tract infections are most frequent in patients with leukemia/lymphoma and in those with lung or neck solid tumors [22]. VAP and VAT are predominantly caused by bacteria, while fungi and viruses are infrequent etiological agents [23]. In oncology patients, the microbial etiology of these infections reflects an immunocompromised status, prolonged use of invasive devices, and frequent prior exposure to broad‐spectrum antimicrobials [18]. The most commonly isolated pathogens in ICU‐acquired pneumonia include especially Gram‐negative bacteria such as K. pneumoniae and P. aeruginosa, as well as Gram‐positive organisms such as S. aureus [8, 23–26]. According to Canadian guidelines, S. aureus and P. aeruginosa are the most frequently isolated organisms in adults with nosocomial pneumonia from ICU settings [27]. Interestingly, S. maltophilia was the third most common pathogen in our study, which is unusual compared to other series in nononcological populations. It has been described that the primary predisposing factor for S. maltophilia infection is an immunocompromised status [27, 28].
Positive blood cultures range from 0% to 40% as reported in the AMMI Canada guidelines for hospital‐acquired pneumonia and VAP [29]. A previous study demonstrated that blood cultures had a higher proportion of Gram‐positive bacteria for healthcare‐associated pneumonia, such as S. aureus and S. pneumoniae, compared to respiratory samples, which showed a lower proportion of Gram‐negatives (55% vs. 36%) [30]. However, our study revealed that even in blood cultures, Gram‐negative bacteria were predominant. In fact, the proportion of patients with Gram‐positive bacteria was actually higher in respiratory samples than that in blood cultures. In the same study, mortality was higher among patients with positive blood cultures [30], a finding also observed in our study.
VAP and VAT can be polymicrobial in up to 30% of cases, which is consistent with our findings (26%). The increasing prevalence of MDRO further highlights the importance of early risk stratification and the appropriate selection of empirical antimicrobial therapy [5, 31], due to its association with higher mortality for VAP. The ICU 30‐day mortality rate ranged from 31.9% to 66.7% for A. baumannii, particularly for MDR [32]. In our study, A. baumannii showed the highest proportion of multidrug resistance. Consistently, more than 70% of the patients who died had infections caused by MDR. However, we found no association between MDR and mortality across all microorganisms. This likely reflects the impact of underlying conditions, particularly malignancies, which on their own can explain the higher mortality.
This study has some limitations. Being a single‐center and retrospective study, its findings may have limited generalizability, particularly to ICUs with different pathogen profiles or institutional practices. Mortality may have been influenced not only by the bacterial profile but also by factors not assessed in our analysis, such as the stage of oncological treatment. Additionally, some bacteria had small sample sizes in this study, which may have overestimated the mortality. Further studies are needed to better understand the microbiological factors associated with mortality in this oncology population.
5. Conclusion
This study provides valuable insights into the microbiological profile of patients with VAP and VAT in an oncological ICU and its impact on mortality. Gram‐negative bacteria were predominant, including in blood cultures, with S. maltophilia emerging unexpectedly as one of the most common pathogens. Mortality was not associated with MDR, as S. maltophilia showed high mortality, more than A. baumannii, despite being fully susceptible to trimethoprim–sulfamethoxazole and levofloxacin. However, patients with positive blood cultures and those with VAP had significantly higher mortality, suggesting a more invasive disease.
Disclosure
All authors reviewed and approved the final manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Contributions
Vitor Falcao de Oliveira, Odeli Nicole Encinas Sejas, and Edson Abdala wrote the main manuscript text. Débora de Oliveira Lopes, Valdirene Santos Folli Cabral, Larissa Vasconcelos Barreto, Odeli Nicole Encinas Sejas, Simone Siqueira Matos, and Luciana Alexandra Antônia de Almeida collected the data. João Manoel da Silva Junior, Ana Paula Cury, and Adriana Satie Gonçalves Kono Magri helped with the data curation and formal analysis. Vitor Falcao de Oliveira prepared all figures and tables.
Funding
This research received no external funding.
Supporting Information
Supporting Information associated with this article is available online and provides additional tables supporting the definitions and findings of this study.
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Papazian L. , Klompas M. , and Luyt C.-E. , Ventilator-Associated Pneumonia in Adults: A Narrative Review, Intensive Care Medicine. (2020) 46, no. 5, 888–906, 10.1007/s 00134-020-05980-0.32157357 PMC 7095206 · doi ↗ · pubmed ↗
- 2Charles M. P. , Kali A. , Easow J. M. et al., Ventilator-Associated Pneumonia, Australasian Medical Journal. (2014) 7, no. 8, 334–344, 10.4066/AMJ.2014.2105, 2-s 2.0-84906853016.25279009 PMC 4157153 · doi ↗ · pubmed ↗
- 3Kajeekul R. , Thamlikitkul V. , Wonglaksanapimon S. , and Rattanaumpawan P. , Epidemiology of Ventilator-Associated Tracheobronchitis and Ventilator-Associated Pneumonia Caused by Multidrug-Resistant Gram-Negative Bacteria at a Tertiary Care Hospital in Thailand, JAC Antimicrobial Resistance. (2024) 6, no. 1, 10.1093/jacamr/dlad 140.PMC 1075364838161966 · doi ↗ · pubmed ↗
- 4Martin-Loeches I. , Povoa P. , and Nseir S. , Ventilator Associated Tracheobronchitis and Pneumonia: One Infection With Two Faces, Intensive Care Medicine. (2023) 49, no. 8, 996–999, 10.1007/s 00134-023-07086-9.37160828 PMC 10425498 · doi ↗ · pubmed ↗
- 5Kalil A. C. , Metersky M. L. , Klompas M. et al., Management of Adults With Hospital-Acquired and Ventilator-Associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society, Clinical Infectious Diseases. (2016) 63, no. 5, e 61–e 111, 10.1093/cid/ciw 353, 2-s 2.0-84995377035.27418577 PMC 4981759 · doi ↗ · pubmed ↗
- 6Timsit J.-F. , Esaied W. , Neuville M. , Bouadma L. , and Mourvllier B. , Update on Ventilator-Associated Pneumonia, F 1000 Res. (2017) 6, 10.12688/f 1000 research.12222.1, 2-s 2.0-85036540984.PMC 571031329225790 · doi ↗ · pubmed ↗
- 7Vincent J.-L. , Rello J. , Marshall J. et al., International Study of the Prevalence and Outcomes of Infection in Intensive Care Units, Journal of the American Medical Association. (2009) 302, no. 21, 2323–2329, 10.1001/jama.2009.1754, 2-s 2.0-72249087115.19952319 · doi ↗ · pubmed ↗
- 8Howroyd F. , Chacko C. , Mac Duff A. et al., Ventilator-Associated Pneumonia: Pathobiological Heterogeneity and Diagnostic Challenges, Nature Communications. (2024) 15, no. 1, 10.1038/s 41467-024-50805-z.PMC 1129190539085269 · doi ↗ · pubmed ↗