Empagliflozin Perception Mapping Survey
Rajiv Kovil, Vijay Panikar, Jothydev Kesavadev, Snehal Tanna, Kamlesh Nayak, Dharmen Punatar, Lotika Purohit, Arun Kumar Kedia, Ami Sanghvi, Aravinda Jagadeesha, Sameer Chandratre, Sanhita Walawalkar, Mahendra Patel, Anil Kumar Virmani, Girish Mathur, Ketan K Mehta

TL;DR
This survey explores how Indian doctors perceive and prescribe empagliflozin, an SGLT2 inhibitor, for type 2 diabetes patients with heart and kidney issues.
Contribution
The study provides real-world insights into physician perceptions and prescribing practices of empagliflozin in India.
Findings
Most physicians recognize heart failure as underdiagnosed in T2DM and use empagliflozin for patients with cardiovascular and renal comorbidities.
Cost, guideline awareness, and therapeutic inertia remain barriers to optimal empagliflozin use.
Prescribing trends reflect recent evidence supporting empagliflozin in both HFrEF and HFpEF.
Abstract
Background: Heart failure (HF) is a frequent yet often underdiagnosed comorbidity among individuals with type 2 diabetes mellitus (T2DM). Sodium-glucose cotransporter-2 (SGLT2) inhibitors, particularly empagliflozin, are known to provide significant cardiovascular and renal benefits and are endorsed by international guidelines. However, real-world gaps in adoption persist, influenced by diagnostic challenges, cost considerations, and clinician familiarity. This survey assessed physician perceptions and prescribing practices regarding empagliflozin across diverse T2DM patient profiles in India. Methods: A cross-sectional, questionnaire-based survey was conducted using a voluntary convenience sampling approach among physicians from various specialities managing T2DM. As the study involved anonymized physician responses without patient-level data, ethical approval was not applicable. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
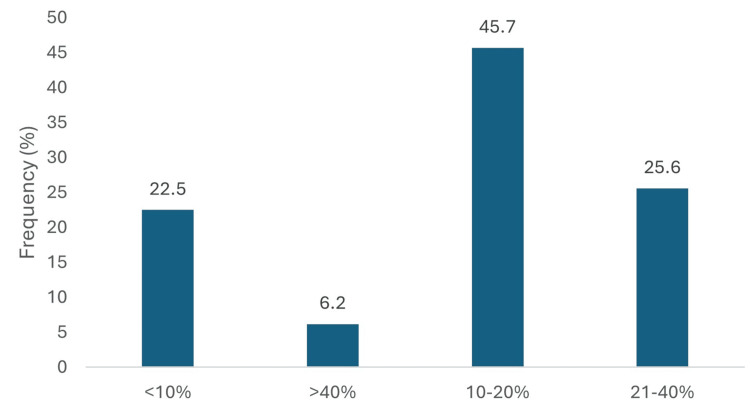 Figure 1
Figure 1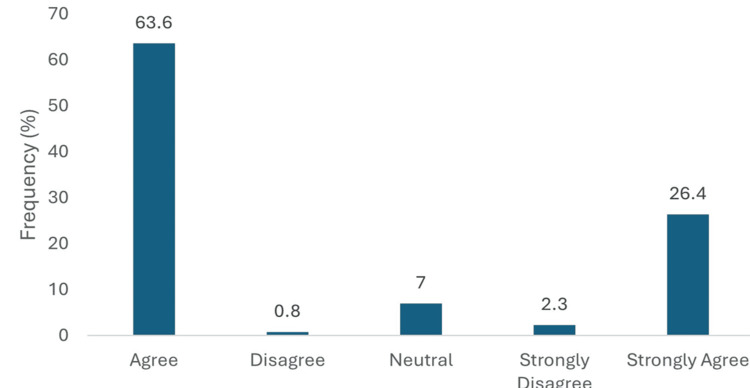 Figure 2
Figure 2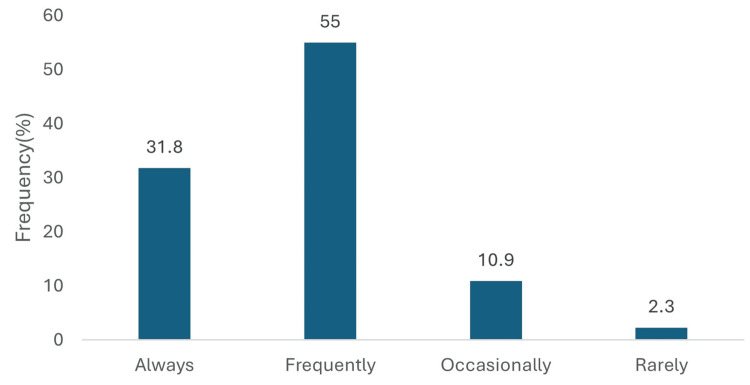 Figure 3
Figure 3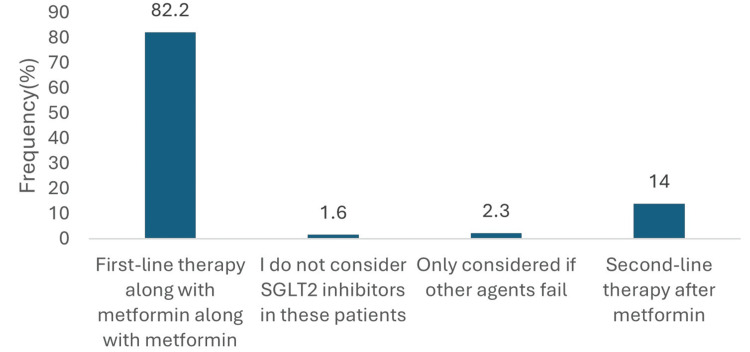 Figure 4
Figure 4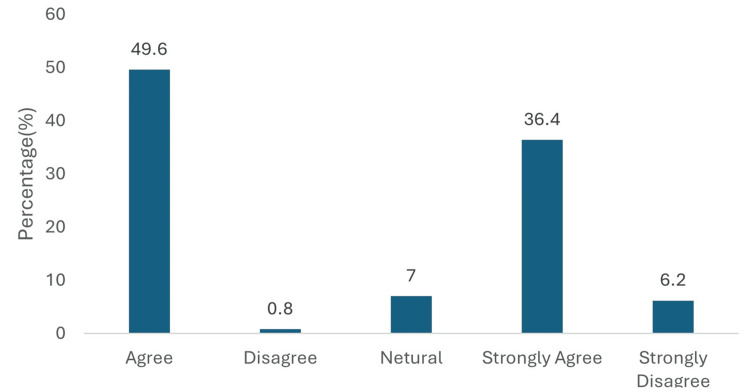 Figure 5
Figure 5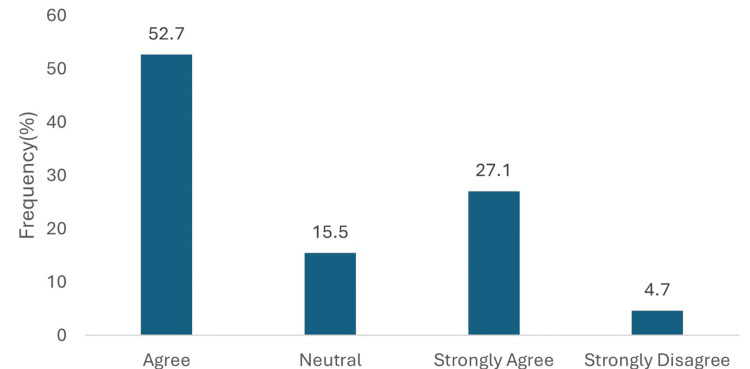 Figure 6
Figure 6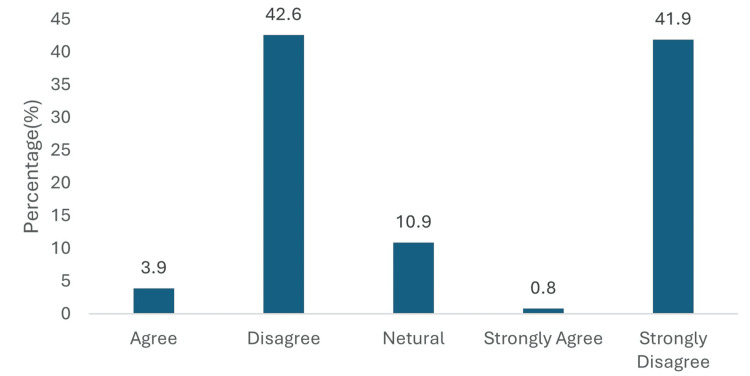 Figure 7
Figure 7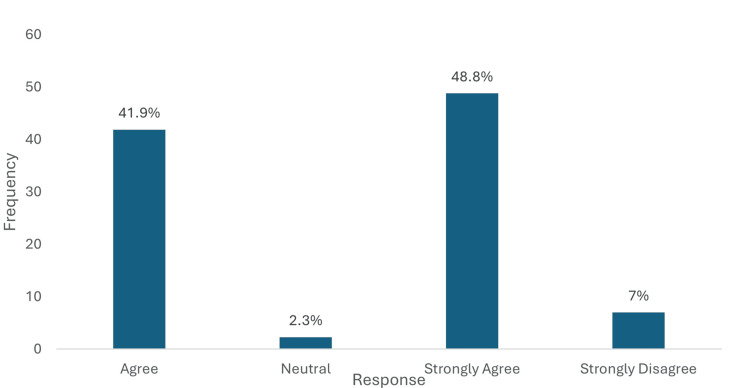 Figure 8
Figure 8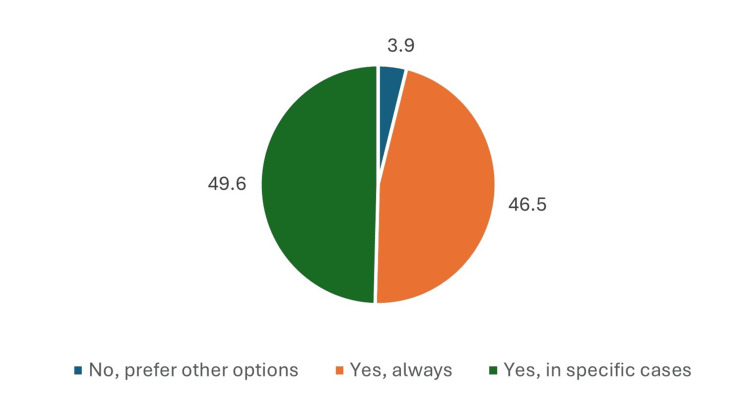 Figure 9
Figure 9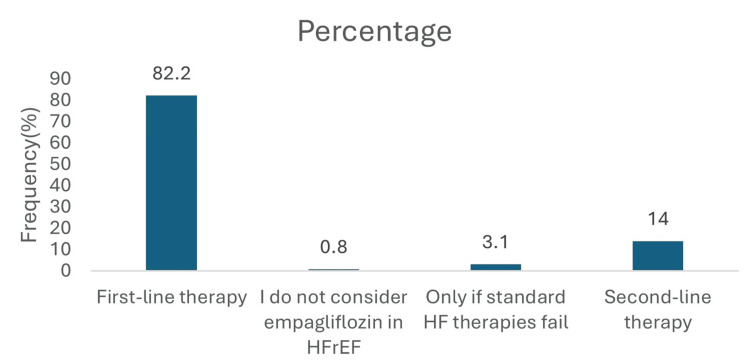 Figure 10
Figure 10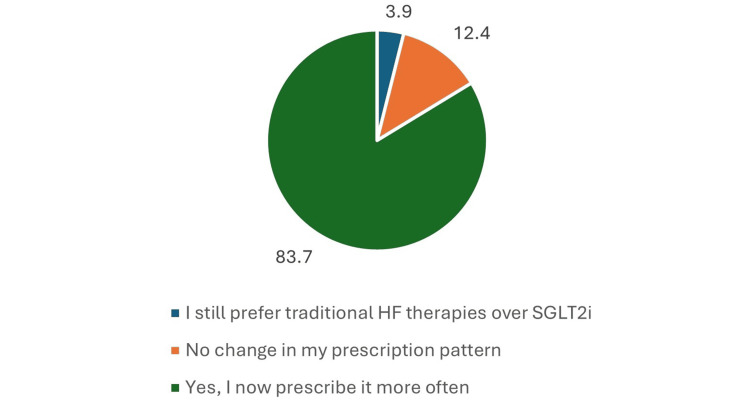 Figure 11
Figure 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiabetes Treatment and Management · Chronic Kidney Disease and Diabetes · Dialysis and Renal Disease Management
Introduction
In Individuals with type 2 diabetes mellitus (T2DM), heart failure (HF) is a common but often underdiagnosed comorbidity [1]. According to recent estimates, more than 537 million adults worldwide suffer from diabetes, and the disease prevalence is still rising [2]. India is one of the nations with the highest prevalence of diabetes, accounting for about 77 million of these cases [3]. An estimated 9% to 22% of patients with type 2 diabetes have heart failure, and even in the absence of a history of myocardial infarction or structural heart disease, the risk of developing heart failure is much higher in this population [4]. Crucially, because of overlapping symptoms and diagnostic complexity, a significant percentage of people with type 2 diabetes may have asymptomatic or undetected heart failure, especially heart failure with preserved ejection fraction (HFpEF) [5-7]. Furthermore, up to 40% and 25% of individuals with type 2 diabetes, respectively, have comorbid conditions like chronic kidney disease (CKD) and atherosclerotic cardiovascular disease (ASCVD), which makes management of the disease difficult and hence increases the risk of cardiovascular disease [8].
Sodium-glucose cotransporter-2 (SGLT2) inhibitors have emerged as an important component of the therapeutic armamentarium for T2DM, especially in patients with cardiovascular or renal comorbidities [9]. These agents work by blocking SGLT2 in the proximal renal tubule, which in turn reduces the kidney’s reabsorption of glucose and sodium. This mechanism leads to increased urinary glucose excretion, a modest degree of natriuresis, and a lowering of intraglomerular pressure [10,11]. One of these agents is empagliflozin, which is now recommended for patients with T2DM who also have coexisting cardiovascular or renal disease, according to guidelines from the American Diabetes Association (ADA) and Kidney Disease Improving Global Outcomes (KDIGO) [12,13]. In addition, there remain gaps in practical application despite this strong clinical evidence. Widespread adoption may be hampered by factors like cost, genitourinary infection risk, unfamiliarity with updated guidelines, and therapeutic inertia, according to reports from clinician surveys [14]. The Empagliflozin perception mapping survey aimed to evaluate physician perspectives on the use of empagliflozin in diverse clinical scenarios involving T2DM, with a focus on cardiovascular and renal risk profiles, heart failure management, and practical prescribing challenges.
Therefore, the present study aimed to evaluate physician perceptions and prescribing practices related to empagliflozin across diverse clinical scenarios in T2DM, with particular emphasis on cardiovascular risk, CKD, and heart failure management.
Materials and methods
Study design and participants
A cross-sectional survey was conducted to evaluate physician perspectives and prescribing practices regarding the use of empagliflozin in T2DM across diverse clinical scenarios. A total of 129 physicians were recruited using purposive sampling during advisory board meetings held between February and April 2025. Eligible participants included practising diabetologists, consulting physicians, cardiologists, and endocrinologists who manage patients with T2DM. Participation was voluntary, and physicians were invited to complete a structured questionnaire during the meetings or immediately thereafter via a secure survey link.
Survey instrument
The questionnaire consisted of 13 items developed specifically for this study. The survey underwent an internal two-step validation process (Appendix A).
Content Validation
Content validation was conducted by the study moderator and two independent clinical experts, who reviewed all items for clarity, relevance, and alignment with real-world practice.
Pilot Testing
The draft survey was piloted with five physicians to ensure clarity and usability. No major revisions were required. The questionnaire was organized into five clinically relevant domains: Participant demographics, including medical speciality and years of clinical experience; Physician assessment of heart failure prevalence and risk in the T2DM population; Selection preferences for SGLT2 inhibitors across different patient profiles; Utilization of empagliflozin in the management of heart failure; Identification of adverse effects and barriers to prescribing encountered in practice.
The survey included single-choice, multiple-choice, and Likert-scale questions, with response options ranging from strongly agree to strongly disagree, allowing for the capture of nuanced clinical perspectives and varying degrees of agreement.
Survey Administration and Data Collection
Data were collected from February to April 2025 using a secure, web-based survey platform. Participants submitted anonymized responses electronically. No identifying information was collected. All completed surveys were exported to a password-protected database for analysis.
Statistical analysis
Survey responses were collected and subjected to descriptive statistical analysis. Categorical variables were reported as frequencies and percentages to characterize response patterns. The analysist examined physician perceptions of empagliflozin's cardiovascular protective effects, renal benefits, and heart failure management efficacy across different patient populations encountered in clinical practice.
Ethical considerations
This study involved a voluntary, anonymized, opinion-based survey of licensed physicians and did not include any patient data, personal identifiers, or sensitive personal information. The questionnaire captured only professional practice perspectives related to prescribing patterns and clinical decision-making. According to institutional policy and prevailing national norms for minimal-risk research, surveys of healthcare professionals that do not collect identifiable information and do not involve patients are classified as exempt from formal ethics committee review. Therefore, this study met the criteria for exemption, and separate ethics committee approval was not required. Completion of the survey constituted implied consent for participation.
Results
A total of 129 physicians participated in the survey. The majority of respondents were diabetologists (78, 60.5%), followed by consulting physicians (45, 34.9%). Cardiologists and endocrinologists each comprised 2.3% of the sample (3 participants each). The physician cohort was highly experienced, with 77 (59.7%) having more than 20 years of clinical practice. Those with 11-20 years of experience represented 38 (29.5%), while physicians with 5-10 years and less than 5 years of experience comprised 11 (8.5% ) and 3 (2.3%), respectively.
When asked about the prevalence of undiagnosed heart failure among the T2DM, 59 (45.7%) estimated the rate to be 10-20%, while 33 (25.6%) believed it ranged from 21-40%. Only 8 (6.2%) suspected a prevalence above 40%, and 29 (22.5%) physicians estimated it to be below 10% (Figure 1).
Percentage of T2DM with undiagnosed heart failure.Data has been presented as %.
A substantial majority of physicians (116, 90.0%) believed that heart failure is underdiagnosed in T2DM patients, with 82 (63.6%) agreeing and 34 (26.4%) strongly agreeing with this statement. Only 1 (0.8%) disagreed, while 9 (7.0%) remained neutral and 3 (2.3%) strongly disagreed (Figure 2).
Heart failure underdiagnosed in T2DM.Data has been presented as %.
Among patients with T2DM who had multiple cardiovascular risk factors but no established atherosclerotic cardiovascular disease (ASCVD), 112 (86.8%) of physicians reported prescribing empagliflozin either frequently or always. Of these, 71 (55.0%) indicated that they frequently prescribed the medication, while 41 (31.8%) reported always prescribing it. In contrast, 14 (10.9%) prescribed it only occasionally, and 3 (2.3%) rarely used empagliflozin in this patient group (Figure 3).
Empagliflozin for T2DM with multiple cardiovascular risk factors.Data has been presented as %.
In patients with established ASCVD, the majority of physicians (106, 82.2%) reported prescribing empagliflozin as first-line therapy in combination with metformin. A smaller proportion (18, 14.0%) considered it as a second-line option following metformin. Very few physicians prescribed it only after failure of alternative treatments (3, 2.3%), and 2 (1.6%) did not consider SGLT2 inhibitors for this population (Figure 4).
Empagliflozin treatment preference ranking T2DM with ASCVD.Data has been presented as %.
Regarding empagliflozin's role in T2DM patients with chronic kidney disease (CKD) and proteinuria, physicians demonstrated strong confidence in its renal protective effects. For delaying CKD progression, 111 (86.0%) expressed positive views, with 64 (49.6%) agreeing and 47 (36.4%) strongly agreeing. Only 9 (7.0%) remained neutral, while disagreement was minimal (1, 0.8% disagreed; 8, 6.2% strongly disagreed) (Figure 5).
Perceived role of empagliflozin in delaying CKD progression.Data has been presented as %.
Similarly, for proteinuria reduction, 103 (79.8%) physicians responded positively, with 68 (52.7%) agreeing and 35 (27.1%) strongly agreeing, 20 (15.5%) remained neutral, and only 6 (4.7%) strongly disagreed. Physicians overwhelmingly rejected the notion that empagliflozin provides no significant renal benefit. A total of 109 (84.5%) disagreed with this statement, with 55 (42.6%) disagreeing and 54 (41.9%) strongly disagreeing. Only 6 (4.7%) expressed agreement (5, 3.9% agreed; 1, 0.8% strongly agreed) (Figure 6).
Perceived role of empagliflozin in reducing proteinuria in T2DM patients.Data has been presented as %.
Physicians overwhelmingly rejected the notion that empagliflozin provides no significant renal benefit. A total of 84.5% disagreed with this statement, with 55 physicians (42.6%) disagreeing and 54 physicians (41.9%) strongly disagreeing. Only 6 physicians (4.7%) expressed agreement (5, 3.9% agreed; 1, 0.8% strongly agreed) (Figure 7).
Perceived role of empagliflozin in reducing proteinuria in T2DM patients with CKD progression.Data has been presented as %.
A substantial majority of physicians (117, 90.7%) expressed positive perceptions regarding empagliflozin's cardiovascular benefits in T2DM with CKD and proteinuria. Specifically, 54 (41.9%) agreed, and 63 (48.8%) strongly agreed with the cardiovascular benefits. Only 9 (7.0%) strongly disagreed, while 3 (2.3%) remained neutral (Figure 8).
Perceptions regarding empagliflozin's cardiovascular benefits in Type 2 diabetes patients with CKD and proteinuria.Data has been presented as %.
When considering T2DM patients with CKD but without proteinuria, 124(96.1%) of physicians would prescribe empagliflozin. The majority (64, 49.6%) indicated they would prescribe it in specific cases, while 60 (46.5%) reported they would always prescribe it. Only 5 (3.9%) preferred other treatment options (Figure 9).
Empagliflozin prescribing decision in non-proteinuric CKD patients with T2DM.Data has been presented as %.
In T2DM patients with HFrEF: EF >40%, 106 (82.2%) prioritized empagliflozin as first-line therapy. An additional 18 (14.0%) considered it as second-line therapy. Only a small minority indicated its use solely after failure of standard heart failure therapies (4, 3.1%) or did not consider its use at all (1, 0.8%) (Figure 10).
Empagliflozin priority in T2DM with HFrEF; EF>40%.Data has been presented as %.
For patients with heart failure with HFpEF: EF >50%, recent clinical evidence significantly influenced prescribing patterns. Among all participants, 108 physicians (83.7%) reported that recent clinical evidence led them to prescribe empagliflozin more frequently. In contrast, 16 (12.4%) noted no change in their prescribing habits, and only 5 (3.9%) continued to prefer traditional heart failure therapies over SGLT2 inhibitors (Figure 11).
Change in prescribing behaviour (empagliflozin in HFpEF+T2DM).Data has been presented as %.
Discussion
This cross-sectional survey provides a real-world evaluation of physician perspectives on the use of empagliflozin across a range of clinical scenarios in patients with T2DM. The present findings indicate a high level of awareness among Indian clinicians about the cardiovascular and renal benefits of empagliflozin, especially in high-risk subgroups such as those with atherosclerotic cardiovascular disease (ASCVD), HF, and CKD. Nonetheless, our results also highlight critical perceptual and diagnostic gaps, particularly in the recognition of undiagnosed HF and the adoption of empagliflozin in CKD without proteinuria. These findings point to areas where further clinical education and implementation support may be necessary. However, these encouraging trends coexist with areas where clinical practice still falls short of current evidence, particularly in the early recognition of heart failure and consistent adoption of SGLT2 inhibitors in CKD without proteinuria.
Heart failure is increasingly recognized as a major comorbidity in T2DM, with prevalence estimates ranging from 9% to 22% in observational studies, even in the absence of overt cardiovascular disease or myocardial infarction history [12]. In line with these observations, the majority of respondents, 116 (90%), in our survey agreed that HF is underdiagnosed in T2DM populations. However, only a small proportion (8, 6.2%) estimated that more than 40% of their own patients might have undiagnosed HF. This discrepancy indicates that although physicians acknowledge HF under-recognition at a population level, they may underestimate its true burden in their own practice, a pattern previously observed in real-world cohorts where HF prevalence exceeded clinician expectations. Such findings echo prior real-world data, such as that reported byStoyanova et al., where HF prevalence among T2DM patients in a large German cohort exceeded 15%, yet initiation rates for evidence-based HF therapies remained suboptimal [1].
Most physicians in our study demonstrated guideline-concordant prescribing patterns for empagliflozin. In patients with ASCVD, 106 (82.2%) reported initiating empagliflozin as first-line therapy alongside metformin, consistent with the 2025 ADA Standards of Care, which recommend SGLT2 inhibitors with proven cardiovascular benefit irrespective of glycemic control [12]. The strong evidence base from the EMPA-REG OUTCOME trial and subsequent meta-analyses appears to have influenced these prescribing preferences, contributing to the widespread first-line positioning of empagliflozin reported by participants [15].
A majority (111, 86.0%) agreed that it delays CKD progression, and 103(79.8%) endorsed its role in proteinuria reduction. Notably, 124 (96.1%) indicated they would consider prescribing it in CKD patients without proteinuria, reflecting awareness of recent guideline updates, such as those from KDIGO 2022 and 2024 guideline updates, which recommend SGLT2 inhibitors based on eGFR thresholds rather than albuminuria status alone [16]. However, published registry data from Canada and other global settings suggest that actual prescribing rates remain lower, particularly in non-proteinuric CKD. Despite this alignment, several international registry studies have documented low real-world uptake of SGLT2 inhibitors among eligible patients, suggesting that familiarity with evidence does not necessarily translate into routine prescribing [17,18].
In the context of heart failure, most survey respondents reported a preference for empagliflozin as part of first-line therapy in patients with HFrEF, with 106 (82.2%) indicating its routine initiation in this population. This is consistent with ESC 2021 HF guidelines (reinforced by the 2023 focused update) and the ACC/AHA/HFSA 2022 HF guidelines, which position SGLT2 inhibitors as a component of foundational pharmacotherapy for HFrEF regardless of glycemic status [19]. Notably, 108 (83.7%) of surveyed physicians indicated that their prescribing of empagliflozin for HFpEF had increased following recent trial evidence. This reported change aligns with emerging data demonstrating significant reductions in HF hospitalizations and improvements in symptom burden among T2DM patients with preserved ejection fraction, even in the absence of substantial glucose-lowering effects. Nevertheless, observational analyses such as that by Abudureyimu et al. suggest that real-world uptake in HFpEF remains lower than expected, highlighting the importance of ongoing dissemination of trial findings and updated guideline recommendations [8].
While our survey focused on physician perceptions rather than actual prescription data, these findings can be better understood within broader implementation science frameworks. For example, Yi et al. applied the Consolidated Framework for Implementation Research (CFIR), identified multiple barriers to SGLT2 inhibitor uptake, including medication cost, incomplete guideline familiarity, concerns about adverse effects (such as genitourinary infections), and therapeutic inertia [14].
Our survey findings indicate that physicians are increasingly aligning their reported prescribing preferences with contemporary evidence supporting empagliflozin’s role in T2DM patients with cardiovascular and renal comorbidities. Nonetheless, the responses also suggest ongoing diagnostic caution in the detection of asymptomatic HF, some reluctance to routinely initiate therapy in normoalbuminuric CKD, and the persistence of systemic barriers such as cost and access. Addressing these gaps will likely require a combination of targeted educational initiatives, streamlined dissemination of updated guideline recommendations, and policy-level measures aimed at improving equitable availability of SGLT2 inhibitors across diverse clinical settings.
Being a cross-sectional, self-reported survey, the findings reflect physician perceptions at a single point in time and may be subject to recall and response bias. The modest sample size and unequal representation across specialities and geographic regions may limit the generalizability of the results to the wider clinician population. As the survey relied on stated practices rather than actual prescription data, discrepancies between perceived and real-world prescribing behavior cannot be excluded.
Conclusions
This nationwide survey provides insight into how physicians perceive the role of empagliflozin in managing Type 2 diabetes mellitus, particularly in individuals with cardiovascular or renal comorbidities. Respondents expressed confidence in its cardiorenal benefits, and many reported using it routinely in settings such as ASCVD, HFrEF, and proteinuric CKD. However, because the survey captured self-reported perceptions rather than actual prescribing data, these responses may not fully reflect real-world practice patterns. The findings also point to several areas where clinical practice may not yet be fully aligned with evidence, including the under-recognition of asymptomatic heart failure, inconsistent adoption in non-proteinuric CKD, and practical challenges such as cost, access, and awareness of evolving guidelines. Targeted educational initiatives, better diagnostic pathways, and supportive policy measures may help narrow these gaps and promote more consistent evidence-based use of SGLT2 inhibitors in routine diabetes care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heart failure among people with Type 2 diabetes mellitus: real-world data of 289 954 people from a diabetes database Diabet Med Stoyanova D Stratmann B Schwandt A 129112983720203070160710.1111/dme.13915 PMC 7496405 · doi ↗ · pubmed ↗
- 2IDF Diabetes Atlas 10th edition scientific committee IDF Diabetes Atlas [Internet] 10th edition Magliano DJ Boyko EJ Brussels International Diabetes Federation 2021 https://www.ncbi.nlm.nih.gov/books/NBK 581934/
- 3Epidemiology of type 2 diabetes in India Indian J Ophthalmol Pradeepa R Mohan V 293229386920213470872610.4103/ijo.IJO_1627_21PMC 8725109 · doi ↗ · pubmed ↗
- 4Type 2 diabetes mellitus and heart failure: a scientific statement from the American Heart Association and the Heart Failure Society of America: this statement does not represent an update of the 2017 ACC/AHA/HFSA Heart Failure Guideline update Circulation Dunlay SM Givertz MM Aguilar D 03241402019 https://www.acc.org/Latest-in-Cardiology/ten-points-to-remember/2019/06/18/14/27/http%3a%2f%2fwww.acc.org%2f Latest-in-Cardiology%2ften-points-to-remember%2f 2019%2f 06%2f 18%2f 14%2f 27%2f Type-2-Diabetes-Melli · doi ↗ · pubmed ↗
- 5Epidemiology of heart failure in diabetes: a disease in disguise Diabetologia Hoek AG Dal Canto E Wenker E Bindraban N Handoko ML Elders PJ Beulens JW 5746016720243833481810.1007/s 00125-023-06068-2PMC 10904471 · doi ↗ · pubmed ↗
- 6Diabetes leading to heart failure and heart failure leading to diabetes: epidemiological and clinical evidence Heart Fail Rev Palazzuoli A Iacoviello M 5855962820233552239110.1007/s 10741-022-10238-6PMC 10140137 · doi ↗ · pubmed ↗
- 7Observational study investigating the prevalence of asymptomatic stage B heart failure in patients with type 2 diabetes who are not known to have coronary artery disease BMJ Open Oo MM Tan Chung Zhen I Ng KS 011202110.1136/bmjopen-2020-039869 PMC 782525433478961 · doi ↗ · pubmed ↗
- 8Heart failure with preserved ejection fraction (H Fp EF) in type 2 diabetes mellitus: from pathophysiology to therapeutics J Mol Cell Biol Abudureyimu M Luo X Wang X 14202210.1093/jmcb/mjac 028PMC 946563835511596 · doi ↗ · pubmed ↗