Above-Knee Amputation in the Setting of a Chronic Soft Tissue Infection and Periprosthetic Joint Infection With Exposed Hardware
Kiana Bennett, Srikanth A Pillai, William F Oppat

TL;DR
A 71-year-old woman with a history of knee replacement and recurring infections required an above-knee amputation due to a chronic wound exposing the implant.
Contribution
This case report highlights the management of recurrent periprosthetic joint infections leading to above-knee amputation.
Findings
The patient had a 10-year history of complications following knee arthroplasty.
An above-knee amputation was performed due to a non-healing wound exposing the hardware.
Multidisciplinary care was essential in managing this complex case.
Abstract
Total knee arthroplasty is one of the most common and successful orthopedic surgeries for the treatment of osteoarthritis. While infection is a common postoperative complication, periprosthetic joint infection is a rarer type of infection requiring aggressive treatment. This case report reviews the clinical course of a 71-year-old female with a history of recurrent prosthetic joint infections and osteomyelitis of the left knee and femur following a left total knee arthroplasty. Ten years after the index procedure, she developed a soft tissue ulcer and non-healing wound that led to exposure of her knee joint hardware at the level of the skin. Due to her complicated medical history, it was decided she would undergo an above-knee amputation. This report discusses a unique patient history of recurrent periprosthetic joint infections requiring extensive surgical and medical management,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4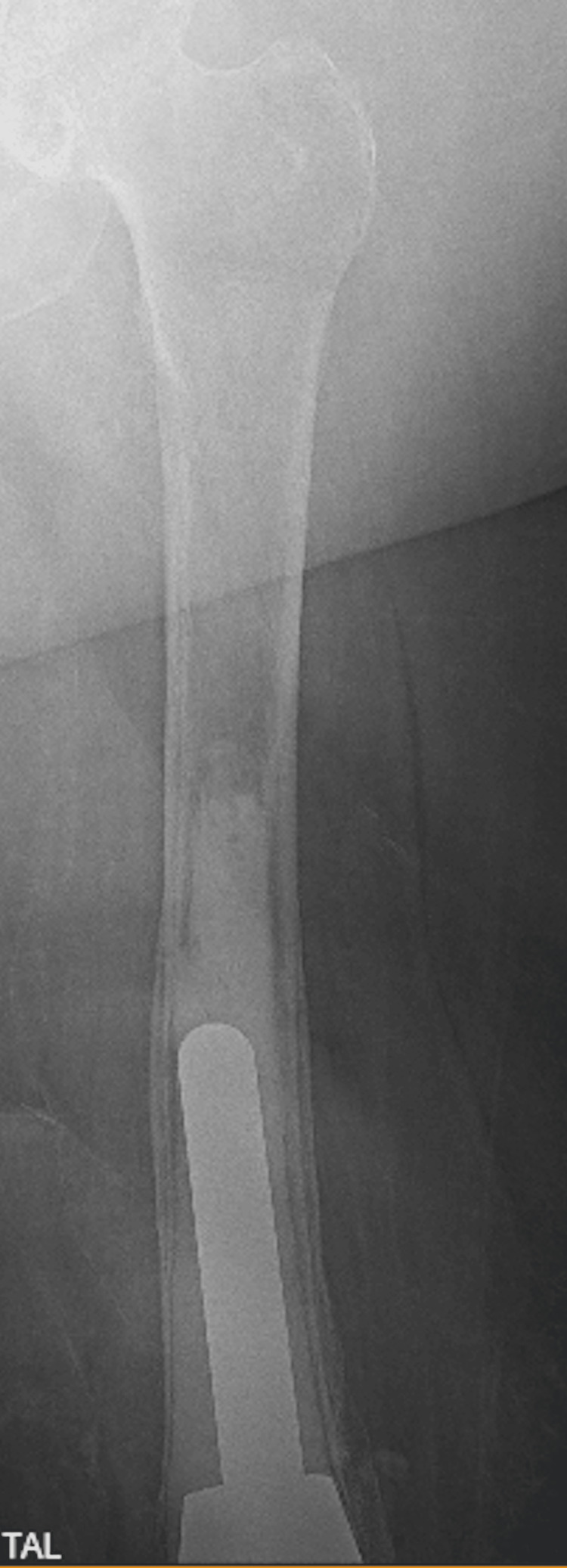 Figure 5
Figure 5| Year | Clinical course description | Microbiology | Treatment |
| August 2013 | Left TKA | ||
| August 2013 (2 weeks after index procedure) | Periprosthetic left femur fracture | Secondary reconstruction with distal femoral replacement | |
| July-August 2014 | PJI | Two strains of | Two-stage revision with six weeks of IV vancomycin and four to six weeks of oral minocycline |
| December 2014 | Revision arthroplasty | Four weeks of IV vancomycin in the setting of previous PJI | |
| January 2024 | Non-healing left knee wound with exposed hardware and left posterior thigh soft tissue wound |
| Wound care dressing changes. 12 weeks of IV dalbavancin. Close follow-up with the infectious disease department. |
| October 2024 | Non-healing left knee wound with exposed hardware and minimally improved left posterior thigh soft tissue wound. |
| High AKA with postoperative IV vancomycin |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Total Knee Arthroplasty Outcomes · Orthopaedic implants and arthroplasty
Introduction
Overall life expectancy continues to improve as total knee arthroplasty (TKA) has become a mainstay of treatment for debilitating osteoarthritis. Prosthetic joint infection (PJI) is a major cause of prosthetic failure after TKA with an estimated incidence between 0.5-2% [1]. It is associated with substantial morbidity, mortality, and cost [2]. Management of PJI involves a multidisciplinary approach including surgical revision, debridement, and antimicrobial therapy [3]. However, when multiple revisions and antibiotics fail to eradicate the infection, above-knee amputation (AKA) may be used as a salvage option [4]. Amputation allows patients to regain some mobility with the option for a prosthetic. Overall studies show patient satisfaction following AKA in this context is as high as 85% [5,6]. This remains a high-risk procedure in a vulnerable patient population with a 5-year mortality estimates as high as 50% [6].
This case discusses the complex history of a 71-year-old female who underwent a TKA that led to the development of multiple PJIs requiring a series of surgical interventions. Her care was closely monitored by the infectious diseases department, wound care clinic, and the orthopedic department with eventual involvement of the vascular surgery department. Ten years after her initial surgery, she developed a large posterior thigh pressure ulcer and a non-healing left knee wound with exposed hardware. After failed surgical and medical management and decreased quality of life, it was decided that she should undergo an AKA. This case aims to highlight the multidisciplinary approach to the management of chronic and complex PJIs, as well as present a unique case.
Case presentation
A 71-year-old female with a medical history significant for morbid obesity, recurrent renal calculi, neurogenic bladder, periprosthetic left femur fracture, recurrent osteomyelitis/PJI of the left knee and femur, and bilateral lower extremity chronic lymphedema presented to the emergency department (ED) following an outpatient visit with the infectious disease department. She has a complex history with the orthopedic and infectious disease departments following her TKA in 2013. Notable surgical history is a left TKA and ureteral stent placements, cystoscopy, and lithotripsy for recurrent renal calculi. Her social history notes that she lives in a skilled nursing facility requiring assistance with most activities of daily living. She has been non-ambulatory for over eight years.
She had a left TKA in 2013, and two weeks postoperatively, she had a periprosthetic femur fracture that required a secondary reconstruction with a distal femoral replacement. In mid 2014, she had presented to the ED for persistent knee pain following the secondary reconstruction. Arthrocentesis was done at the time, which grew two strains of coagulase-negative Staphylococcus epidermidis. During that time, she underwent a resection arthroplasty with placement of an antibiotic spacer and immobilization rod, followed by six weeks of IV vancomycin and then oral minocycline. Upon completion of her antibiotics, she underwent a revision arthroplasty with placement of a hinge prosthetic with postoperative IV vancomycin for four weeks due to her history of a previous infection.
In early 2024, she presented to the ED from the wound care clinic due to a non-healing left knee wound with exposed knee joint hardware (Figure 1). Cultures at that time grew Staphylococcus lugdunensis, and she was treated appropriately. She was then started on daily prophylactic antibiotics with doxycycline and 12 weeks of IV dalbavancin, which was managed by the infectious disease department. Wound care had also been following her for a pressure ulcer on the left posterior medial thigh (Figures 2, 3). By late 2024, her posterior medial thigh wound showed minimal improvement with oral and IV antibiotics. She was then referred to the ED for IV antibiotics and consideration of more aggressive treatment versus an above-knee amputation (AKA). Another culture was taken of the exposed hardware due to the purulent drainage seen at the left knee, which grew Pseudomonas aeruginosa. She was seen by the orthopedics department who offered continued conservative management, resection arthroplasty, or a high AKA. The vascular surgery department was consulted as the patient would likely undergo an AKA. She had a knee and femur X-ray to assist with preoperative planning, to further assess how high the amputation should be, with consideration to the existing hardware (Figures 4, 5). After evaluation of the imaging, it was felt that the amputation did not need to be higher than the femoral prosthetic component. During this time, a computer tomography (CT) without contrast of the left lower extremity was done to rule out an abscess of the soft tissue wound. The imaging was unremarkable for any sign of abscess.
Left knee exposed joint hardwareExposed left knee joint hardware following a non-healing wound.
Left posterior thigh pressure ulcerSuperficial pressure ulcer on the posterior thigh. This was taken after approximately 10 months of wound care management and antibiotics.
Left posterior thigh ulcerMagnified view of the pressure ulcer seen on the left posterior thigh.
Left knee X-rayThis X-ray highlights the components of the knee joint. The hinged knee joint prosthesis that inserts into the femur. A long stem prosthesis is seen in the tibia.
Left femur X-rayThis image shows how proximal the femoral hinge joint extends into the bone.
The decision-making process for this patient was complex and multifactorial. Both the patient and her family expressed concerns that the complications following her knee arthroplasty in 2013 have greatly limited her mobility and independence. Possible amputation had been previously discussed at length with the patient at prior office visits with multiple specialties. The vascular department had a discussion of a below-knee transection, as this would give the best results in terms of mobility, but this was complicated by the posterior left thigh soft tissue infection. A hip disarticulation would eliminate both sources of infection; however, it would greatly limit mobility as she would be unable to have a prosthetic. The orthopedics department had discussed a resection arthroplasty as she already had three revision surgeries, and the joint was unsalvageable. However, a resection arthroplasty would leave the leg with less support, affecting her quality of life and independence. She had undergone months of IV antibiotics to treat the pressure ulcer with the hope of providing healthy tissue to create an uncontaminated flap for an AKA. Despite antibiotic treatment and follow-up with infectious diseases, there was minimal clinical improvement. Due to her limited mobility and presence of infection, it was decided she would undergo an AKA, despite the high risk of wound infection during recovery.
The left AKA was completed alongside the orthopedic surgery team, who removed the prosthetic components. Intraoperative wound cultures from the left posterior infection revealed methicillin-resistant Staphylococcus aureus (MRSA). Due to the high risk for wound infection during closure, only the fascial layer was closed. It was decided that the skin would remain open and heal by secondary intention with a wound vacuum placed over the stump. Postoperatively, the stump was healing as expected, and appropriate antibiotics were continued. It was anticipated that her recovery would be complicated by the presence of remaining infection, and the healing process would be variable. On postoperative day 19, she underwent debridement and delayed primary closure of the stump with placement of incisional wound vacuum. She was then discharged to a subacute rehab facility on postoperative day 2 from her delayed closure. However, she was readmitted two days later for superficial wound dehiscence and underwent another debridement. Her wound culture grew MRSA, which was consistent with the intraoperative culture results. Her antibiotics were monitored by the infectious disease department. There was a discussion regarding another debridement in the operating room, but ultimately it was managed conservatively with the placement of a wound vacuum. She was then discharged on postoperative day 10 from her last operative debridement. Since her last discharge, she has not been readmitted for any acute infection.
Discussion
The most identified microbe in the setting of PJIs is coagulase-negative staphylococcus, specifically Staphylococcus epidermidis, followed by Staphylococcus aureus, enterococcus, and then gram-negative pathogens [7]. Pseudomonas is a less common microorganism of PJIs and is a challenging organism to treat and prevent [8]. This pathogen typically attaches to bone and fibrocartilaginous articular surfaces making osteomyelitis and septic arthritis a more common presentation compared to PJI [8]. The presence of Pseudomonas is more likely in patients with a history of diabetes mellitus, gastrointestinal or genitourinary surgery [8]. In this case, she has a complex history with multiple renal calculi requiring stents, cystoscopy, and lithotripsy, likely contributing to the presence of this microbe.
PJIs are a rare complication of arthroplasty with an incidence of 1-2% [9]. Treatment options are highly individualized and require a multi-disciplinary team to give the best outcome [10]. Common management of PJIs is antibiotic therapy alongside surgical options such as debridement and implant retention [10]. The surgical gold standard of treatment has been a two-stage exchange [11]. This involves removing the implant followed by IV antibiotics, placement of a temporary spacer, and then reimplantation of the components after the infection has cleared [11]. In some cases, depending on the patient’s comorbidities and presentations, a one-stage or one-and-a-half-stage exchange is becoming a more available treatment option [11]. In this case, the patient had undergone a two-stage revision following her initial PJI with aggressive antibiotics following the surgery. Table 1 illustrates the patient's entire clinical course in chronological order with associated treatment.
The patient’s care had been closely followed by multiple specialties to ensure proper management of her infections. However, she had undergone a series of revisions with minimal improvement to her quality of life. Multiple factors were considered before, during, and after surgery to give her the best chance of regaining some level of function and independence. These included (1) the patient’s personal goals regarding her ability to walk and regain some independence, (2) the necessity for a high transection at the thigh given the presence of hardware in the femur, (3) the presence of cellulitis within the tissue that would become the posterior flap after amputation, and (4) the presence of osteomyelitis at the knee joint, which could extend further into the femur than initially anticipated.
Conclusions
This case discusses the complicated clinical course of a female with significant comorbidities that ultimately underwent an AKA due to failed knee revisions secondary to the development of multiple PJIs. While there is a gold standard treatment for PJIs, it becomes less clear in the setting of multiple infections and can be highly variable depending on patient factors. Her clinical course required a multidisciplinary approach between infectious diseases, orthopedics, wound care, and the vascular team. It also discusses a unique and complex surgical and medical history. This case aims to add to existing literature about the treatment of complicated and recurrent PJIs as well as highlight a unique patient presentation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence of periprosthetic joint infection after primary total knee arthroplasty shows significant variation : a synthesis of meta-analysis and bibliometric analysis J Orthop Surg Res Ma T Jiao J Guo DW Lv SZ Zhang D Hou DC 6491920243939601510.1186/s 13018-024-05099-8PMC 11470562 · doi ↗ · pubmed ↗
- 2Incidence, microbiological studies, and factors associated with prosthetic joint infection after total knee arthroplasty JAMA Netw Open Weinstein EJ Stephens-Shields AJ Newcomb CW 06202310.1001/jamanetworkopen.2023.40457 PMC 1061884937906194 · doi ↗ · pubmed ↗
- 3Review of recent advances in the diagnosis and management of periprosthetic joint infection after total knee arthroplasty part 2: single-stage or two-stage surgical technique?J Orthop Surg Res Suliman J Warda H Samaan M 6431920243939598710.1186/s 13018-024-05152-6PMC 11470652 · doi ↗ · pubmed ↗
- 4Above-the-knee amputation versus knee arthrodesis for revision of infected total knee arthroplasty: Recurrent infection rates and functional outcomes of 43 patients at a mean follow-up of 6.7 years Orthop Traumatol Surg Res Trouillez T Faure PA Martinot P 10291410720213381209110.1016/j.otsr.2021.102914 · doi ↗ · pubmed ↗
- 5Above-knee amputation following chronically infected total knee arthroplasty: patient-reported satisfaction and functional outcomes J Arthroplasty Juryn MS Ekhtiari S Wolfstadt JI Backstein DJ 4864934020253917897110.1016/j.arth.2024.08.017 · doi ↗ · pubmed ↗
- 6Patient-reported outcomes after above-knee amputation for prosthetic joint infection Knee Orfanos AV Michael RJ Keeney BJ Moschetti WE 110111052720203180650710.1016/j.knee.2019.10.007 · doi ↗ · pubmed ↗
- 7Microbiological profiles of patients with periprosthetic joint infection of the hip or knee Diagnostics (Basel) Fröschen FS Randau TM Franz A Molitor E Hischebeth GT 16541220223588555810.3390/diagnostics 12071654 PMC 9316097 · doi ↗ · pubmed ↗
- 8Pseudomonas prosthetic joint infections: a review of 102 episodes J Bone Jt Infect Shah NB Osmon DR Steckelberg JM Sierra RJ Walker RC Tande AJ Berbari EF 2530120162852984910.7150/jbji.15722 PMC 5423557 · doi ↗ · pubmed ↗