How Acute Postoperative Pain Impacts Patient Satisfaction After Lower Limb Fracture Surgery: A 14-Day Follow-Up Study
Ayisha Sultana, Shyam Sunder, Velavan Anandan, Prince Solomon, Akash Deep

TL;DR
This study explores how pain after lower limb fracture surgery affects patient satisfaction over 14 days, finding that pain reduction alone doesn't fully explain satisfaction.
Contribution
The study reveals that patient satisfaction is more influenced by fixation type and communication than by pain levels alone.
Findings
Pain levels significantly decreased from 8.88 to 4.28 over 14 days.
Patient satisfaction increased from 1.7% to 89.7% by day 14.
Fixation type significantly affected satisfaction, but pain management methods did not.
Abstract
Background: Postoperative pain following lower limb fracture surgery is frequently severe, yet the correlation between this acute pain trajectory and patient satisfaction with care remains poorly understood. This study investigated whether effective early pain relief correlates directly with improved patient satisfaction within the first 14 postoperative days. Methodology: A prospective, longitudinal observational study was conducted on 58 adult patients undergoing surgical fixation for lower limb fractures. Pain levels (visual analog scale, VAS) and patient satisfaction (five-point Likert scale) were assessed at two timepoints: 48 hours and 14 days post-surgery. Results: Mean VAS scores demonstrated a significant reduction from 8.88 ± 0.87 at 48 hours to 4.28 ± 1.1 by day 14 (p value <0.001). Despite initial widespread dissatisfaction, with only one patient (1.7%) satisfied at 48…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
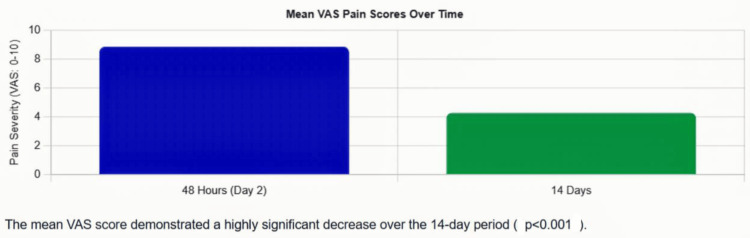 Figure 1
Figure 1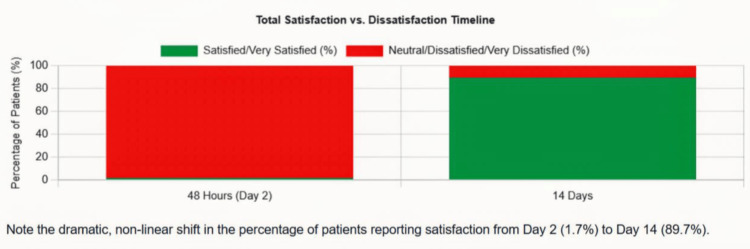 Figure 2
Figure 2| Demographic Variable | n (%) |
| Age (years) | |
| 20–40 | 13 (22.4) |
| 41–60 | 23 (39.6) |
| >60 | 22 (37.9) |
| Gender | |
| Male | 38 (65.5) |
| Female | 20 (34.5) |
| Occupational Status | |
| Unemployed | 11 (19.0) |
| Professional | 5 (8.6) |
| Skilled laborer | 15 (25.9) |
| Semi-skilled worker | 27 (46.6) |
| Educational Status | |
| No formal education | 4 (6.9) |
| Primary school | 17 (29.3) |
| Secondary school | 16 (27.6) |
| High school or beyond | 21 (36.2) |
| Monthly Household Income (Indian National Rupee) | |
| <10,000 | 21 (36.2) |
| 10,001–20,000 | 23 (39.7) |
| 20,001–30,000 | 12 (20.7) |
| >30,000 | 2 (3.4) |
| Characteristic | n (%) |
| Presence of Comorbid Illness | |
| Yes | 13 (22.4) |
| No | 45 (77.6) |
| Prior Surgical History | |
| Yes | 10 (17.2) |
| No | 48 (82.8) |
| Road traffic accident or fall | 51 (87.9) |
| Sports-related | 3 (5.2) |
| Occupational | 3 (5.2) |
| Other | 1 (1.7) |
| Type of Fixation Used | |
| Internal (plates, screws, nailing) | 42 (72.4) |
| External | 16 (27.6) |
| Anesthesia Type | |
| Regional (spinal/epidural) | 56 (96.6) |
| General | 2 (3.4) |
| Postoperative Analgesia Method | |
| Epidural catheter | 39 (67.2) |
| Intravenous analgesia | 19 (32.8) |
| Mobilization Status at Day 2 | |
| Immobilized | 10 (17.2) |
| Partial weight bearing | 43 (74.1) |
| Full weight bearing | 4 (6.9) |
| Non-weight bearing | 1 (1.7) |
| Outcome | Day 2 | Day 14 | p-value |
| Visual Analog Scale (VAS) Pain Score | |||
| Mean ± SD | 8.88 ± 0.87 | 4.28 ± 1.12 | p < 0.001 |
| Range | 6–10 | 2–6 | |
| Outcome | Day 2 | Day 14 |
| Patient Satisfaction Rating | ||
| Very satisfied | 0 (0%) | 19 (32.8%) |
| Satisfied | 1 (1.7%) | 33 (56.9%) |
| Neutral | 9 (15.5%) | 5 (8.6%) |
| Dissatisfied | 28 (48.3%) | 1 (1.7%) |
| Very dissatisfied | 20 (34.5%) | 0 (0%) |
| Combined Satisfied/Very Satisfied | 1 (1.7%) | 52 (89.7%) |
| Variable | Satisfied/Very Satisfied | Neutral/Dissatisfied | p-value |
| Type of Anesthesia | |||
| Regional | 51 (91.1%) | 5 (8.9%) | 0.198 |
| General | 1 (50.0%) | 1 (50.0%) | |
| Type of Analgesia | |||
| Epidural | 34 (87.2%) | 5 (12.8%) | 0.653 |
| Intravenous | 18 (94.7%) | 1 (5.3%) | |
| Type of Fixation | |||
| Internal | 40 (95.2%) | 2 (4.8%) | 0.043* |
| External | 12 (75.0%) | 4 (25.0%) | |
| Gender | |||
| Male | 33 (86.8%) | 5 (13.2%) | 0.653 |
| Female | 19 (95.0%) | 1 (5.0%) | |
| Age Group | |||
| 20–40 years | 11 (78.6%) | 3 (21.4%) | 0.067 |
| 41–60 years | 19 (90.5%) | 2 (9.5%) | |
| >60 years | 22 (95.7%) | 1 (4.3%) | |
| Parameter | VAS (48 hours) | VAS (14 days) |
| Patient Satisfaction Score | -0.132 | -0.125 |
| r=-0.132 | r=-0.125 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Music Therapy and Health · Pediatric Pain Management Techniques
Introduction
The experience of acute postoperative pain following fracture surgery is often perceived by patients as greater than anticipated. However, existing literature often fails to simultaneously explore this experience through the objective metric of pain severity and the subjective measure of patient satisfaction [1,2]. While a linear relationship between reduced pain and increased satisfaction is intuitively assumed, clinical practice demonstrates that patient satisfaction is a multifactorial construct. It is influenced by preoperative expectations, health literacy, and communication with the surgical team.
The distinction between the immediate (48 hours) and early recovery (two weeks) phases is critical, as patient priorities and levels of adaptation change during this period. At our institution, clinical observations suggested that patients managed with optimized regional anesthesia and multimodal pain regimens reported higher satisfaction, independent of standard confounding factors such as age or fixation method [3,4]. To rigorously examine this relationship, we prospectively measured pain trajectory and satisfaction in adult patients undergoing lower limb fracture fixation.
The objective of this study is to identify factors that impact patient satisfaction using the visual analog scale (VAS), a validated, subjective measure for acute and chronic pain [1], and Likert’s scale. Likert-type scales are frequently used in medical education and medical education research [5]. We hypothesized that the evolution of pain severity and patient satisfaction would be independent over the first 14 postoperative days and that the chosen anesthesia and analgesia strategy - rather than demographic or surgical variables - would be the dominant determinant of satisfaction outcomes.
Materials and methods
Study population and setting
Between May 2025 and June 2025, a cohort of 58 consecutive adults (aged ≥18 years) presenting with isolated lower limb fractures (femoral neck, intertrochanteric, femoral shaft, tibial, or ankle fractures) requiring operative fixation were enrolled. The study was conducted at the Department of Orthopaedics in a tertiary care centre in South India, serving both urban and rural populations.
Inclusion criteria comprised of adult patients (age ≥18 years) with isolated lower limb fractures (both open and closed) requiring operative fixation, the ability to provide informed consent, and the capacity to use standardized scales for pain and satisfaction assessment. Exclusion criteria were polytrauma or multiorgan injuries, documented psychiatric illness, neurological impairment affecting pain perception, and refusal to participate. The sample size was estimated for comparing paired VAS pain scores at 48 hours and 14 days after surgery. A change of 1.5 points on the 0-10 VAS was taken as clinically important based on postoperative pain studies [6]. With a two-sided α of 0.05, 90% power, and an assumed standard deviation of 2.5 points for the within-patient difference, the required sample size was 30 patients. Our study included 58 participants; the sample size was adequate to detect a clinically meaningful change in pain.
Data collection protocol
Structured face-to-face interviews were conducted by the research team on postoperative days 2 and 14 in the patient's room or clinic setting. Pain severity was quantified using the VAS, a 10 cm horizontal line scored from 0 ("no pain") to 10 ("worst pain imaginable"). We utilized a five-point Likert scale to assess three domains: satisfaction with pain relief effectiveness, overall satisfaction with the surgical experience, and confidence in recovery trajectory. The scale anchors were defined as 1 = Very Dissatisfied, 2 = Dissatisfied, 3 = Neutral, 4 = Satisfied, and 5 = Very Satisfied. Data collected included comorbid illnesses, previous surgeries, mode of injury, fracture site and type, operative approach, fixation method (internal vs. external), type of anesthesia (general vs. regional), and primary pain relief strategy (intravenous (IV) infusion vs. epidural catheter). The Institutional Ethics Committee of Pondicherry Institute of Medical Sciences granted approval for this study. Written informed consent was obtained from all participants prior to enrolment.
Statistical approach
Descriptive statistics were calculated as frequencies, percentages, means, and standard deviations. The change in continuous pain scores between days 2 and 14 was assessed using a paired t-test. The association between categorical variables and satisfaction at day 14 was analyzed using the chi-square test or Fisher's exact test, where cell counts were small. Statistical significance was defined as a two-tailed test (p < 0.05).
Results
Sample characteristics
The cohort comprised 58 patients (38 male, 20 female) with a mean age of 50.2 ± 14.8 years. The majority were semi-skilled (46.6%) or skilled labourers (25.9%). Road traffic accidents accounted for 87.9% of the injury mechanisms. See Table 1 for the baseline demographic characteristics.
Clinical and operative characteristics
The majority of patients (72.4% underwent internal fixation. Regional anesthesia (spinal or epidural) was administered to 96.6% of the cohort. For primary pain management, 67.2% received epidural catheters, while 32.8% were managed with IV analgesia alone. See Table 2 for the clinical and operative characteristics.
Pain severity trajectory
On postoperative day two, the mean VAS was 8.88 ± 0.87. By day 14, the mean VAS had decreased substantially to 4.28 ± 1.12, representing a reduction of 4.60 points. This reduction was statistically highly significant (p < 0.001, paired t-test). See Figure 1 for the mean VAS pain scores at 48 hours and 14 days, and Table 3 for the VAS pain score at 48 hours and 14 days.
Mean visual analog scale (VAS) pain scores at 48 hours and 14 daysThe chart shows a clear decline in pain from 8.88/10 at 48 hours to 4.28/10 at 14 days, with error bars representing standard deviation. The trajectory illustrates the typical postoperative pain resolution pattern (p value <0.001)
Table 3: Visual analog scale (VAS) pain score at 48 hours and 14 daysThis reduction in VAS score was statistically highly significant (p<0.001, paired t-test).
Patient satisfaction over time
At 48 hours, only one patient (1.7%) reported satisfaction with pain relief, with 82.8% reporting dissatisfaction. The overall satisfaction with the surgical experience was similarly low. At 14 days, a near-complete reversal was observed, with 52 patients (89.7%) reporting satisfaction or marked satisfaction with pain relief and overall surgical experience. See Figure 2 for the distribution of patient satisfaction ratings at 48 hours vs. 14 days, and Table 4 for the patient satisfaction at 48 hours and 14 days.
Distribution of patient satisfaction ratings at 48 hours vs. 14 daysA stacked bar chart illustrates the dramatic shift in satisfaction: at 48 hours, approximately 82.8% express dissatisfaction, with only 1.7% satisfied. By day 14, the pattern inverts, with 89.7% satisfied and dissatisfaction dropping to 1.7%.
Predictors of patient satisfaction at day 14
Patients who received regional anesthesia (n=56) reported similar satisfaction rates compared to those receiving general anesthesia (n=2) (p value=0.198). However, this finding must be interpreted with extreme caution due to the very small sample size (n=2) in the general anesthesia group.
The type of analgesia also showed no significant statistical association with patient satisfaction (p=0.653). Meanwhile, both methods resulted in high overall satisfaction - 87.2% for epidural analgesia (n=34) and 94.7% for IV analgesia (n=18). This confirms that the choice of primary analgesic modality is not a strong predictor of the final satisfaction outcome. The observed trend of higher satisfaction in the IV group is noteworthy, potentially reflecting the avoidance of catheter-related complications sometimes associated with epidural use. Demographic and other clinical factors, such as age, gender, income, and education level, were not found to be statistically significant predictors of satisfaction at day 14. There was a significant statistical association between patient satisfaction and the type of fixation. Univariate analysis showed a significant satisfaction in patients who underwent internal fixation compared to the external fixation group (p value=0.043, statistically significant). See Table 5 for the univariate predictors of satisfaction.
Table 5: Univariate predictors of patient satisfaction at day 14*Statistically significant (p<0.05). The association between categorical variables and satisfaction at day 14 was analysed using Fisher's exact test.
Additionally, the calculation of the correlation coefficient between the VAS score (at 48 hours and 14 days ) and patient satisfaction score was done. The results showed a negative correlation between the VAS score and patient satisfaction score. See Table 6 for the correlation between VAS score and patient satisfaction score.
Discussion
Pain is a highly subjective entity. Postoperative pain is acute pain due to surgical trauma with an inflammatory response and initiation of an afferent neuronal barrage that results in several unpleasant sensory, emotional, and psychological burdens. Patient satisfaction is a subjective measurement influenced by many variables and may be difficult to interpret.
The pain-satisfaction disparity
Our results underscore a significant disparity: severe pain at 48 hours did not predict low satisfaction at day 14. Furthermore, the 52% reduction in pain scores was disproportionate to the 88%-point surge in satisfaction. This phenomenon strongly suggests that satisfaction is not merely a consequence of pain relief but is heavily mediated by psychological adaptation, the achievement of early functional milestones, and the clarity of patient-provider communication. The initial high pain is an expected component of orthopaedic trauma recovery; however, the subsequent recovery trajectory allows non-pharmacological factors to influence the overall experience. Literature reviews shows strong association between patient satisfaction and postoperative pain scores [7], and optimizing postoperative pain management is a potential opportunity to satisfy the patient.
The role of anesthesia and analgesia
Literature evidence suggests that regional anesthesia was significantly associated with higher satisfaction as per established anesthetic guidelines. Regional techniques offer advantages such as reduced postoperative nausea/vomiting [8,9], faster cognitive recovery, and a superior patient-perceived pain control profile [10]. However, in our study, no significant association was found (p=0.198). This must be interpreted cautiously due to the minimal number of patients who received general anesthesia (n=2).
The statistically insignificant difference observed in satisfaction based on the analgesia method (p=0.653) suggests a delicate balance in pain management strategy. While epidural analgesia often provides superior numeric pain control, its use carries inherent risks of complications (e.g., urinary retention). Our data suggest that, for some patients, the avoidance of these complications via a well-managed IV analgesic regimen may translate into comparable or even higher satisfaction (as seen in the 94.7% satisfaction rate), despite potentially less aggressive numeric pain control. This emphasizes that patient comfort and complication avoidance are critical drivers of satisfaction, potentially outweighing the benefit of absolute zero pain.
Importance of expectation management and communication
Qualitative synthesis of patient remarks highlighted that initial dissatisfaction (day two) was often rooted in uncertainty - specifically a lack of clarity regarding expected pain severity and the recovery timeline. Studies show that pain sensations are enhanced by negative emotions [11,12]. The dramatic improvement in satisfaction by day 14 is likely a function of patients receiving repeated information, their expectations normalizing, and the commencement of tangible functional gains (e.g., initial mobilization). This supports the growing body of literature that emphasizes the crucial role of information provision, care team responsiveness, and the congruence between expected and experienced reality in determining patient contentment. Future interventions should therefore focus on standardized, timely patient education rather than relying solely on pharmacological interventions.
Demography, socioeconomic status, and satisfaction
The lack of association between satisfaction and demographic factors (age, income, education) is a powerful finding. Literature evidence shows varying results in relation to demographic parameters, as few studies showed that older age groups show higher satisfaction rates than younger age groups [13-15], whereas few studies show no significant association between age and patient satisfaction [7]. This indicates that, in our setting, where standardized surgical and pain management protocols were applied, the quality of care transcended socioeconomic stratification. This reinforces the principle that excellent clinical care, delivered with effective communication, is the universal driver of positive patient experience.
Type of fixation and satisfaction
The only significant factor having a statistically significant association with patient satisfaction was the type of fixation. Forty out of 42 patients who underwent internal fixation (n=40, 95.2%) reported better satisfaction rates than those who underwent external fixation (12 out of 16, 75%). Even though this is a statistically significant association, this needs to be analyzed with caution, as the patients who underwent external fixation were having open fractures, which inherently can cause more dissatisfaction because of the need for multiple surgeries, regular dressings, and the presence of heavy, not-so-aesthetic implants visible outside their bodies. Traditionally, too many external fixators are considered cumbersome by patients because of potential discomfort, restricted mobility, and prolonged care of pins, even though they are an excellent tool in the setting of open fracture treatment [16,17].
Study limitations
The study's findings are subject to several limitations, including the single-center design (limiting generalizability), a small sample size (n=58), which limits statistical power for complex subgroup analysis, and the reliance on subjective scales, which are prone to recall and response biases. Critically, the analysis of the type of fixation is severely limited by the small sample size in the external fixation group (16 in external fixation compared to 42 in internal fixation) and variability in the fracture prolife. Open fractures, which were treated by external fixation, are inherently a cause for poor satisfaction because of other factors discussed above. Furthermore, the brief 14-day follow-up period does not capture long-term satisfaction associated with functional recovery milestones.
Conclusions
Our study failed to find an association between anesthesia/analgesia and patient satisfaction, likely due to underpowering/selection bias. The association between the type of fixation and patient satisfaction, even though statistically significant, needs detailed analysis to remove the confounding effect because of underlying fracture severity. This suggests that the complexity and sequelae of the initial trauma are key drivers of long-term patient dissatisfaction, not the choice of anesthesia/analgesia. Moreover, perioperative patient communication, effective expectation management, and optimizing regional pain control protocols are the principal drivers of a positive patient experience. Orthopaedic units should focus on these structural elements to enhance adherence to rehabilitation, improve functional outcomes, and build community trust.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Patient satisfaction with post-operative pain management and associated factors among surgical patients at Tikur Anbessa Specialized Hospital: cross-sectional study Ann Med Surg (Lond) Buli B Gashaw A Gebeyehu G Abrar M Gerbessa B 1040877920223586006210.1016/j.amsu.2022.104087 PMC 9289483 · doi ↗ · pubmed ↗
- 2Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey Curr Med Res Opin Gan TJ Habib AS Miller TE White W Apfelbaum JL 1491603020142423700410.1185/03007995.2013.860019 · doi ↗ · pubmed ↗
- 3The value of "multimodal" or "balanced analgesia" in postoperative pain treatment Anesth Analg Kehlet H Dahl JB 10481056771993810572410.1213/00000539-199311000-00030 · doi ↗ · pubmed ↗
- 4Practice guidelines for acute pain management in the perioperative setting: an updated report by the American Society of Anesthesiologists Task Force on Acute Pain Management Anesthesiology Apfelbaum JL Ashburn MA Connis RT 24827311620122222778910.1097/ALN.0b 013e 31823 c 1030 · doi ↗ · pubmed ↗
- 5Analyzing and interpreting data from Likert-type scales J Grad Med Educ Sullivan GM Artino AR Jr 541542520132445499510.4300/JGME-5-4-18PMC 3886444 · doi ↗ · pubmed ↗
- 6Establishing the minimal clinically important difference and substantial clinical benefit for the pain visual analog scale in a postoperative hand surgery population J Hand Surg Am Randall DJ Zhang Y Li H Hubbard JC Kazmers NH 6456534720223564474210.1016/j.jhsa.2022.03.009PMC 9271584 · doi ↗ · pubmed ↗
- 7Early patient satisfaction following orthopaedic surgery J Clin Orthop Trauma Howard B Aneizi A Nadarajah V 0811202010.1016/j.jcot.2020.06.037PMC 750313432999563 · doi ↗ · pubmed ↗
- 8Comparing regional anesthesia and general anesthesia for postoperative pain control in abdominal surgeries: a systematic review and meta-analysis Cureus Alshebly AA Alhwaiti AS Bahamdan O 017202510.7759/cureus.90483 PMC 1244524540978983 · doi ↗ · pubmed ↗