Case Report of Overlapping Pubic Symphysis Dislocation Managed Nonoperatively
Majed S Alasbali, Mohammed S Alghamdi, Bader F Alsubie, Abdalaziz F Alamer, Abdullah M Alrafee

TL;DR
A rare pelvic injury case was successfully treated without surgery, showing that nonoperative methods can work in specific situations.
Contribution
This case report demonstrates the successful nonoperative management of overlapping pubic symphysis dislocation.
Findings
Manual reduction under anesthesia successfully treated the patient's overlapping pubic symphysis dislocation.
The patient showed no complications or pelvic instability after 18 weeks of non-weight-bearing and gradual mobilization.
Nonoperative management can be a viable alternative when there is no urethral injury or posterior pelvic ring disruption.
Abstract
Overlapping pubic symphysis dislocation (OPSD) is a rare form of pelvic injury typically caused by high-energy lateral compression forces, resulting in the entrapment of the pubic body against or behind the contralateral pubic ramus. The majority of reported cases have required open reduction and internal fixation due to the mechanical complexity of the injury. However, less invasive management strategies may be feasible in select cases. We present a case of a 56-year-old male with diabetes who sustained an OPSD associated with a right sacral ala fracture, along with multiple nondisplaced rib and lumbar spine fractures, following blunt trauma. Urological evaluation, including CT urogram and ascending urethrogram, confirmed no bladder or urethral injury. Given the absence of posterior instability and urethral injury, this specific patient was managed conservatively under general…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
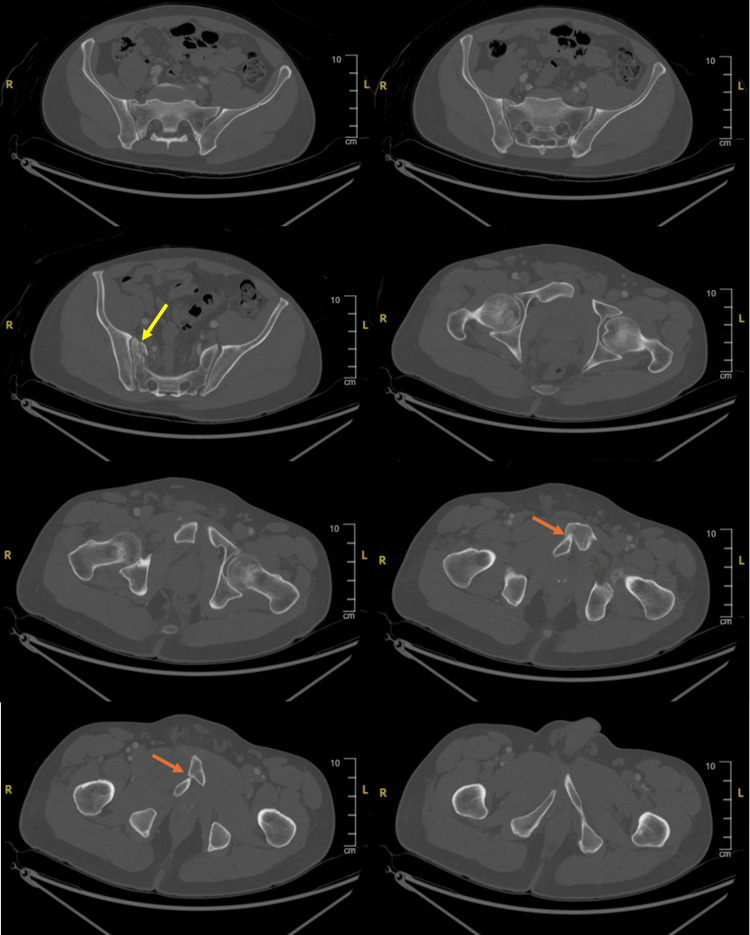 Figure 1
Figure 1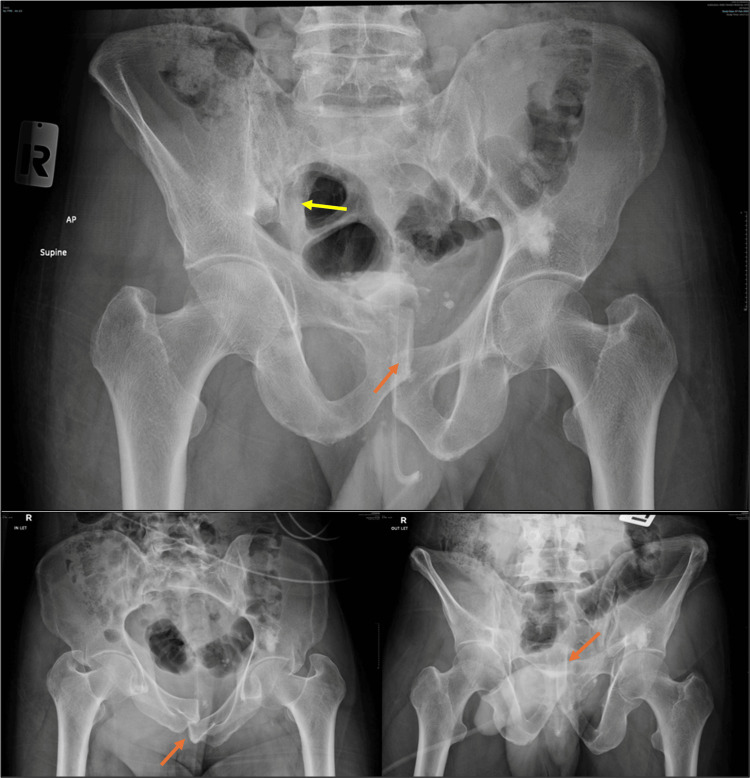 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6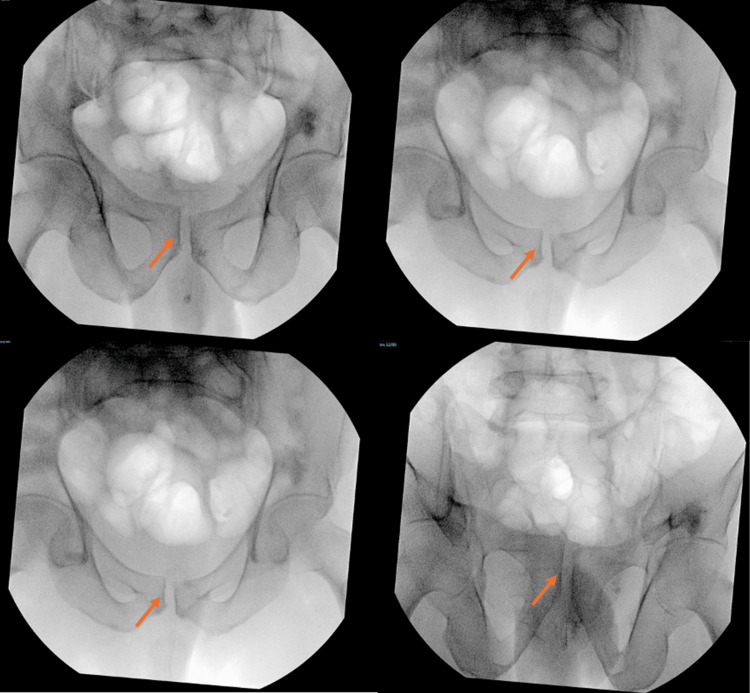 Figure 7
Figure 7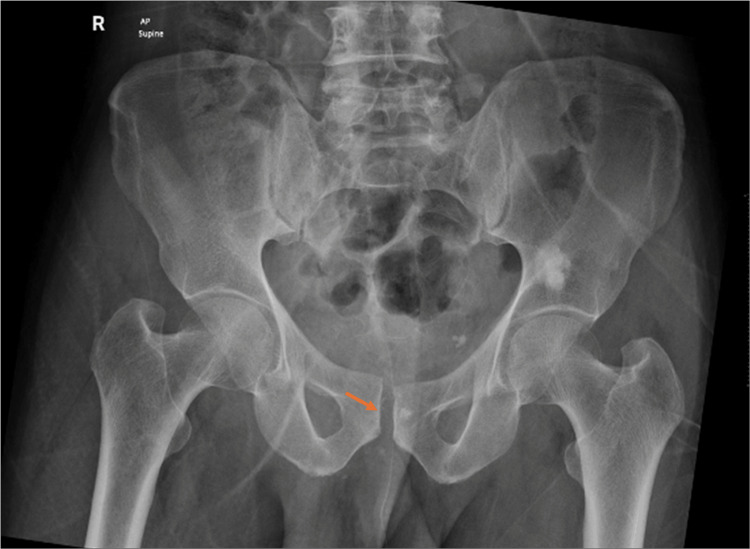 Figure 8
Figure 8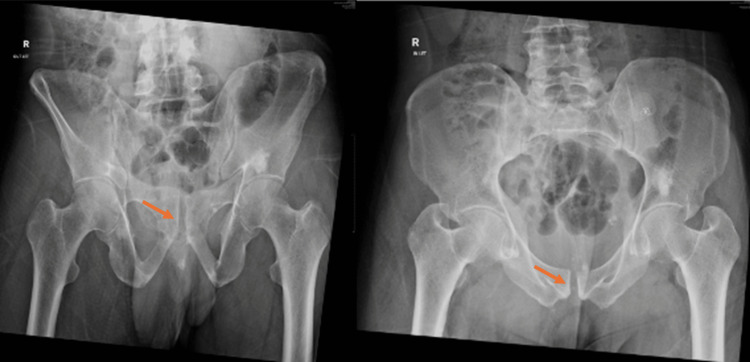 Figure 9
Figure 9 Figure 10
Figure 10 Figure 11
Figure 11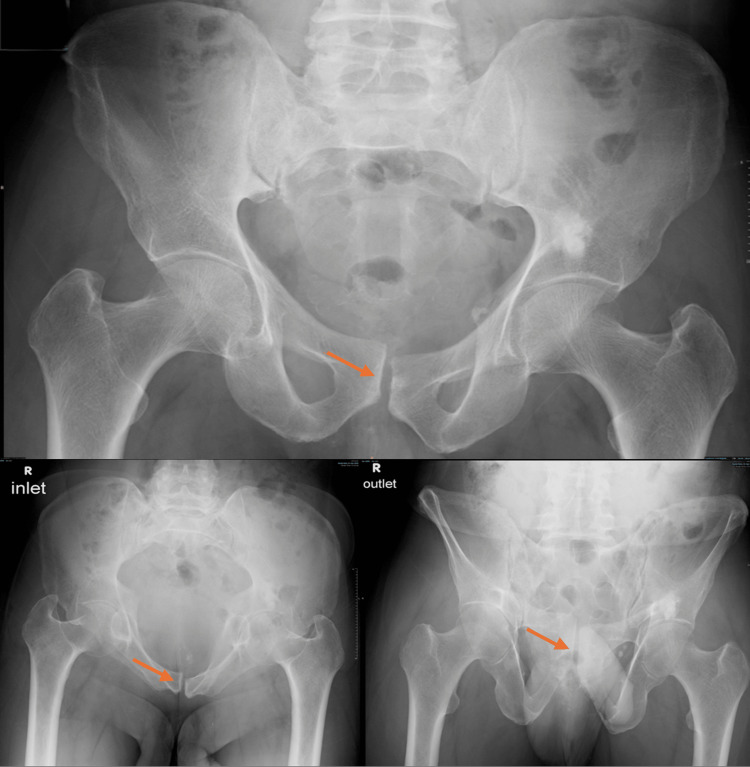 Figure 12
Figure 12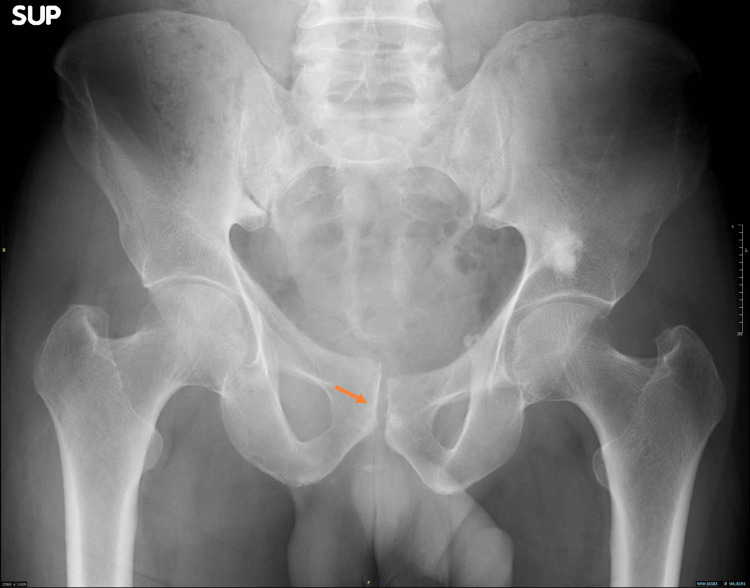 Figure 13
Figure 13Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic and Acetabular Injuries · Sports injuries and prevention · Urological Disorders and Treatments
Introduction
Locked symphysis pubis, or overlapping pubic symphysis dislocation (OPSD), is an infrequent type of pelvic injury due to lateral compression on the pelvic ring [1,2], causing the pubic body to displace and become entrapped against the contralateral side [2,3] or within the obturator foramen [1,3], resembling Tile classification B2.
It was first reported by Eggers in 1952 [4]. It is an uncommon injury and usually due to blunt trauma with hyperextension, adduction, and internal rotation, which result in pubic symphysis displacement anterior or posterior to the contralateral hemipelvis. In the literature, most cases were managed operatively with open reduction and internal fixation, but in our case, the injury was managed successfully with a manual reduction maneuver without surgical intervention.
Although most reported OPSD cases require open reduction, we aim to demonstrate that closed reduction may suffice in select patients without posterior ring instability or urethral injury. We present our case to describe the less invasive method for the reduction of OPSD, where we rely only on the manual technique, sparing the patient's need for invasive surgical intervention and instrumentation, thus decreasing soft tissue injury and pain.
Case presentation
A 56-year-old male with diabetes mellitus presented to the Emergency Department of King Fahad Medical City with complaints of pubic pain, right buttock pain, and inability to bear weight after a heavy metal door fell on him. He sustained an overlapping pubic symphysis dislocation associated with a comminuted right sacral ala fracture (zone 1) according to the Denis classification system, with an intact neurological exam and preserved distal pulses. Upon urological assessment, there was no distended bladder and no blood at the meatus. A computed tomography urogram protocol showed no extravasation from the bladder, and a follow-up retrograde urethrogram demonstrated a well-distended bladder with no extravasation. The patient had multiple nondisplaced rib fractures on the right side involving the second, fourth, and fifth ribs, and on the left side involving the fourth, fifth, sixth, and seventh ribs. Additionally, there were lumbar spine fractures at L1 and L4, both of which were managed conservatively. Similarly, the pre-procedural assessment of the radiographic images showed a right sacral ala fracture with overlapping pubic symphysis dislocation (Figures 1-2).
Pre-procedural axial CT scan showing overlapping pubic symphysis dislocation with entrapment of the pubic body and a comminuted right sacral ala fracture.The yellow arrow indicates the sacral injury. The orange arrow indicates the pubic injury.CT, computed tomography
Pre-procedural AP, inlet, and outlet radiographs showing a right sacral ala fracture with overlapping pubic symphysis dislocation.The yellow arrow indicates the sacral injury. The orange arrow indicates the pubic injury.AP, anteroposterior
On day 2 post-trauma, the patient was taken to the operating room, positioned supine on a Jackson table, and, after induction of general anesthesia, a closed reduction maneuver was attempted by flexion, abduction, and external rotation of both hips while applying anterior and outward pressure with two hands over the bilateral anterior superior iliac spines, while the assistant palpated the pubic symphysis to assess the reduction, as shown in Figures 3-6. With C-arm fluoroscopy guidance, a closed reduction was achieved (Figure 7).
Sequential intraoperative photograph showing the closed reduction technique performed with both hips held in flexion and external rotation.
Sequential intraoperative photograph showing the closed reduction technique performed while maintaining hip abduction.
Sequential intraoperative photograph showing the closed reduction technique, performed with combined anterior and outward pressure over the iliac bone, resulting in successful reduction.
Sequential intraoperative photograph showing the closed reduction technique, with palpation of the pubic symphysis and application of pressure to assess the reduction.
Intraoperative AP, inlet, and outlet fluoroscopic images showing realignment of the pubic symphysis.AP, anteroposterior
X-rays showed an acceptable reduction in anteroposterior (AP), inlet, and outlet views (Figures 8-9).
Post-reduction AP radiograph showing the reduced pubic symphysis.AP, anteroposterior
Post-reduction inlet and outlet radiographs confirming satisfactory reduction and alignment.
On the second day after reduction, weight-bearing radiographs showed a stable pelvis (Figure 10).
Weight-bearing X-ray confirms pelvic stability, reinforcing the clinical relevance of early mobilization.Radiograph shows a stable pelvis with maintained alignment on the second day after reduction.AP, anteroposterior
Postoperatively, the patient was managed with multimodal analgesia and physiotherapy focusing on functional transfer training, bed mobility, and strict non-weight-bearing for six weeks. At six weeks follow-up, he was allowed weight-bearing as tolerated. Follow-up evaluations at 6, 10, and 18 weeks with radiographs revealed maintained reduction (Figures 11-13). The patient reported no anterior or posterior pelvic pain and returned to his activities of daily living. He denied any symptoms of urinary dysfunction, confirming a favorable functional outcome.
Serial follow-up pelvic radiographs after six weeks demonstrating maintained reduction, with an AP view showing stable alignment of the pubic symphysis.AP, anteroposterior
Serial follow-up pelvic radiographs after 10 weeks demonstrating maintained reduction in AP, inlet, and outlet views.AP, anteroposterior
Serial follow-up pelvic radiographs after 18 weeks demonstrating maintained reduction in AP view.AP, anteroposterior
Discussion
OPSD is a rare and complex pelvic injury resulting from high-energy lateral compression forces. It typically involves the pubic body of one hemipelvis becoming entrapped against or behind the contralateral pubic ramus, or within the obturator foramen [2,4,5]. First described by Eggers in 1952, OPSD remains an uncommon entity, with only a limited number of cases reported in the literature [4].
Our case is notable for the successful closed manual reduction of an OPSD with an associated sacral ala fracture, managed without open surgery or internal fixation. Understanding the injury’s biomechanism, specifically how lateral compression entraps the pubic symphysis, enabled us to achieve reduction by reversing this mechanism. Our maneuver employed flexion, abduction, and external rotation to generate a lateral distraction force on the hemipelvis, combined with direct anterior pressure to disengage the entrapped symphysis. This conservative approach contrasts with the majority of published cases, in which surgical intervention was necessary due to the mechanical complexity of the injury or associated complications.
For instance, Chee and Ahmad reported a locked symphysis associated with iliac wing and femoral shaft fractures that required open reduction and internal fixation via an anterior pubic symphysis approach [2]. Likewise, Tadros et al. reported three cases of OPSD, each involving varying posterior pelvic injuries, all of which required open reduction and internal fixation [5].
In some reported severe cases, osteotomy of the contralateral superior pubic ramus was required for reduction when closed and standard open techniques failed. Rajput et al. and Basu et al. presented cases in which osteotomy was required to release the irreducible locked pubic ramus. However, long-term complications such as urethral stricture, sexual dysfunction, heterotopic ossification, and implant failure were noted, raising concerns about the morbidity associated with such invasive procedures [6, 3].
Pushpasekaran et al. used a distraction osteotomy in an 18-year-old patient and achieved mechanical realignment, although the patient developed a urethral stricture requiring later repair [7]. Similarly, Tsehaye and Teklu described an open approach in the setting of a concurrent acetabular fracture, again emphasizing the need for open reduction internal fixation in more complex injury patterns [8].
There is limited but important support in the literature for non-surgical management. Afshar and Koushkzari reported a case in which closed reduction under general anesthesia was sufficient, although the patient later had persistent urological complications due to urethral transection, so even nonoperative management is not without risk of further injury [1]. Notably, our patient had no signs of urethral or bladder injury on CT urogram or ascending urethrogram, and post-reduction follow-up demonstrated stable alignment with no complications or signs of pelvic instability.
Fergany et al. also emphasized the role of soft tissue entrapment as a cause of failed reduction [9]. However, their case required surgical bladder dissection, highlighting the importance of urological evaluation before attempting reduction, which was adequately addressed in our workup. A favorable outcome was noted in this case after reduction, as pain decreased, gait normalized, and the patient was able to return to work with normal urological function.
Conclusions
Our patient benefited from a well-executed closed reduction maneuver under fluoroscopic guidance. The technique involved flexion, abduction, and external rotation of the hips while applying anterior and outward pressure over the bilateral anterior superior iliac spines. This avoided the risk of surgical exposure and its potential risks like infection, iatrogenic injury, and prolonged hospitalization. Post-reduction management with non-weight-bearing followed by gradual mobilization resulted in favorable early outcomes.
This case shows that closed reduction can be a viable and safe alternative in selected cases of OPSD, particularly when there is no entrapment in the obturator canal, no urethral injury, and no complex posterior ring instability, confirming radiologic and functional stability up to 18 weeks. The key elements for success include adequate imaging to rule out soft tissue incarceration, prompt reduction under anesthesia, and proper follow-up. Hence, this case underscores that fluoroscopy-guided closed reduction may provide a safe and effective management option in OPSD when careful selection and imaging evaluation are performed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Overlapped pubic symphysis: a case report and review of the literature Arch Bone Jt Surg Afshar A Koushkzari M 21221632015 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4507077/ 26213708 PMC 4507077 · pubmed ↗
- 2Locked pubic symphysis: a case report and review of literature JUMMEC Chee WH Ahmad AR 5961212018 https://jummec.um.edu.my/index.php/jummec/article/view/15634
- 3Mid-term follow-up of superior pubic ramus osteotomy in locked symphysis pubis with urethral injury: a case report Chin J Traumatol Basu A Shukla N Velagada S Behera S 2442482620233399251310.1016/j.cjtee.2021.03.008PMC 10388251 · doi ↗ · pubmed ↗
- 4Dislocations of the os coxae Am J Surg Eggers GWN 3003078319521490338210.1016/0002-9610(52)90261-4 · doi ↗ · pubmed ↗
- 5Overlapping dislocation of the pubic symphysis: report of three cases and review of the literature Arch Orthop Trauma Surg Tadros AM Lunsjo K O'Brien P 67968312920091916549310.1007/s 00402-009-0813-0 · doi ↗ · pubmed ↗
- 6Irreducible overlapping pubic symphysis dislocation managed with distraction osteotomy of the contralateral superior pubic ramus: a rare case report J Orthop Case Rep Rajput R Pal KK Goel AK Mandal A 535611202110.13107/jocr.2021.v 11.i 07.2314 PMC 857676334790604 · doi ↗ · pubmed ↗
- 7Treatment of locked pubic symphysis by distraction osteotomy of the superior pubic ramus: a case report JBJS Case Connect Pushpasekaran N Thampy S Khaleel VM Joseph S 010202010.2106/JBJS.CC.19.0019632649101 · doi ↗ · pubmed ↗
- 8Case report on locked pubic symphysis with concomitant ipsilateral acetabular fracture Int Med Case Rep J Tsehaye M Teklu D 7437471420213473765210.2147/IMCRJ.S 316296 PMC 8560322 · doi ↗ · pubmed ↗