Isolated Vertigo as an Early Sign of Anti-GQ1b-Positive Miller Fisher Syndrome: Expanding the Spectrum
Noor Widyani Ahmad Shahaime, Mazaya Mahmud, Othmaliza Othman, Wan Haslina Wan Abdul Halim

TL;DR
A rare case of Miller Fisher Syndrome presented with isolated vertigo before typical symptoms, highlighting the need for careful neurological exams.
Contribution
This case expands the known spectrum of anti-GQ1b-positive Miller Fisher Syndrome by presenting isolated vertigo as an early sign.
Findings
Isolated vertigo can precede typical MFS symptoms like ophthalmoplegia and ataxia.
Anti-GQ1b antibody testing confirmed the diagnosis in this patient.
Early treatment with IVIG led to full recovery within six weeks.
Abstract
Miller Fisher syndrome (MFS) occupies a distinct corner of Guillain-Barré syndrome (GBS), typically presenting with a triad comprising ophthalmoplegia, ataxia, and areflexia. While diplopia and limb incoordination are typically early features, isolated vertigo as a prodromal symptom is exceedingly uncommon and often misdiagnosed as benign vestibular disease. We report a 56-year-old Malay man who presented twice to the emergency department with acute, continuous vertigo and was initially treated symptomatically before subsequently developing bilateral ophthalmoplegia and ataxia. Anti-ganglioside (anti-GQ1b) antibody testing was positive, confirming the diagnosis of MFS, and electrophysiological studies revealed early GBS-spectrum changes. The patient responded well to intravenous immunoglobulin (IVIG) and made a full recovery within six weeks. This case illustrates that vestibular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1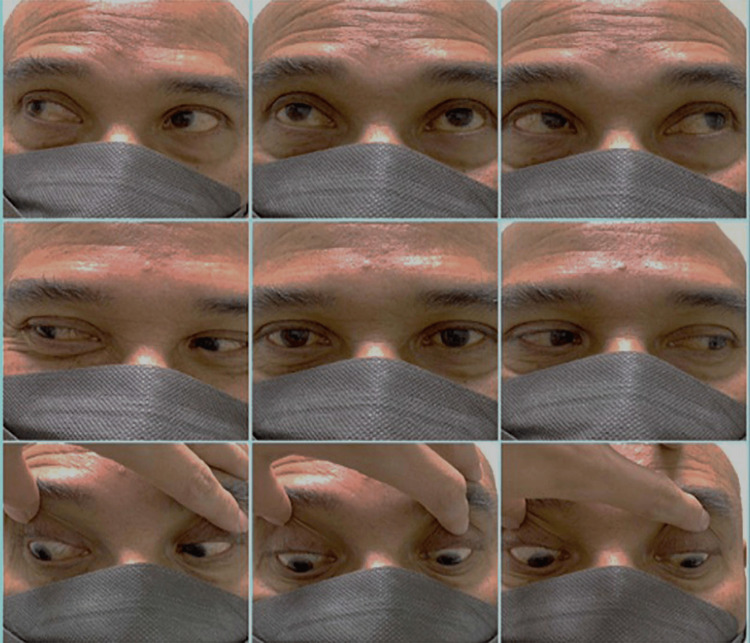 Figure 2
Figure 2| Condition | Typical presentation | Key ocular/neurological features | Investigations/ancillary tests | Red flags/distinguishing features |
| Miller Fisher Syndrome | Ophthalmoplegia, ataxia, areflexia, may begin with vertigo | Areflexia with preserved limb power, ophthalmoplegia | NCS (may show sensory-predominant changes), anti-GQ1b serology | Progression beyond the isolated vertigo, evolving new neuro-ophthalmic features |
| Posterior Circulation Stroke | Continuous vertigo, vomiting, gait instability | Direction-changing gaze-evoked nystagmus | HINTS, MRI brain with DWI, vascular work-up | Sudden onset, notable vascular risk factors, abnormal HINTS |
| Space Occupying Lesion (Posterior Fossa Tumor bleeding/Herniation) | Sudden vertigo, vomiting, altered mental consciousness | Progressive focal cranial nerve deficits, variable ocular motor palsies/skew | HINTS, MRI brain/orbit with contrast | Progressive symptoms, features of raised intracranial pressure (e.g., headache, vomiting, papilledema) |
| Cardiac Arrhythmia | Episodic or persistent/presyncope dizziness (perceived as vertigo) ± palpitation | No nystagmus/neurological deficits | ECG, cardiac enzyme | Syncope, exertional episodes, irregular rhythm |
| BPPV/Vestibular Neuritis | Episodic positional (BPPV) or prolonged vertigo (neuritis) | No ophthalmoplegia or areflexia, normal limb strength | Dix-Hallpike (BPPV), caloric testing, vHIT | Triggered by movement of the head (BPPV), normal pupils, no diplopia, no limb weakness |
| Electrolyte Imbalance/Endocrine Disturbances/Drug Toxicity | Dizziness, oscillopsia, confusion, tremor | Non-specific | Glucose, electrolytes, thyroid panel, Selective drug levels | Linked to medication or metabolic derangement, improves with correction or drug withdrawal |
| Myasthenia Gravis | Fluctuating ptosis/diplopia without ataxia or areflexia | Fatigability test positive, intact reflexes | Ice-pack test, RNS (signal decrement), AChR/MuSK antibodies | Worsening at evening or repetitive movement, reflexes preserved |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Long-Term Effects of COVID-19 · Autoimmune Neurological Disorders and Treatments
Introduction
Miller Fisher syndrome (MFS) represents a small but distinct subset within the Guillain-Barré syndrome (GBS) spectrum, a condition characterized by immune misrecognition. The condition was first described by Collier in 1932 and later defined by Fisher in 1956 as a complex comprising ophthalmoplegia, ataxia, and areflexia [1]. Although MFS is rare, the prevalence is higher in parts of Asia [2]. Such epidemiological differences are likely shaped by infectious exposures, underlying host susceptibility, and regional variation in diagnostic practice [3].
While the triad defines the syndrome, early manifestation may be subtle or incomplete. Isolated vertigo, in particular, can precede other neurological signs and lead to diagnostic uncertainty in acute care settings, where peripheral vestibular disorders are far more common. Recognizing this diagnostic pitfall is important, as vestibular involvement has increasingly been described across the expanding anti-GQ1b spectrum [4,5].
MFS typically follows an upper respiratory tract or gastrointestinal infection, and molecular mimicry between microbial antigens and neuronal ganglioside GQ1b triggers an autoimmune response that attacks the paranodal regions of ocular and vestibular nerves. This pathophysiological mechanism links the clinical involvement observed in MFS and its related anti-GQ1b spectrum [6,7].
We reported a rare case of anti-GQ1b-positive MFS that began with isolated vertigo, which later progressed to the full clinical triad. This case underscores the potential for early vestibular involvement within the anti-GQ1b spectrum and diagnostic pitfalls within the expanding anti-GQ1b spectrum.
Case presentation
A 56-year-old Malay man with well-controlled asthma presented with persistent vertigo for two weeks. The vertigo was described as a continuous spinning sensation that worsened with movement. There were no accompanying symptoms, such as diplopia, facial asymmetry, slurred speech, limb weakness, numbness, tinnitus, or hearing impairment. He denied any recent upper respiratory tract infection, gastrointestinal illness, fever, trauma, smoking, drug or alcohol use, and was not on any chronic medication.
He visited the emergency department twice during the initial two-week period. On both visits, he was hemodynamically stable, his pupils were reactive, and no nystagmus was observed. His symptoms improved with prochlorperazine and were treated as peripheral vertigo.
Approximately one week after his second visit, he noticed increasing unsteadiness. He reported difficulty detecting objects in his peripheral visual field unless he turned his head, although he denied having diplopia or blurred vision. Examination revealed complete external ophthalmoplegia (Figure 1), generalized areflexia, and broad-based ataxia. Limb strength was intact, and there were no signs of facial weakness, sensory deficit, or bulbar involvement.
Complete ophthalmoplegia at presentation.The patient was instructed to attempt upgaze, downgaze, left gaze, and right gaze, with very limited to almost no extraocular movement observed in any direction.
Initial laboratory investigations, including full blood count, renal profile, electrolytes, and glucose levels, were all within normal limits. Computed tomography of the brain (CT brain) showed no acute intracranial pathology. The patient was subsequently co-managed with the neurology team. Nerve conduction studies (NCS) showed normal distal motor and sensory conduction across the median, ulnar, peroneal, and sural nerves. However, H-reflexes were absent bilaterally, indicating early proximal demyelinating involvement, a common electrophysiological finding in the GBS spectrum. Serum anti-GQ1b antibody testing returned positive, confirming the diagnosis of MFS. He received IVIG (0.4g/kg/day) for five days. His reflexes improved during the admission, and his ophthalmoplegia (Figure 2) and ataxia were fully resolved by the six-week follow-up.
Resolution of ophthalmoplegia at six weeks.The patient demonstrated full extraocular movements in all gaze directions, consistent with complete recovery of ocular motility.
Discussion
Mechanistic bridge: Molecular mimicry and vestibulo-ocular vulnerability
The pathophysiological basis of MFS is well established and centers on the formation of anti-GQ1b IgG antibodies through molecular mimicry. Campylobacter jejuni is a well-recognised precursor infection in GBS, and its lipo-oligosaccharides share structural similarity with ganglioside GQ1b, providing the immunological link that drives antibody-mediated neuropathy [2,6]. The expression of GQ1b is highest in the ocular motor, vestibular, and proprioceptive fibres, making them vulnerable to damage. Antibodies bind to these paranodal regions, interfere with axonal conduction, and result in a range of characteristic clinical features observed across the spectrum. These features include symptoms such as ophthalmoplegia, ataxia, and areflexia. If the vestibular fibers are affected, vertigo or oscillopsia may emerge before other neurological signs [6,7].
While a preceding infection is often noted in classical cases, our patient did not have any prior infectious trigger. This is consistent with reports describing a subset of anti-GQ1b-positive patients without a clear antecedent infection, which contributes to the diagnostic challenges in identifying the spectrum in early presentations [6,8].
Isolated vertigo and early presentations within the anti-GQ1b spectrum
Patients with classical MFS typically present with ophthalmoplegia in nearly all cases, ataxia in 94%, and areflexia in approximately 90%. These symptoms usually emerge within the first one to four days [8]. In contrast, conditions within the anti-GQ1b spectrum may develop sequentially or remain incomplete, exhibiting a non-classical order depending on the initial site of antibody binding [4].
Although isolated vertigo is rarely highlighted in classical MFS studies, early ocular motor signs, such as nystagmus, have been documented, suggesting early vestibulo-ocular involvement [8]. Supporting this, Jung et al. described that atypical MFS initially presented with dizziness, imbalance, and gait unsteadiness, underscoring that vestibular pathways may have been affected way earlier than traditionally recognized [9]. While specific distributions of GQ1b in vestibular pathways are still not fully understood, clinical observations have consistently demonstrated that vestibular symptoms can manifest before the onset of more apparent neuro-ophthalmic symptoms in certain anti-GQ1-associated conditions [8-11]. This evidence expands the understanding of early presentations within the anti-GQ1b spectrum.
Recent research has further refined our understanding by grouping MFS, vestibular-predominant forms, Acute Ophthalmoparesis (AO), Bickerstaff Brainstem Encephalitis (BBE), and the overlap of MFS and GBS into a single, dynamic anti-GQ1b continuum [4,5]. In this spectrum, isolated vertigo may represent the earliest clinical manifestation, possibly appearing even before the hallmark triad of symptoms. Evidence from acute vestibular syndrome (AVS) studies further supports this notion, as patients who initially present with acute vertigo or dizziness often later develop ocular motor abnormalities [10]. Our patient followed this trajectory closely, experiencing two weeks of isolated vertigo before progressing to complete MFS. A similar vertigo-first onset has been described only once in a dedicated case report [11].
Recognizing persistent or unexplained vertigo as a possible early presentation within the anti-GQ1b spectrum reframes diagnostic expectations. This approach justifies repeated and comprehensive neurological and ophthalmic assessment and supports early anti-GQ1b testing when symptoms are evolving.
Differential diagnosis and diagnostic pitfalls
Vertigo as the initial and isolated symptom can mimic a wide range of conditions, particularly when ocular signs or areflexia have yet to emerge [12]. This was evident in our case, where the initial presentation closely resembled that of peripheral vestibular disease, which delayed consideration of MFS. The limited recognition of vertigo in MFS likely stems from the rare occurrence, as well as the common diagnostic approach used in acute care, where isolated vertigo is often attributed to peripheral vestibulopathies or posterior circulation strokes [13,14]. A structured evaluation is therefore essential to exclude other potential causes of emergency, before attributing symptoms to immune-mediated disorders. Peripheral vestibulopathies, such as benign paroxysmal positional vertigo (BPPV) or vestibular neuritis, are common, especially in older adults. Central causes, such as posterior circulation strokes or mass lesions, may present without apparent focal deficits and must be excluded first [13-15]. The HINTS (Head Impulse, Nystagmus, and Test of Skew) examination has been demonstrated to be more effective than early MRI in differentiating central and peripheral vertigo [13]. Moreover, neuromuscular and metabolic conditions such as myasthenia gravis, electrolyte imbalances, endocrine disturbances, and drug toxicity may also create overlapping neurology and ophthalmic features [12,15]. Table 1 summarizes the major differential diagnoses and their distinguishing features relevant in the acute setting.
In patients with persistent or unexplained vertigo, it is crucial to perform repeated neuro-ophthalmic examinations, as signs associated with the anti-GQ1b spectrum may evolve over time [4,9,10]. This approach increases the likelihood of identifying subtle signs that may appear before the classical triad.
Treatment and outcomes
Corticosteroids have shown no therapeutic benefit in GBS [16], and similarly, are not recommended for MFS given the shared immunopathological mechanism and guideline extrapolations [17]. First-line therapy for MFS remains IVIG or plasma exchange (PLEX), both of which exhibit comparable efficacy. IVIG is generally favored for its practicality in administration and overall tolerance. Spontaneous recovery can happen; however, early treatment is recommended when neurological deficits are functionally significant, progressive, or when diagnostic delay is expected, particularly in vestibular-predominant cases [16,17]. Emerging therapeutic approaches such as FcRn blockade, enzymatic IgG reduction, and complement inhibition are currently being explored for patients with severe or refractory disease [17].
Our patient achieved complete recovery by six weeks of IVIG, mirroring the excellent prognosis described in classical MFS [8], reinforcing the value of early recognition, timely referral, and prompt initiation of immunotherapy [16,17].
Conclusions
Persistent vertigo without peripheral vestibular features may, in rare instances, illustrate an early presentation of anti-GQ1b-positive MFS. This case highlights the need for comprehensive and repeated ophthalmology, neurology, and vestibular assessments when vertigo remains unexplained or evolves. Early anti-GQ1b testing can facilitate a timely diagnosis. Hence, recognizing these diverse presentations within the broader anti-GQ1b continuum enables prompt immunotherapy and favorable neurological recovery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An unusual variant of acute idiopathic polyneuritis (syndrome of ophthalmoplegia, ataxia and areflexia)N Engl J Med FIM 576525519561333479710.1056/NEJM 195607122550201 · doi ↗ · pubmed ↗
- 2Guillain-Barré syndrome Lancet Shahrizaila N Lehmann HC Kuwabara S 1214122839720213364723910.1016/S 0140-6736(21)00517-1 · doi ↗ · pubmed ↗
- 3Diagnosis of Guillain-Barré syndrome and validation of the Brighton criteria in Malaysia J Peripher Nerv Syst Tan CY Razali SN Goh KJ Shahrizaila N 2562642520203251181710.1111/jns.12398 · doi ↗ · pubmed ↗
- 4Clinical spectrum of the anti-GQ 1b antibody syndrome: a case series of eight patients Acta Neurol Belg de Bruyn A Poesen K Bossuyt X 293611920193074733610.1007/s 13760-019-01093-8 · doi ↗ · pubmed ↗
- 5Expanding horizons in anti-GQ 1b antibody syndrome: recognizing atypical and overlap forms J Ment Health Disord Noioso CM Pecoraro A Acerra GM 177952025
- 6Guillain-Barré syndrome Lancet Willison HJ Jacobs BC van Doorn PA 71772738820162694843510.1016/S 0140-6736(16)00339-1 · doi ↗ · pubmed ↗
- 7Guillain-Barré syndrome: expanding the concept of molecular mimicry Trends Immunol Laman JD Huizinga R Boons GJ Jacobs BC 2963084320223525627610.1016/j.it.2022.02.003PMC 9016725 · doi ↗ · pubmed ↗
- 8Clinical features and prognosis of Miller Fisher syndrome Neurology Mori M Kuwabara S Fukutake T Yuki N Hattori T 110411065620011132018810.1212/wnl.56.8.1104 · doi ↗ · pubmed ↗