The Ripple Effect: Applying Positive Psychology Principles in Debriefing to Transform Team Culture
David O Kessler, Jordyn Feingold, Rachel Elkin, Mirette Dube, Jennifer Reid

TL;DR
This paper explores how positive psychology can be used in healthcare debriefing to improve team culture and reduce burnout.
Contribution
The paper introduces practical strategies for integrating positive psychology into healthcare debriefing to foster well-being and positive workplace culture.
Findings
Positive psychology principles can shift healthcare workers' mindsets toward well-being and resilience.
Simulation programs can act as organizational nodes to spread positive effects across teams and departments.
Integrating positive psychology into debriefing supports clinician well-being and culture change.
Abstract
Healthcare is a complex system filled with high-stress and high-stakes situations that can put workers at risk for burnout and prime negative patterns of thinking. When an individual’s job entails constantly searching for problems or areas of improvement, as in medicine, they can become “stuck” in this paradigm, which may then spill over into social interactions and further compound negative workplace culture. Simulation programs can be effective levers for positive culture change, promoting a growth mindset, learning orientation, and culture of safety. The field of positive psychology can further enhance this by providing specific and explicit tools that help shift individual and team mindsets toward a more positive orientation attuned to what is working well and thereby promote cultures of well-being and resilience. The simulation’s position as an organizational node, with influence…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
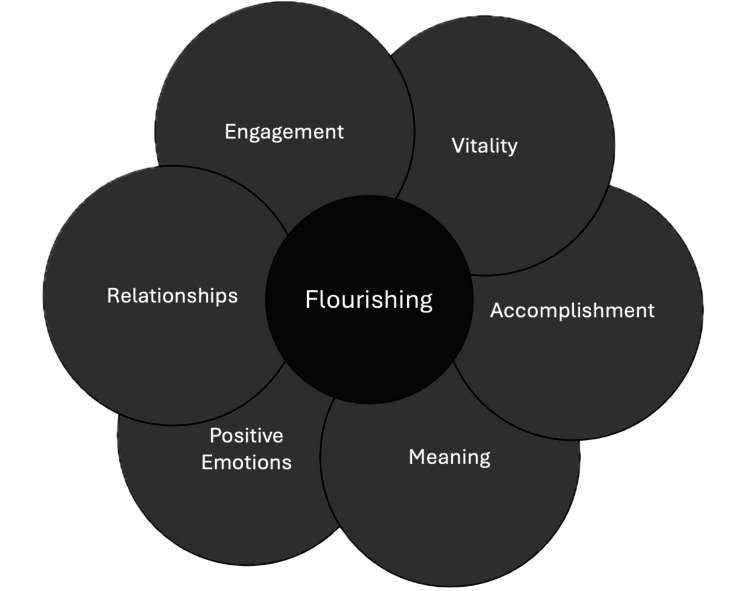 Figure 1
Figure 1| Positive psychology intervention | Description | Why it works |
| Gratitude exercises | Discuss three things that went well and why they happened | Encourages noticing positive events, builds positive emotions, counters negativity bias |
| Best possible self /future self visualization | Imagine what it would look like if everything went as well as possible | Builds optimism and engagement, links to meaning and goals |
| Use signature strengths in new ways | Identify and use top character strengths | Promotes a growth mindset, builds competence and self-efficacy through positive self-reflection |
| Acts of kindness | Perform intentional acts of kindness for others | Builds relational well-being, fosters teamwork |
| Savoring / positive experience recall | Intentionally notice, immerse in, and reflect on positive moments | Amplifies positive emotion, counters negativity bias, and strengthens memory for positive moments |
| Mindfulness | Intentionally slowing down, increase awareness of the present, notice with all senses, without judgement | Helps with emotional regulation, and bolsters engagement in the present moment |
| Meaning/values reflection | Reflecting on personal and shared mission, connecting to day-to-day tasks with one's larger sense of purpose in life | Enhances personal and relational engagement in daily life, improves motivation, self-transcendence |
| REVAMP category | Definition | Possible applications in the simulation | Examples |
| Relationships | The quality of social connection and trust between team members, perceived support from supervisors | Highlight examples of high-quality teamwork, trust, and collaboration during pre-brief, debrief, or post-simulation communications | Meet with an interprofessional team to plan a simulation case together |
| Invite learners to share what team behaviors supported them | |||
| Use plus-delta to capture positive interpersonal dynamics | |||
| Engagement | The experience of being fully absorbed, focused, and energized in a task or role | Co-Design immersive, realistic scenarios | Include multiple stakeholders in scenario co-design |
| Ask “When did you feel most focused or in the zone?” | |||
| Use video review to highlight moments of high engagement | |||
| Vitality | A sense of aliveness that energizes individuals and enables resilience and recovery | Focus on how learners sustained their energy and adapted under stress | Convey gratitude for high energy level |
| Normalize discussions of stress responses and discuss adaptive coping | |||
| Format session to enable repeated attempts and opportunity for immediate improvement | |||
| Accomplishments | Recognition of progress, mastery, or success in achieving goals | Call attention to individual, team, and system-level improvements resulting from simulation | Ask “What are you most proud of accomplishing today?” |
| Document progress across sessions (e.g., faster time to defibrillation) | |||
| Celebrate system improvements (e.g., unsafe conditions identified with simulation) | |||
| Meaning | The sense of purpose and significance derived from one’s work and its connection to larger values, such as patient care, teamwork, or service | Connect simulation experiences to broader professional purpose and patient impact | Choose scenarios based on actual patient cases |
| Ask if anybody has experienced similar challenges caring for actual patients | |||
| Ask what people will do if they see the same case during their next patient care session | |||
| Positive Emotions | Feelings such as joy, gratitude, pride, or relief that broaden thinking, improve coping, and strengthen resilience | Actively elicit pride, joy, or gratitude | Have fun creating novel scenarios or formats (e.g., escape room) |
| Open or close debriefing with sharing gratitude | |||
| Highlight humor or human connection where appropriate |
| Stage | Description | Positive psychology integration opportunity |
| Needs Assessment and Scenario Planning | Selecting, designing, and preparing the scenario and teaching team | Select learning objectives and cases based on recent, relevant patient scenarios. Involve inter-professional teams to design and teach scenarios - considering relevance for a range of professional roles. Use the planning team as a way to develop relationships and model |
| Pre-session Communication | All communication (e.g. course notices, emails, announcements, directions, pre-session materials, etc) that participants receive prior to attending the event | “The cases for our session are based on recent patient cases with great outcomes. We will focus on things that have/are going well, so that our entire team can all learn from and integrate these strengths and best practices.” |
| Facilitator Preparation | Consider the current culture/ outcomes of needs assessment. Identify learning objectives, scripting, logistics (e.g. location, comfort, time, etc) and teaching team structure (e.g. professional roles of debriefers) | Edit current outgoing communication to reflect positive psych principles (see above) Edit current debriefing scripts to reflect positive psychology questions (see below) Look for opportunities in every step to incorporate positive psychology principles |
| Environment preparation | Everything the participants see, hear, or experience in the simulation space (e.g. welcoming signage, introductory videos, instructions or posted ground rules and assumptions) | Incorporate into non-verbal experience (e.g. Signage “Our events help us to identify our team’s strengths. This depends on the experience and perspective each person brings. Please introduce yourselves to one another and share your role in the team and a goal you have for today’s session”) |
| Pre-briefing | What is shared/done with the participants prior to the start of the simulation (e.g. clarification of goals, roles, expectations) | Include opportunities for engagement and relationship building. Prior to starting the session, invite participants to participate in a breathing exercise to promote individual calming and mindfulness. Share goals (e.g. “Our goal is to improve how we work together and the care we provide our patients, by identifying our strengths and opportunities for growth). |
| Simulation scenario | Scenario selection and design including branched phases, based on team actions | Include scenarios with relevance for the team, identify patient care scenarios with successful behaviors/outcomes |
| Debriefing | Debriefing structure and scripting | Incorporate positive psychology scripting (see Table |
| Post-session communication | All communication (e.g. learning summaries, issue summaries, mitigation plans) that participants receive after attending the event | “In our last simulation session, we identified two systems issues that are being addressed…We also highlighted individual and group strengths including...” |
| Debriefing phase | Sample positive psychology intervention | Definition | Examples |
| Setting the scene (create safe context for learning) | Positive introduction | A positive introduction is where somebody introduces a time when they acted virtuously as their “best possible self” | “Take a moment before we begin to think about a moment when you were proudest of yourself or someone else.” |
| Positive priming | Positive priming is the intentional activation of positive emotions before an activity | “As we start the debrief, I want you to think of a way you helped during the scenario and also somebody that really helped you.” | |
| Reactions (explore feelings) | Counteract the negativity bias | Intentional focus on positive emotions and reactions can help counterbalance the stickiness of negative emotions |
|
| Mindfulness | Mindfulness is intentional slowing down, increased awareness of the present, noticing with all senses, and without judgment | “As we start to explore our reactions to this case, let’s pause and notice what's going on in each of our bodies (your pulse, your breath, whether you feel calm or nervous. Try to simply notice, without judgment. Would anyone like to share what they are noticing?" | |
| Description (clarify facts) | Connect with meaning | Reflecting on the personal and shared purposes | “Can you summarize the case and share if you have ever had a similar case?” “What did you find most important/relevant about this case?” |
| Practice gratitude | Recognizing and appreciating others or systems/ circumstances that support our work and learning | “Can you summarize the case and share if you have ever had a similar case?" "What did you find most important/relevant about this case?” | |
| Analysis (explore performance domains) | Spot character strengths | Identifying and naming character strengths helps promote self-worth, resilience, and well-being. Spotting strengths in team members can build morale and enhance relationships. The values in action (VIA) classification lists 24 character traits that contribute to personality and categorizes strengths into six categories: wisdom, love of learning, courage, humanity, justice, temperance, and transcendence [ | Facilitators can spot character strengths in group members or invite participants to spot strengths in themselves or each other. Facilitators can share the list of 24-character strengths to provide the language to group members. “I noticed an action that took a lot of courage. [name of participant] I noticed you asked for help with [action]. [name] can you talk to us through your thoughts and actions?” “What did the team notice about the bedside RN during this case, what strengths did he bring to the case?” Groups can also reflect on what strengths they are using collectively in the debrief, e.g. perspective, curiosity, love of learning, bravery, etc. |
| Positive reframe | Shifting perspective from a negative interpretation of events to a neutral or positive one (e.g., reframing obstacles as challenges, mistakes as learning opportunities) Considering what values or character strengths are underlying a negative interpretation of events Discuss how negative events may be temporary and isolated, rather than permanent, personal, and pervasive | “You mentioned that moment was tough, what strengths stood out in how the team responded to that challenge?” | |
| Practice Self-Compassion | Treating oneself with kindness, recognizing struggle as universal, and creating healthy emotional distance from painful experiences without disavowing them |
| |
| Application/Summary (identify take-aways) | Celebrate wins (including growth) | Recognizing and appreciating effective moments, progress, or achievements to reinforce positive emotions and foster a sense of shared meaning |
|
| Positive intervention meta-cognition | Explicitly naming positive psychology principles to build awareness, foster a culture of well-being, and encourage a ripple effect for continued practice | “You’ve probably noticed that we intentionally paused today to focus on our unique strengths and share gratitude for each other – these small habits are based on positive psychology principles that help teams and individuals flourish. I hope we’ll carry some of these practices forward into our clinical environment to promote a culture of well-being.” |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSimulation-Based Education in Healthcare · Patient Safety and Medication Errors · Workplace Violence and Bullying
Introduction
Modern healthcare systems are often designed with an emphasis on diagnosing illness, evaluating error, reacting to system failures, and debriefing what has gone wrong. While this vigilance is essential for ensuring patient safety, it leaves less room for learning from what goes right. Tools like safety-II, positive event debriefing, and strength-based reflections can broaden our lens toward success, resilience, and system adaptability. Without this balance, the medical model’s deficit orientation, both in theory and in practice, risks eroding clinician morale and fueling burnout [1].
Contemporary researchers have proposed expanding the Institute for Healthcare Improvement's Triple Aim (better health, better care, and lower cost) into a Quadruple Aim by adding a fourth goal: improving the work-life and well-being for the healthcare workforce [2,3]. The Centers for Disease Control and Prevention (CDC) has similarly encouraged integrating professional well-being into all quality improvement initiatives, recognizing healthcare workers as central to the functioning of healthcare systems [4]. Despite increased awareness, particularly in the wake of COVID-19, clinician burnout, moral injury, and psychological distress remain endemic across the health care workforce [5,6]. When a negative mindset dominates healthcare culture, prioritizing error detection over celebrating resilience, clinicians are at risk of accelerated disengagement and loss of meaning in work.
Simulation is uniquely positioned to be a driver of change within organizations [7,8]. Simulation programs are often situated at the junction between the learning environment, quality and safety, interprofessional teamwork, and clinical implementation paradigms, and as such are uniquely positioned to shape behaviors and mindsets. Simulation-based education, particularly through structured debriefing, has long served as a powerful tool for fostering psychological safety, enhancing reflective capacity, and driving positive change in a low-stakes environment. Many of the principles of positive psychology are already embedded in the debriefing pedagogy and lexicon, whether through social learning theory, plus-delta, safety-II/resilience engineering, or growth mindset. These frameworks highlight connection, resilience, and learning from success, values that align closely with key principles of positive psychology.
This article was previously presented in part at a meeting workshop at the 2025 (Munich, Germany) and 2020 annual International Pediatric Simulation Symposia and Workshops meeting for the International Pediatric Simulation Society.
Technical report
Positive psychology, popularized by Martin Seligman [9] at the turn of the 21st century, offers a powerful counterbalance to health care’s prevailing negativity bias. As a subfield of psychology, it focuses on the empirical study of well-being and human flourishing, examining constructs that contribute to individual and collective thriving. Frameworks such as Seligman’s PERMA model (positive emotions, engagement, relationships, meaning, and accomplishment) and the updated REVAMP framework (which adds vitality and is specifically geared for clinical settings) summarize core ingredients of well-being that are especially relevant in healthcare [9,10] (see Figure 1). Many of these concepts already permeate simulation, for example, practicing as a team naturally strengthens relationships at work, yet there are opportunities to be more intentional in how we cultivate them.
Framework of factors contributing to positive well-being and flourishing (REVAMP)REVAMP stands for relationships, engagement, vitality, accomplishments, meaning, and positive emotions.
Beyond conceptual models, positive psychology researchers have designed and tested intentional activities aimed at cultivating well-being known as positive psychology interventions (PPIs) [11-16] (see Table 1). These interventions target one or more domains of well-being (e.g., meaning, positive emotions, relationships, etc.) and have been shown to enhance resilience, engagement, thriving, and mitigate burnout. Despite a growing body of evidence supporting their effectiveness, positive psychology principles and PPIs have not yet been systematically integrated into the healthcare culture.
The simulation’s impact can be amplified through the intentional and explicit application of positive psychology. This approach is not about suppressing negative emotions, glossing over errors, or avoiding difficult conversations, which risks “toxic positivity” and can undermine psychological safety and trust. Instead, the aim is to acknowledge challenges while framing them in ways that foster growth, resilience, and agency. A balanced approach intentionally draws attention to strengths, progress, and meaning alongside authentic reflection on opportunities for improvement. By incorporating positive psychology frameworks such as the REVAMP model and evidence-based PPIs into debriefing conversations, educators can reframe challenges constructively, reinforce adaptive behaviors, and strengthen social connections and meaning at work (see Table 2).
Within any healthcare team, there are opportunities to systematically embed positive psychology throughout all stages of the simulation process, from planning and scenario design to debrief and follow-up. Table 3 provides additional examples for the integration of positive psychology across all phases of simulation.
Thoughtful integration of specific phrases or PPIs during the debriefing phase can further enrich discussion and deepen the impact of positive psychology principles within the experience. While authenticity is paramount, having a few pre-scripted positive prompts or targeted questions, as illustrated in Table 4, can help facilitators apply these principles reliably, especially when they are first getting started. Briefly previewing that you are trying a new technique can also smooth the transition and maintain transparency while building fluency in new techniques.
Discussion
The following example illustrates a pragmatic approach to integrating positive psychology into practice.
Needs assessment and planning stage
You are preparing an interprofessional simulation for a clinical unit that has recently experienced rapid growth and turnover. Many team members are early in their careers and motivated by a strong purpose to provide excellent patient care, yet the busy clinical pace has limited opportunities for team reflection and connection during shifts. You want to integrate positive psychology principles but realize that not every intervention can (or should) be applied at once, so to prioritize, you conduct a brief needs assessment talking to a few frontline staff and clinical leaders. Hospital well-being surveys have identified issues of belonging and feelings of isolation and an annual safety attitude questionnaire revealed issues around trust and feeling safe to speak up. Your needs assessment reveals themes of negativity bias (focus on errors), moral distress (from recent bad outcomes amidst resource constraints), burnout (which has eroded vitality), and limited relationships. The fact that frontline staff requested more simulation underscores their strong desire to learn (engagement, meaning, positive emotions), and leadership wants simulation to help disseminate new workflow and space improvements (accomplishments).
To promote relationships and model collaboration from the outset, you convene a small inter-professional planning group (doctor, nurse, and respiratory therapist). Together, the group decides to prioritize meaning, an existing team strength, and relationships, to build trust and support across the team. They select a recent case with strong clinical relevance and emotional resonance, and design a scenario that offers shared problem-solving opportunities for all team members.
Pre-simulation stage
In pre-session communication, you share pride in the team’s inter-professional approach to planning the simulation experience. You acknowledge the time and effort that both planners and participants are investing and express gratitude for their engagement. In highlighting the purpose of the simulation, you emphasize the incorporation of key points from recent meaningful cases and highlight the recent accomplishments of newly rolled out resources in the room being used.
On the day of the session, you welcome people with theme music from a popular action movie to energize people and make them laugh as they come in, employing fun and playfulness to promote feelings of vitality and connection. At the entrance to the simulation room, there is a brief message of gratitude on the sign-in log and a QR code with a link for the positive quote of the day. Learners are asked to silence phones to support presence and mindfulness. Name badges are used to encourage introductions between participants.
During the pre-brief, learners introduce themselves and share one thing they are proud about from the prior week. Before beginning, you guide the team in a brief mindful moment where they close their eyes, breathe in together and then slowly breathe out while focusing on the intention to take risks together during the simulation to foster learning.
Simulation stage
The simulation scenario carefully blends elements from recent clinical cases that are strongly relevant for all members of the inter-professional team. Branch points in the case are designed to be triggered by specific aspects of teamwork and communication. It is intentionally written to provide adequate challenge and reinforce a sense of accomplishment with completion of challenging tasks while eliciting meaningful opportunities for reflection on improvement. The quality of chest compressions (depth, rate, and recoil) is recorded by a high-technology manikin to facilitate discussion about quality and launch of a new mock code chest compression leaderboard (something the team came up with as a motivator) that enhancing engagement by posting high scores in the break room every month.
Debriefing stage
After completing the scenario, your planning team helps the team transition to a learning stance by having them step away from the simulation space, take three deep breaths (mindfulness), close their eyes, and picture one thing they saw or heard another teammate do well during the case (positive experience recall and priming).
You start the debrief using the PEARLS (Promoting Excellence and Reflection in Learning) debriefing framework [18], actively incorporating positive psychology principles and interventions throughout the five phases of the debrief (setting the scene, reactions, description, analysis, and summary). Co-debriefers actively invite reactions from each professional group, acknowledging expertise and strengths across roles, and model mutual respect in the discussion. Throughout the debrief, you weave in principles of meaning and relationships, prompting reflections with inquiries such as: “What did you find most important or relevant about this case?" and "Can someone share a few things you're grateful for, big or small, about how the team worked together?" Pre-scripting some positive prompts or targeted questions based on examples in Table 4 helps ensure these principles are reinforced consistently.
Post-simulation stage
After the simulation, you complete the learning cycle by following up with an email to the participants and take home points for the rest of the unit. You once again convey gratitude to the team and leadership for their engagement and commitment to improving care and growing together as a team. The connection to real clinical cases and reinforcement of new work resources and processes underscore the relevance of the session and its direct link to process improvement. While preserving anonymity (and thereby psychological safety), small wins and accomplishments can be called out. With the team’s prior permission a shout-out is made for the winner of the new “SimCompression leaderboard," highlighting accomplishments and the shared purpose of commitment to excellence.
Conclusions
In a time when healthcare teams are facing systemic challenges to well-being, positive psychology offers a practical framework for simulation-based interventions that strengthen relationships, engagement, vitality, meaning, accomplishment, and positive emotions at work. By intentionally embedding practices such as gratitude, mindfulness, strengths recognition, and positive reframes into debriefing, simulationists can help foster individual and team well-being. Positive psychology approaches are not designed to silence or ignore negative experiences. It is important to avoid “toxic positivity” and integrate interventions along with authentic reflections on error, stress, and system challenges to maintain psychological safety. A blended approach to learning from errors while reinforcing a positive mindset helps promote an orientation towards continued growth and sense of purpose.
Looking ahead, simulation may serve not only as an optimal environment for rehearsing clinical performance, but also as a space for processing system failures, moral distress, and emotional burden. Deliberately integrating team simulation and clinical debriefing into organizational well-being strategies could provide fertile ground for innovation in applied positive psychology interventions. Ultimately, the goal is to translate individual well-being to system-level culture change and improved clinical outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Burnout Stress: concepts, cognition, emotion and behavior Maslach C Leiter MP 351357 Elsevier Academic Press 2016
- 2From triple to quadruple aim: care of the patient requires care of the provider Ann Fam Med Bodenheimer T Sinsky C 573576122014 https://doi.org/10.1370/afm.17132538482210.1370/afm.1713 PMC 4226781 · doi ↗ · pubmed ↗
- 3The triple aim: care, health, and cost Health Aff (Millwood) Berwick DM Nolan TW Whittington J 7597692720081847496910.1377/hlthaff.27.3.759 · doi ↗ · pubmed ↗
- 4Introducing the Impact Wellbeing™ guide: taking action to improve health care worker well-being Workplace Health Saf Novicki E Howard J Simmons S 3207320254034683210.1177/21650799241290541 PMC 12065978 · doi ↗ · pubmed ↗
- 5Burnout trends among US health care workers JAMA Netw Open Mohr DC Elnahal S Marks ML Derickson R Osatuke K 08202510.1001/jamanetworkopen.2025.5954 PMC 1201335540257797 · doi ↗ · pubmed ↗
- 6Changes in burnout and satisfaction with work-life integration in physicians and the general US working population between 2011 and 2023 Mayo Clin Proc Shanafelt TD West CP Sinsky C 1142115810020254020247510.1016/j.mayocp.2024.11.031 · doi ↗ · pubmed ↗
- 7Changing systems through effective teams: a role for simulation Acad Emerg Med Rosenman ED Fernandez R Wong AH 1281432520182872725810.1111/acem.13260 · doi ↗ · pubmed ↗
- 8A study to assess the influence of interprofessional point of care simulation training on safety culture in the operating theatre environment of a university teaching hospital J Interprof Care Hinde T Gale T Anderson I Roberts M Sice P 2512533020162685419510.3109/13561820.2015.1084277 · doi ↗ · pubmed ↗