Surgical Technique for Stroke Prevention During Ventricular Assist Device Removal
Hannah Copeland, Tanisha Rajah, David Blitzer, John Morton

TL;DR
A surgical technique is described to prevent strokes when removing a heart support device called Impella 5.5, showing promising results in three patients.
Contribution
The paper introduces a novel surgical technique combining Trendelenburg positioning, carotid occlusion, and thrombectomy to reduce stroke risk during Impella 5.5 removal.
Findings
Three patients underwent the technique with no postoperative strokes or neurological deficits.
The method was feasible and safe for high-risk surgical candidates.
Device removal occurred 13 to 43 days after implantation without complications.
Abstract
Mechanical circulatory support with the Impella 5.5 is increasingly used as a bridge to heart transplantation or durable left ventricular assist device in patients with chronic heart failure. However, thrombosis and stroke remain significant concerns upon Impella 5.5 device removal. To mitigate this risk, one technique involves placing the patient in the Trendelenburg position, temporary carotid occlusion, and Fogarty thrombectomy during device explantation. We retrospectively report outcomes from 3 patients (mean age 45; 2 male) with chronic end-stage heart failure who underwent this technique between September 2022 and June 2023. Impella implantation was via axillary access as a bridge to heart transplant (n = 2) or durable left ventricular assist device (n = 1), with device removal 13 to 43 days later. All patients remained neurologically intact postoperatively, with no strokes or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
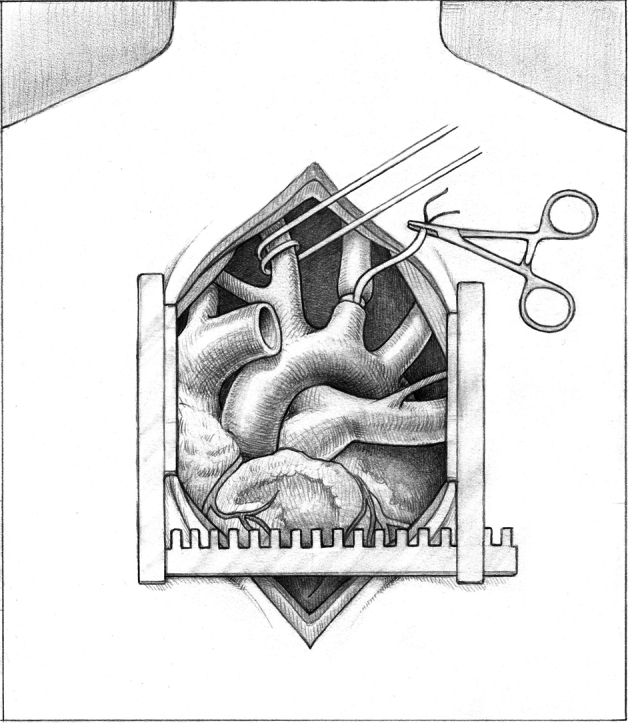 Figure 1
Figure 1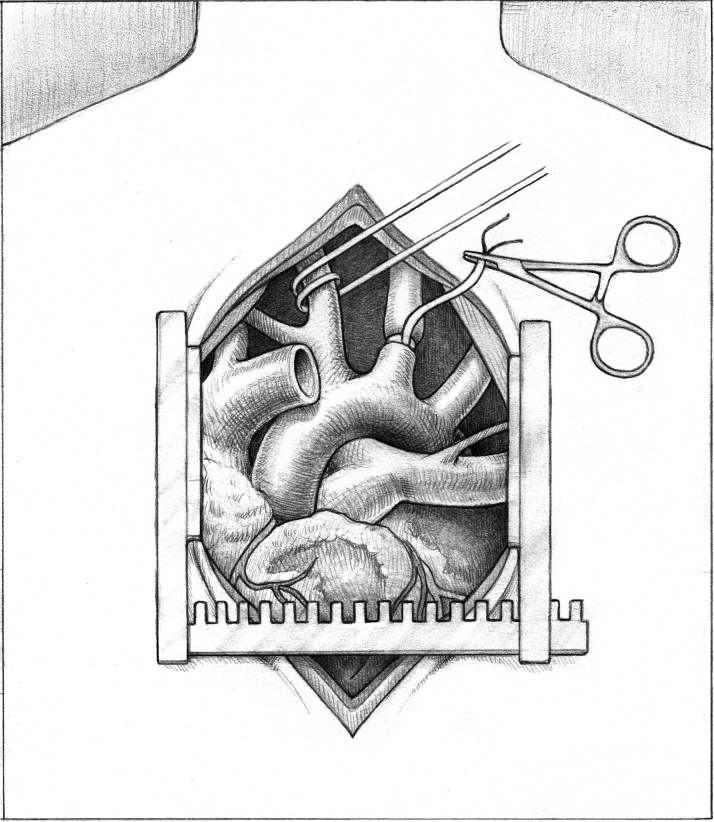 Figure 2
Figure 2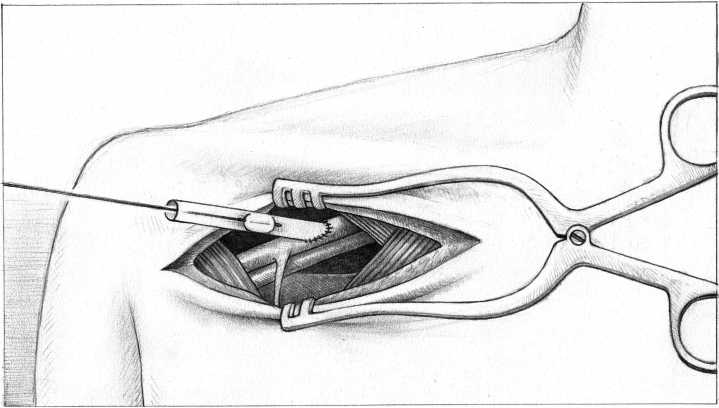 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac Structural Anomalies and Repair · Transplantation: Methods and Outcomes
Mechanical circulatory support has been increasingly used as a bridge to orthotopic heart transplant.1 Embolization and stroke are well-documented complications of left ventricular assist device (LVAD) removal,2 with the incidence of cerebrovascular accidents rates reaching 7.4% in specific patient populations.3 We describe a technique for preventing embolic stroke during Impella 5.5 (Abiomed) removal in heart transplant or durable LVAD implantation.Take-Home Messages
- •Bilateral carotid occlusion, followed by Fogarty thrombectomy is a simple, effective method to prevent stroke during Impella 5.5 removal.
- •No strokes occurred in all 3 patients using this technique.
Technique
The 8-mm graft for the axillary artery anastomosis is identified and prepared. A median sternotomy is performed, and hemostasis is achieved. The pericardium is opened and retracted. First the head vessels are palpated to ensure there are no palpable plaques. The right carotid artery past the innominate artery bifurcation and the left carotid artery are identified and encircled with umbilical tapes or vessels using a right angle (Figure 1). This is followed by intravenous heparin administration. Cannulation sutures are then placed in the ascending aorta and either the right atrium (for durable LVAD) or bicaval for heart transplantation. Once an appropriate activated clotting time is confirmed, the ascending aortic and the venous cannulae are placed, secured, and de-aired. The Impella 5.5 is gradually weaned and turned off, and cardiopulmonary bypass is initiated.Figure 1. Umbilical Tapes Placed Around the Bilateral Carotid Arteries
The patient is then placed in the Trendelenburg position. The right and left carotid arteries are snared, and either: 1) the Impella 5.5 is removed completely in the setting of durable LVAD implantation; or 2) the aortic cross-clamp is applied in the setting of heart transplant. The Impella is cut at the level of the aortic cross clamp, followed by the removal of the remaining Impella 5.5 in heart transplantation. The axillary graft is clamped after the removal of the Impella; the clamp is then removed off the axillary graft, and a Fogarty thrombectomy of the graft and axillary artery are performed with removal of clot and debris (Figure 2). To perform the thrombectomy, a Fogarty catheter is passed through the graft, the balloon is inflated and pulled back, and the clot is removed. The Fogarty catheter is passed into the axillary artery. Immediately afterwards, the snares are released and removed, leaving the right and left carotid arteries open. The axillary graft is cut and oversewn with a 4-0 prolene running suture, and the wound is then packed and closed at the end of the procedure.Figure 2. Demonstration of the Balloon Pull During Thrombectomy
Results
In this case series, we reviewed 3 patients who had Impella 5.5 removal between September 2022 and June 2023 using this novel technique. All 3 patients had chronic end-stage heart failure due to varying etiologies. Implantation of the Impella 5.5 was indicated either as a bridge to durable LVAD (n = 1) or a bridge to heart transplantation (n = 2). Impella insertion was via axillary access, with removal 13 to 43 days later.
Two out of 3 patients were male, with the average age being 45 years. In all 3 cases, no strokes occurred, with all patients being alert and orientated postoperatively. A summary of the case series is presented in Table 1.Table 1. Summary of Case Series Using Novel Technique for Stroke Prevention During Impella RemovalCasePatient DemographicsHeart Failure EtiologyIndication for ImpellaDuration of Impella ImplantationThromboendarterectomy Required?Postoperative Length of StayPostoperative Neurological Findings1FemaleAge 24 yearsKawasaki’s vasculitis, ischemic cardiomyopathyBridge to LVAD13 daysNo12 daysNo focal deficits2MaleAge 46 yearsDilated cardiomyopathyBridge to OHT27 daysYes19 daysNo focal deficits3MaleAge 66 yearsMixed (ischemic cardiomyopathy/non-ischemic cardiomyopathy)Bridge to OHT43 daysYes16 daysNo focal deficitsLVAD = left ventricular assist device; OHT = orthotopic heart transplant.
Discussion
Current strategies to prevent thromboembolic complications during Impella 5.5 removal vary across centers. While many experienced centers may adopt similar techniques, no standardized approach has been established, and the literature on this topic remains limited.
One approach is the use of embolic protection devices (EPDs); Ranganath et al4 reported successful use of these in a patient undergoing Impella removal without anticoagulation. However, some studies suggest that the use of EPDs has been associated with an increased risk of complications due to the required manipulation of the device within diseased aortic and carotid vessels.5 In addition, EPDs require radial or femoral artery access for their deployment, adding procedural complexity. Comparatively, our technique is a less-invasive form of embolic protection with minimal associated risks.
In contrast, our technique of temporary bilateral carotid artery occlusion achieves the same goal of embolic protection through a less-invasive approach. We use near-infrared spectroscopy monitoring throughout the snaring of the vessels, which takes typically about 1 to 2 minutes in total. This technique protects the brain and right arm vessels from debris that could migrate to these areas while the Impella is removed as it passes along the aortic arch. Thrombendarterectomy was performed on all patients when we bridged from Impella to durable LVAD and/or heart transplant.
Temporary bilateral carotid artery occlusion also avoids the need for additional arterial access and minimizes manipulation within the vasculature, thereby reducing the risk of access-related and embolic complications. While many experienced centers may already employ similar methods, we believe that formal description and standardization of this technique can support wider adoption and improve procedural safety.
Data Availability Statement
Data available upon request.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Iskaros O.Ahuja T.Arnouk S.Antithrombotic management for Impella® temporary ventricular assist devices: an analysis of an academic health-system experience Int J Artif Organs 45620225505593528533910.1177/03913988221082686 · doi ↗ · pubmed ↗
- 2Clothier J.S.Kobsa S.Praeger J.Impella 5.5 bridge to heart transplant: an institutional series and a closer look at device removal technique ASAIO J 701020248418473850214710.1097/MAT.0000000000002193 · doi ↗ · pubmed ↗
- 3Lazkani M.Murarka S.Kobayashi A.Seibolt L.Yang T.Pershad A.A retrospective analysis of Impella use in all-comers: 1-year outcomes J Interv Cardiol 30620175775832873690310.1111/joic.12409 · doi ↗ · pubmed ↗
- 4Ranganath N.K.Moazami N.Staniloae C.S.Hisamoto K.Successful embolic protection during temporary circulatory support device removal in a patient who required holding of anticoagulation for postoperative hemothorax J Thorac Cardiovasc Surg 15662018 e 203e 2043004192410.1016/j.jtcvs.2018.05.041 · doi ↗ · pubmed ↗
- 5Awad H.Hackett K.Ramadan M.E.Crestanello J.Con: routine use of embolic filters in transcatheter aortic valve replacement is not indicated J Cardiothorac Vasc Anesth 3222018105610612927729910.1053/j.jvca.2017.07.012 · doi ↗ · pubmed ↗