Revisiting Jenkins’ Rule: Evidence-Based Insights on the Suture-to-Wound Length Ratio and Wound Dehiscence
Jideofor Okoye, Ammar M Eskander, Kiranjot Kaur, Beshr Mosa Basha, Osasenaga Bencharles, Shashwat Shetty, Noman Ansari

TL;DR
This paper reviews evidence on how suture length to wound length ratios affect wound dehiscence, suggesting that the traditional Jenkins' 4:1 rule should be adapted based on surgical context and patient factors.
Contribution
The study provides evidence-based recommendations for tailoring suture-to-wound length ratios based on surgical tension, patient characteristics, and suture material.
Findings
Jenkins’ 4:1 suture-to-wound length ratio remains a reliable baseline for fascial closure.
Higher ratios (5:1-6:1) are beneficial in high-tension closures like emergency laparotomies in obese patients.
Lower ratios (3.5:1-4:1) suffice for low-tension procedures such as laparoscopic port-site closures.
Abstract
Wound dehiscence is a serious postoperative complication, with fascial closure technique and suture-length to wound-length (SL:WL) ratio being key determinants of wound integrity. Jenkins’ rule, recommending a 4:1 SL:WL ratio, has long guided midline laparotomy closure. Recent evidence suggests that optimal ratios should be tailored to the surgical context, patient factors, and suture material. High-tension closures, such as emergency laparotomies in obese patients, benefit from higher ratios of 5:1-6:1, while elective or low-tension procedures, including laparoscopic port-site closures, may achieve secure outcomes with ratios of 3.5:1-4:1. Modern suture materials, including monofilament, delayed-absorbable, and barbed sutures are combined with fine-bite or short-stitch techniques, enhance fascial approximation, reduce tissue trauma, and allow flexible ratio application. This systematic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
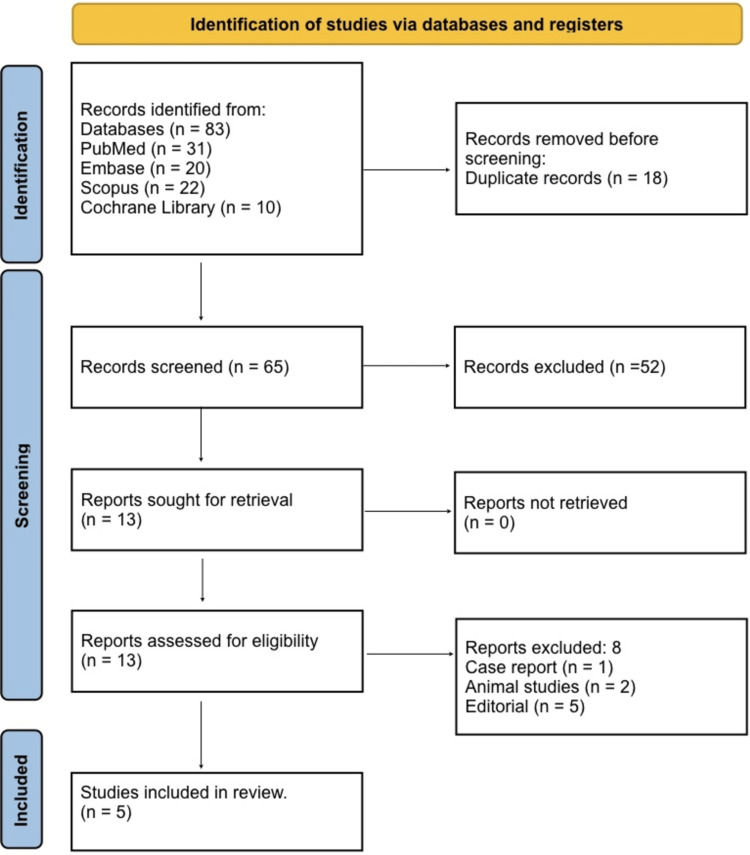 Figure 1
Figure 1| Authors and year | Population (P) | Exposure/Condition (I) | Comparator (C) | Outcomes (O) - wound dehiscence/incisional hernia | Pathophysiological findings | Anatomical impact | Dominant suture type | Closure technique | Typical SL:WL ratio | Dehiscence/hernia rate (%) | Key findings |
| Millbourn et al. (2009) [ | Adults undergoing midline incisions (n = 737) | Short‑stitch group (<10 mm bites) | Long‑stitch group (≥10 mm bites) | Wound dehiscence: 1/381; hernia: long 18% vs. short 5.6% | Short‑stitch and higher SL:WL may improve fascial strength | Midline laparotomy fascia | Not specified | Single-layer continuous running | At least 4:1 | Hernia: 18% vs. 5.6% | Supports >4:1 ratio and short-stitch to reduce hernia incidence |
| Williams et al. (2017) [ | 100 consecutive abdominal wall closures by residents | Measurement of SL:WL achieved | Not mentioned | SL:WL ≥4:1 achieved in 76%; higher infection/hernia when <4:1 | Lower SL:WL associated with worse wound outcomes | Abdominal wall fascial closure | Not specified | Continuous fascia closure | Mean ~4.6:1 | Not fully specified | Highlights that real-world compliance with the 4:1 rule is suboptimal |
| Deerenberg et al. (2015) [ | Elective midline laparotomy, n=560 | Small‑bite closure (5 mm from edge, 5 mm apart) | Large‑bite closure (10 mm/10 mm) | Incisional hernia: small 13% vs. large 21% at 1 year | Small‑bite plus higher SL:WL distributes tension better | Midline abdominal wall | Monofilament PDS | Continuous small‑bite vs. large‑bite | Small ~5:1; large ~4.3:1 | Hernia: 13% vs. 21% | Small-bite technique with higher SL:WL improves hernia outcomes |
| Seth et al. (2021) [ | Midline laparotomy closures pre- and post-education (n=200) | Education to achieve SL:WL ≥4:1 | Pre-education group | SL:WL ≥4:1 achieved 76% pre vs. 90% post | Education improves compliance with SL:WL and outcomes | Midline fascia | Not specified | Continuous closure | Target ≥4:1 | Not mentioned | Education improves the ratio of attainment and closure outcomes |
| Frassini et al. (2023) [ | Emergency midline laparotomy | Recommendation: SL:WL ≥4:1 | Standard closure (<4:1) | SL:WL ≥4:1 reduces incisional hernia/wound complications | A high ratio helps distribute tension in emergency closures | Midline abdominal wall | Not specified | Continuous midline closure | ≥4:1 | Not mentioned | Guideline-level support for ≥4:1 ratio in emergencies |
| Study | Study design | Tool | Risk rating | Justification |
| Millbourn et al. (2009) [ | Prospective cohort | ROBINS-I | Moderate | Large sample, but non-randomized and potential confounding; blinding not performed |
| Williams et al. (2017) [ | Prospective observational | ROBINS-I | Moderate | Small sample; performed by trainees, potential for operator bias; no randomization |
| Deerenberg et al. (2015) [ | Randomized controlled trial (RCT) (STITCH) | RoB 2 | Low | Multicenter RCT; randomization, blinding of outcome assessors, low attrition |
| Seth et al. (2021) [ | Prospective interventional | ROBINS-I | Moderate | Single-center educational intervention; non-randomized; potential selection bias |
| Frassini et al. (2023) [ | Guideline-based observational | ROBINS-I | Moderate | Observational in an emergency setting; heterogeneity in procedures; potential confounding |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Sutures and Adhesives · Surgical site infection prevention · Hernia repair and management
Introduction and background
Surgical wound dehiscence remains one of the most serious postoperative complications, contributing significantly to patient morbidity, prolonged hospitalization, and increased healthcare costs. Among the technical factors influencing dehiscence, the method of fascial closure and the ratio of suture length to wound length (SL:WL) have consistently been identified as critical determinants of wound integrity [1]. In 1976, Jenkins introduced a mathematical principle for midline laparotomy closure, demonstrating that when the suture length was at least four times the wound length, referred to as a 4:1 ratio, the risk of dehiscence was markedly reduced [2]. This concept, now widely known as Jenkins’ rule, has since become a cornerstone of safe and effective fascial closure techniques [3]. The principle is based on achieving even tension distribution across the wound and accommodating normal postoperative tissue expansion without compromising perfusion. Over the past few decades, several developments have challenged the universality of this rule. The introduction of modern suture materials such as monofilament delayed-absorbable sutures, barbed sutures, and fine continuous closure techniques has improved tensile strength, handling, and biocompatibility while reducing tissue trauma [4].
At the same time, surgical practice and patient demographics have evolved. Rising rates of obesity, emergency procedures, and minimally invasive surgeries have altered the biomechanical conditions of wound healing. These changes raise a crucial question: Does the traditional 4:1 ratio still represent the optimal balance between tension relief and tissue integrity in contemporary surgical practice? Recent research indicates that the 4:1 ratio remains a reliable baseline. However, higher ratios (5:1-6:1) may further reduce wound dehiscence in high-tension closures, such as in obese or re-operative abdominal wall patients [5]. Conversely, in low-tension settings, such as laparoscopic port-site closures, slightly lower ratios (around 3.5:1 to 4:1) may provide adequate strength without increasing the risk of wound failure. These findings suggest that Jenkins’ rule should not be regarded as a fixed standard but rather as a flexible guideline that can be adapted to the surgical context, suture material, and tissue tension. Consequently, there is a growing need to revisit and refine Jenkins’ rule in light of current surgical techniques and material advancements, aiming to establish an evidence-based, context-specific framework for optimal wound closure.
The primary aim of this study is to systematically evaluate contemporary evidence (2010-2024) on the relevance and validity of Jenkins’ rule, determining whether the 4:1 suture-length to wound-length (SL:WL) ratio remains optimal for minimizing wound dehiscence across different surgical settings. The secondary aim is to assess how factors such as suture material, closure technique, anatomical site, and patient characteristics influence the relationship between the SL:WL ratio and the risk of wound dehiscence, and to propose an updated, evidence-based perspective for modern surgical practice.
Review
Materials and methods
Search Strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines to ensure methodological transparency and reproducibility [6]. A comprehensive electronic search was performed across PubMed, Embase, Scopus, and the Cochrane Library to identify relevant studies published between January 2010 and December 2024. The search combined controlled vocabulary (MeSH/Emtree terms) and free-text keywords including “Jenkins’ rule,” “suture length to wound length ratio,” “fascial closure,” “abdominal wound dehiscence,” and “suture technique.” Boolean operators (“AND,” “OR”) were applied to refine results. Reference lists of included studies and key reviews were manually screened to identify additional eligible publications. Search results were imported into EndNote for organization and duplicate removal.
Eligibility Criteria
Eligibility was defined using the PICO framework to ensure methodological rigor [7]. The population included adult patients undergoing abdominal or fascial wound closure. The intervention involved closure following Jenkins’ rule or studies measuring the SL:WL ratio. Comparators included alternative closure techniques or materials not adhering to Jenkins’ rule. The primary outcome was wound dehiscence, with secondary outcomes including related closure complications. Eligible designs were randomized controlled trials (RCTs), cohort, and comparative studies, while animal studies, case reports, editorials, non-English articles, and abstracts were excluded.
Study Selection
All identified records were imported into a citation manager, and duplicate entries were automatically removed before screening. Two reviewers independently screened titles and abstracts to exclude irrelevant studies, following the PRISMA 2020 flow protocol. Full-text versions of potentially eligible articles were retrieved for in-depth evaluation against the inclusion criteria. Any disagreements regarding study inclusion were resolved by consensus or consultation with a third reviewer. The entire selection process, including the number of records at each stage, is presented in a PRISMA flow diagram to ensure methodological transparency and reproducibility.
Data Extraction
Data were extracted using a standardized template that included study characteristics, population demographics, type of surgical procedure, closure technique, suture material, SL:WL ratio, anatomical site, dehiscence rate, and follow-up duration. Data extraction was independently verified by two reviewers to minimize transcription errors and ensure data reliability. Due to heterogeneity in surgical procedures, patient populations, and SL:WL ratios, a meta-analysis was not performed. A narrative synthesis was conducted instead.
Risk-of-Bias Assessment
The methodological quality of RCTs was evaluated using the RoB 2 (Revised Cochrane Risk-of-Bias Tool) [8], while non-randomized studies were assessed with the ROBINS-I (Risk of Bias in Non-randomized Studies of Interventions) tool [9]. Each study was categorized as having low, moderate, or high risk of bias based on factors such as randomization, confounding, attrition, and reporting bias.
Data Synthesis
A qualitative narrative synthesis was performed due to heterogeneity in study designs, surgical populations, and outcome measures. Data were analyzed to identify consistent trends between SL:WL ratios and wound dehiscence rates across surgical contexts. When comparable data were available, pooled descriptive statistics were considered to highlight effect size directionality. Findings were integrated with methodological assessments to ensure balanced and statistically sound interpretation.
Results
Study Selection Process
A total of 83 records were identified through database searching, including 31 from PubMed, 20 from Embase, 22 from Scopus, and 10 from the Cochrane Library (Figure 1). After the removal of 18 duplicate records, 65 unique studies remained for title and abstract screening. Following this initial screening, 52 studies were excluded as they did not meet the inclusion criteria based on relevance or study design. The full texts of 13 articles were retrieved and assessed for eligibility. Of these, eight reports were excluded, comprising case reports, animal studies, editorials, and conference abstracts, leaving a total of five studies that met all inclusion criteria and were included in the final qualitative synthesis.
PRISMA 2020 flow diagram.PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of the Selected Studies
Table 1 summarizes key studies evaluating the SL:WL ratio and its impact on wound dehiscence. Millbourn et al. reported that short-stitch closures with SL:WL ≥4:1 in 737 midline laparotomies reduced hernia rates (5.6% vs. 18%) compared to long-stitch closures [10]. In 100 abdominal closures, Williams et al. observed that achieving SL:WL ≥4:1 lowered wound complications, while suboptimal ratios increased infection and hernia risk [11]. In the STITCH trial, Deerenberg et al. found that small-bite closures (~5:1 SL:WL) significantly reduced hernia incidence (13% vs. 21%) compared to large-bite closures (~4.3:1) [12]. A 2021 educational intervention [13] improved SL:WL compliance from 76% to 90%, highlighting the role of training. Frassini et al. recommended an SL:WL ratio of ≥4:1 for emergency midline laparotomies, demonstrating that higher ratios reduce wound complications in high-tension settings [14]. Across studies, the midline fascia was the primary anatomical site, continuous closure was commonly used, and monofilament sutures (polydioxanone (PDS)) were typical. SL:WL ratios of 4:1-5:1 were generally associated with optimal wound integrity and lower dehiscence rates.
Risk-of-Bias Assessment
The risk of bias across the selected studies varied according to design and methodology. Millbourn et al. conducted a prospective cohort study with a large sample, but the lack of randomization, potential confounding, and absence of blinding resulted in a moderate risk of bias [10]. Similarly, Williams et al. performed a prospective observational study with a small sample, operator variability, and no randomization, leading to a moderate risk [11]. In contrast, the STITCH trial by Deerenberg et al., a multicenter RCT with proper randomization, outcome assessor blinding, and low attrition, was rated as low risk [12]. Seth et al. implemented a single-center prospective educational intervention, which was non-randomized and subject to selection bias, resulting in moderate risk [13]. Finally, Frassini et al. reported a guideline-based observational study in an emergency setting with heterogeneous procedures and potential confounding, also rated moderate risk [14], as shown in Table 2.
Discussion
The findings of this systematic review reaffirm the central role of the SL:WL ratio in minimizing wound dehiscence, consistent with Jenkins’ original 4:1 recommendation. Millbourn et al.demonstrated that midline laparotomies closed with short-stitch techniques, achieving SL:WL ≥4:1, had lower hernia rates (5.6% vs. 18%), emphasizing the importance of adequate suture length for tension distribution [10]. Williams et al. similarly found that maintaining SL:WL ≥4:1 reduced wound complications and infections, while suboptimal ratios were associated with higher risk, highlighting real-world challenges in achieving the recommended ratio [11]. The STITCH trial by Deerenberg et al. further confirmed that small-bite closures with SL:WL ratios around 5:1 significantly reduced incisional hernia rates (13% vs. 21%) compared to large-bite closures, supporting the superiority of higher ratios and fine-bite techniques in elective midline laparotomies [12].
Educational interventions by Seth et al. demonstrated that targeted training improved compliance with the 4:1 rule from 76% to 90%, indicating that surgeon education is crucial in optimizing fascial closure outcomes [13]. Frassini et al. recommended SL:WL ≥4:1 in emergency midline laparotomies, showing that higher ratios effectively reduce wound complications in high-tension settings [14]. These studies collectively support a stratified approach to fascial closure: elective or moderate-tension closures can reliably follow the classic 4:1 ratio, optimized short-stitch techniques with SL:WL ~5:1 reduce dehiscence in elective procedures, and emergency or high-tension closures benefit from ratios ≥5:1. Modern suture materials, including monofilament and delayed-absorbable types, facilitate uniform tension distribution, allowing flexibility in SL:WL ratios while minimizing tissue trauma.
Several limitations must be acknowledged. The included studies were heterogeneous in terms of patient populations, surgical settings, closure techniques, and suture materials, limiting direct comparability. Some studies had small sample sizes or single-center designs, increasing the risk of bias and reducing external validity [10,11]. Additionally, follow-up durations were often short, potentially underestimating late dehiscence or hernia formation, and most studies focused on midline laparotomies, leaving other anatomical sites underrepresented. Future research should focus on large, multicenter trials stratified by patient body mass index (BMI), comorbidities, and surgical urgency to validate optimal SL:WL ratios across diverse populations. Biomechanical and imaging studies assessing fascial tension and perfusion could refine closure techniques, while investigations into novel suture materials, including barbed or hybrid absorbable sutures, may further improve outcomes. Development of procedure-specific, evidence-based SL:WL guidelines and long-term follow-up studies evaluating hernia formation, chronic pain, and wound integrity are needed to optimize modern fascial closure practices.
Conclusions
Jenkins’ 4:1 SL:WL ratio remains a reliable baseline, but modern evidence supports adjusting the ratio based on wound tension, patient factors, and suture type. High-tension closures may benefit from ratios of 5:1-6:1, while low-tension closures may use 3.5:1-4:1. Flexible application of Jenkins’ rule can optimize wound integrity and reduce the risk of dehiscence in modern surgical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suture length to wound length ratio in 175 small animal abdominal midline closures P Lo S One Winter V Degasperi B Bockstahler B DupréG 014201910.1371/journal.pone.0216943 PMC 652720531107892 · doi ↗ · pubmed ↗
- 2Editorial: Ten commandments of safe and optimum abdominal wall closure Indian J Surg Chintamani Chintamani 1051088020182991547310.1007/s 12262-018-1776-6PMC 5991013 · doi ↗ · pubmed ↗
- 3Abdominal wound closure--the Jenkins's technique: a registrar's experience Br J Surg Love A 27866197937831410.1002/bjs.1800660419 · doi ↗ · pubmed ↗
- 4Sutures and Needles Rose J Tuma F Treasure Island, FL Stat Pearls 2025 https://www.ncbi.nlm.nih.gov/books/NBK 539891/30969713 · pubmed ↗
- 5The 6:1 short stitch SL-WL-ratio: short term closure results of transverse and midline incisions in elective and emergency operations Hernia Golling M Breul V Zielska Z Baumann P 4474562820243828516810.1007/s 10029-023-02927-4PMC 10997695 · doi ↗ · pubmed ↗
- 6PRISMA 2020: an update J Pediatr Health Care Swartz MK 3513520213424384410.1016/j.pedhc.2021.04.011 · doi ↗ · pubmed ↗
- 7A review of the Pub Med PICO tool: using evidence-based practice in health education Health Promot Pract Brown D 4964982120203187456710.1177/1524839919893361 · doi ↗ · pubmed ↗
- 8Risk-of-bias assessment using Cochrane's revised tool for randomized trials (Ro B 2) was useful but challenging and resource-intensive: observations from a systematic review J Clin Epidemiol Crocker TF Lam N Jordão M 394516120233736462010.1016/j.jclinepi.2023.06.015 · doi ↗ · pubmed ↗