Molecular Characterization of Carbapenem and Colistin Resistance in Isolates Causing Urinary Tract Infections at an Outpatient Setting of a Tertiary Care Hospital
Chandan Mishra, Suneeta Meena, Purva Mathur

TL;DR
This study found carbapenem and colistin resistance in outpatient urinary tract infections, highlighting the need for early detection of antibiotic resistance genes.
Contribution
The study provides new data on carbapenem and colistin resistance in outpatient settings, where such data is scarce.
Findings
5.97% of isolates were carbapenem-resistant, with blaNDM being the most common gene detected.
Colistin resistance in carbapenem-resistant isolates was 11%, similar to previous studies at the same hospital.
Some isolates co-expressed multiple carbapenemase genes, indicating complex resistance patterns.
Abstract
Background Increasing resistance to higher-end antibiotics like carbapenems and colistin is a great cause of concern. There is a paucity of data on the detection of carbapenem and colistin in outpatient settings. This study was to determine the prevalence of carbapenem-resistant Enterobacterales (CRE) and colistin resistance in CRE at the outpatient setting of a tertiary care institute of North India. Methods A prospective study was conducted from January to December 2020. A total of 6,829 non-repetitive urine samples were cultured on cysteine lactose electrolyte-deficient (CLED) agar. Identification was done by matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS), and antimicrobial susceptibility testing followed Clinical and Laboratory Standards Institute (CLSI) 2020, using Kirby-Bauer and Vitek 2 (BioMérieux, Marcy-l'Étoile, France).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
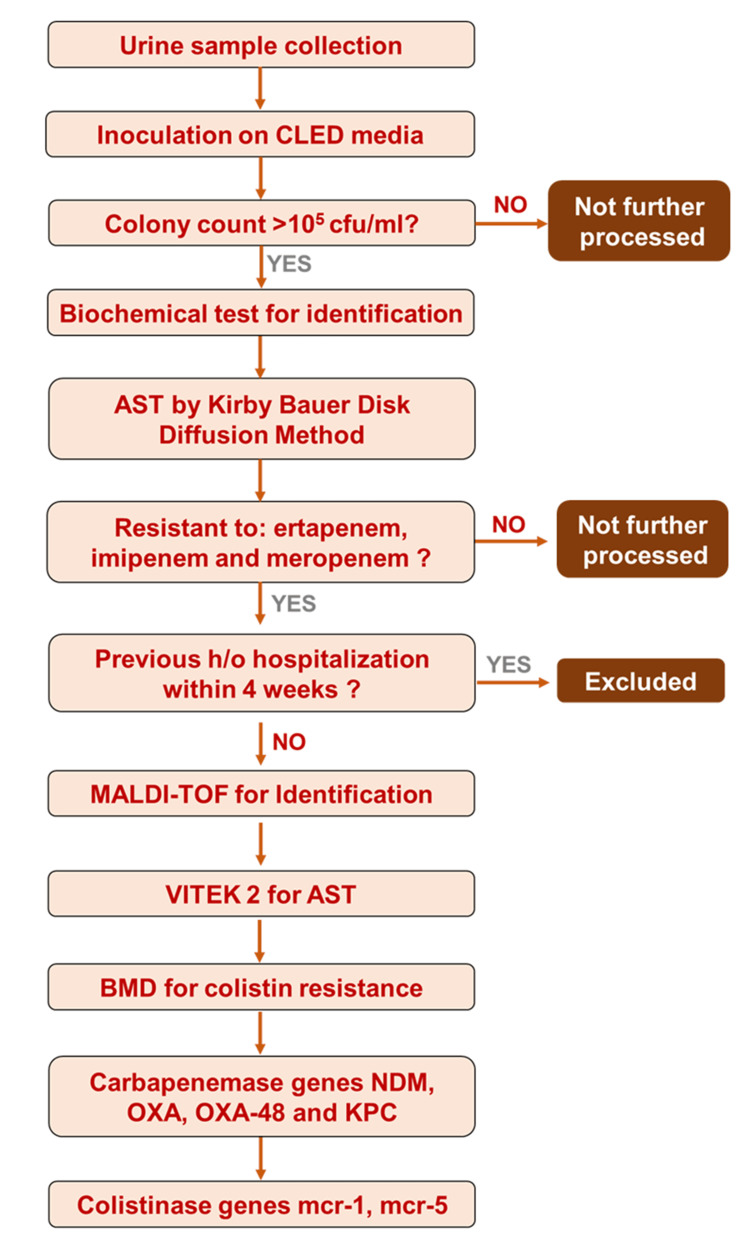 Figure 1
Figure 1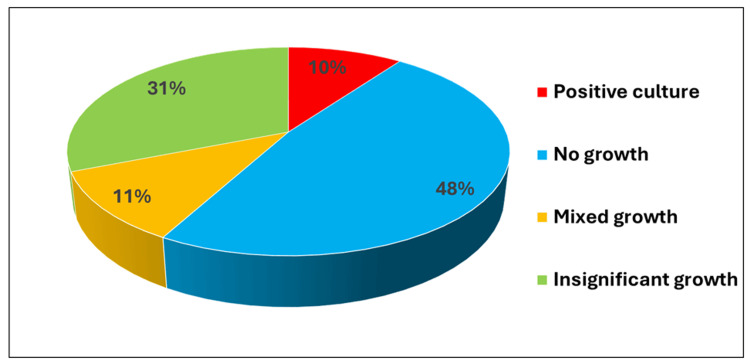 Figure 2
Figure 2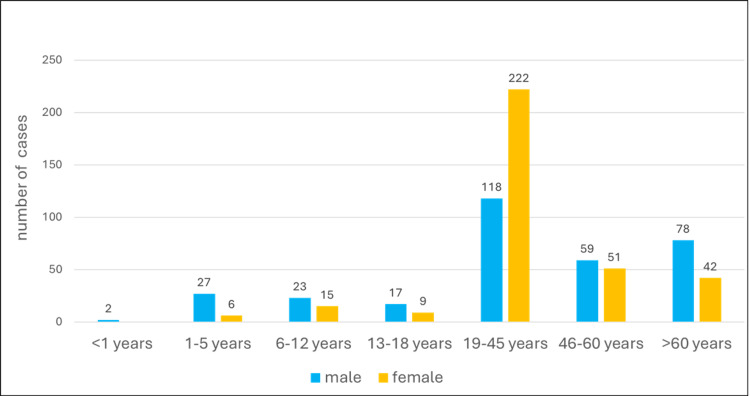 Figure 3
Figure 3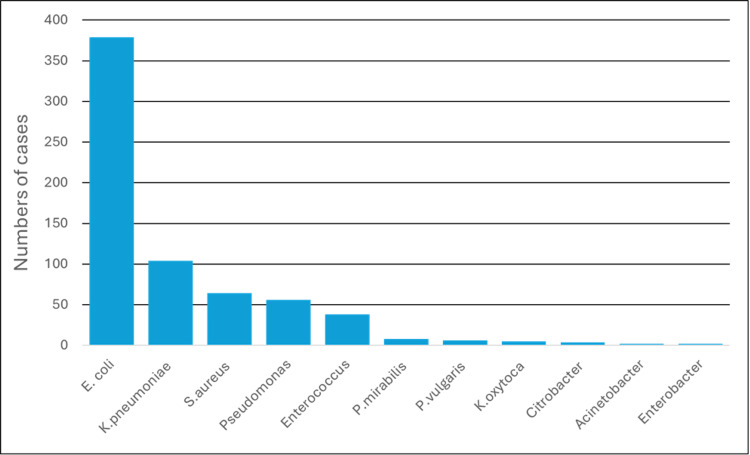 Figure 4
Figure 4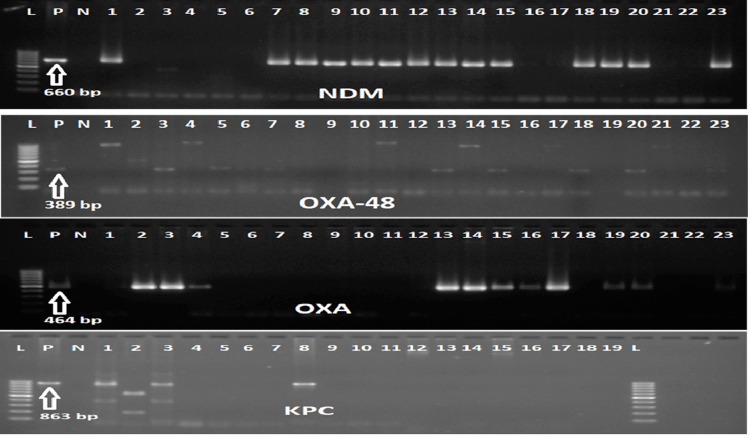 Figure 5
Figure 5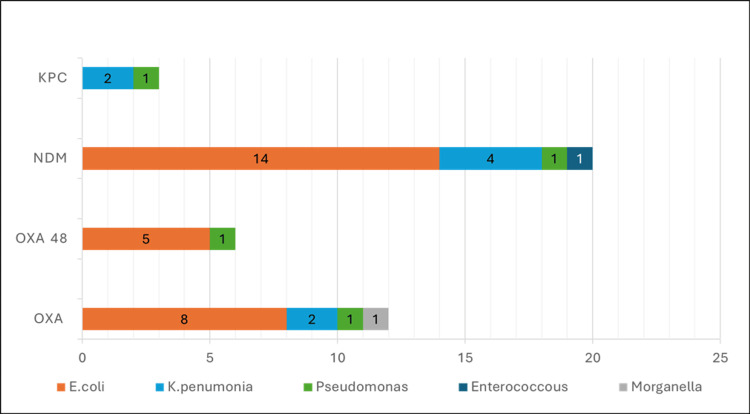 Figure 6
Figure 6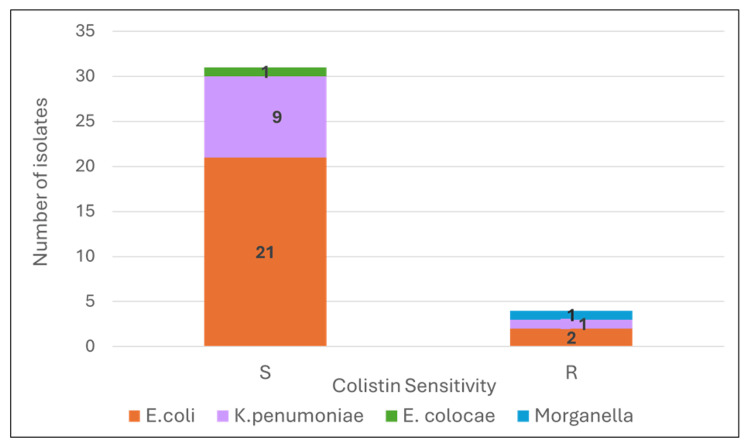 Figure 7
Figure 7| Characteristics | Overall (n=5091) | CRE (n=351) | CSE (n=4741) | p-value |
| Age | 37 (25, 54) | 32 (14, 46) | 38 (25, 55) | 0.22 |
| Gender | ||||
| F | 263 (52%) | 12 (34%) | 251 (53%) | 0.0093 |
| M | 246 (48%) | 23 (66%) | 223 (47%) | |
| Organism | ||||
| E.coli | 379 (74%) | 23 (65%) | 356 (75%) | 0.64 |
| K.pneumoniae | 104 (20%) | 10 (29%) | 93 (20%) | |
| P.mirabilis | 8 (1.6%) | - | 7 (1.5%) | |
| P. vulgaris | 6 (1.2%) | - | 6 (1.3%) | |
| K. oxytoca | 5 (1.0%) | - | 5 (1.1%) | |
| Citrobacter spp. | 4 (0.8%) | - | 4 (0.8%) | |
| Enterobacter spp. | 2 (0.4%) | 1 (3%) | 1(0.2%) | |
| Morgenella spp. | 1 (0.2%) | 1 (3%) | - | |
| Antibiotic | CRE n,(%) | CSE n,(%) | p-value |
| AK | 14 (78%) | 3 (38%) | 0.078 |
| AMC | 35(100%) | 395 (87%) | 0.0151* |
| AMP | 35 (100%) | 378 (83%) | 0.0072* |
| AS | 31 (89%) | 199 (45%) | <0.0012** |
| AT | 15 (100%) | 1 (25%) | 0.0041* |
| CAZ | 21 (100%) | 51 (59%) | <0.0012** |
| CIP | 35 (100%) | 342 (75%) | <0.0012** |
| COT | 31 (89%) | 249 (57%) | <0.0011** |
| CPM | 17 (94%) | 11 (69%) | 0.0781 |
| CX | 30 (88%) | 180 (41%) | <0.0011** |
| CZ | 28 (97%) | 153 (69%) | 0.0022* |
| FO | 11 (31%) | 47 (10%) | 0.0011* |
| GEN | 17 (94%) | 27 (26%) | <0.0012** |
| LE | 33 (94%) | 331 (74%) | 0.0161* |
| NIT | 20 (59%) | 97 (21%) | <0.0011** |
| NX | 6 (100%) | 27 (56%) | 0.0711 |
| PIT | 15 (88%) | 4 (44%) | 0.0281* |
| TCC | 18 (100%) | 4 (67%) | 0.0541 |
| TE | 28 (80%) | 208 (47%) | <0.0012** |
| TOB | 16 (100%) | 2 (40%) | 0.0081* |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Urinary Tract Infections Management · Bacterial Identification and Susceptibility Testing
Introduction
Antimicrobial resistance has challenged the treatment of common infections and is a threat to public health systems [1]. Carbapenems and colistin are the “last resort” antibiotics for treating infections caused by extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae [2].
Carbapenems, a beta-lactam group of antibiotics, kill bacteria by binding to the penicillin-binding proteins, inhibiting bacterial wall synthesis. Carbapenems are broad-spectrum antibiotics against gram-negative organisms and have a somewhat narrower spectrum against gram-positive organisms. Carbapenems are critically important drugs, so resistance to these is a serious healthcare concern [3].
Carbapenem-resistant Enterobacteriaceae (CRE) are defined by resistance to at least one carbapenem or the presence of a carbapenemase. CRE can be carbapenemase-producing (CP-CRE) or non-carbapenemase-producing CRE (non-CP-CRE) strains. CP-CRE produce carbapenemases enzymes to hydrolyse carbapenem, whereas non-CP-CRE have β-lactamase (ESBLs and AmpC enzymes) activity combined with structural mutations of membrane protein and efflux pumps [4].
After development of CRE there are few options left for treatment of multidrug-resistant (MDR) as well as extensively drug-resistant (XDR) gram-negative bacteria. Knowing risk factors associated with CRE acquisition in patients is important, as it has implications for empirical antibiotic therapy and also benefits in infection control. The emergence of CRE among populations is a serious threat to proper antibiotic therapy and eradication of infection. It requires the implementation of multilayered strategies and meticulous surveillance in healthcare and community settings. Carbapenems need to be prescribed and used cautiously [5].
Antimicrobial resistance to carbapenems that has become prevalent in inpatient settings is creeping into the community. In our laboratory we receive urine samples from outpatients for antimicrobial susceptibility. This study setting contains a mix of both inpatients who are followed up and patients from the community. Hence, this study reports the status of antimicrobial resistance in the outpatient setting in our hospital.
This article was previously presented as a meeting abstract at the 2025 ADLM Annual Scientific Meeting on July 29, 2025 [6].
Materials and methods
This is a prospective observational cohort study conducted in the Microbiology section of the Department of Laboratory Medicine, All India Institute of Medical Sciences (AIIMS), New Delhi. Ethical approval was obtained from the Institutional Ethics Committee prior to the start of the study (Ref. No.: IECPG-761/30,01.2020). During the period of study, freshly voided midstream urine samples (10-15 ml) collected in a sterile container with screw cap tops were accepted from different OPDs and processed in the lab within one to two hours for analysis. Urine samples were examined chemically and microscopically. Out of 567 gram-negative bacterial isolates, 43 that were resistant to carbapenem i.e., ertapenem, imipenem or meropenem were selected.
Organisms were identified using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS). A mass spectrum of each organism was generated and automatically compared against a database of mass spectra by MYLA® software, resulting in the identification of the organism. Quality control strain Escherichia coli ATCC-8739 was used to calibrate the instrument for each run.
Antimicrobial susceptibility testing used Vitek 2 (BioMérieux, Marcy-l'Étoile, France) and reported as per Clinical and Laboratory Standards Institute (CLSI) guidelines 2020. Antimicrobial susceptibility results were expressed in terms of measure of accuracy. Results of susceptibility tests were categorized as susceptible (S), intermediate (I), or resistant (R) according to criteria recommended by CLSI guidelines.
The bacterial isolates from the urine samples were subjected to DNA extraction by using HiPurA Genomic DNA Purification Kit (HiMedia Laboratories Pvt., Thane, India). The standard method as given in the kit insert was used for the bacterial DNA extraction. The extracted bacterial DNA was subjected to amplification of the specific region of different genes (NDM, KPC, OXA-1, OXA-48) using primers from Integrated DNA Technologies (Coralville, IA, USA) (Appendix).
Statistical analysis
Data was analysed using Stata statistical software, version 15 (StataCorp 2017, College Station, TX, USA), RStudio (Posit PBC, Boston, MA, USA) software version 2025.05.0+496 and Microsoft Excel 2019 (Redmond, WA, USA) were used for data analysis and graphical representation. Wilcoxon rank sum test, Pearson’s Chi-squared test, and Fisher’s exact test were used for calculation of statistical significance.
The flow of the study is given in Figure 1.
Flowchart of MethodologyCLED - cysteine lactose electrolyte deficient mediumcfu - colony forming unitAST - Antibiotic Sensitivity Testingh/o - history ofMALDI TOF - Matrix-Assisted Laser Desorption Ionization–Time of FlightBMD - Broth Micro Dilutionmcr-1 - mobilized colistin resistance -1mcr-5 - mobilized colistin resistance -5
Results
In this study a total of 6829 urine samples were collected between 1st January 2020 to 31st December 2020. Of 6829 samples, 669 were positive for the growth of pathogenic strains after removing duplicates (Figure 2). The majority (50.82%) of patients belonged to the early adult group (15-45 years) (Figure 3). Among the total pathogenic isolates, the Gram-negative isolates were most representative with 567 and were included in the study. Gram-negative isolates comprised 379 Escherichia coli (E. coli), 104 Klebsiella pneumoniae (K. pneumoniae), 56 Pseudomonas aeruginosa (P. aeruginosa), eight Proteus mirabilis (P. mirabilis), six Proteus vulgaris, five Klebsiella oxytoca (K. oxytoca), four *Citrobacter *spp., two *Acinetobacter *spp., two *Enterobacter *spp., and one *Morganella *sp. (Figure 4). Out of 567 Gram-negative bacterial isolates, 509 were enterobacterial, of which 35 were identified as CRE. The characteristics of these CRE and CSE are given in Table 1.
Urine specimen yields for culture growths.
Age group-wise population distribution.
Urinary isolates-wise distribution.
Carbapenemase in carbapenem-resistant Enterobacteriaceae
Polymerase chain reaction (PCR) was performed for detection of carbapenemase and colistin resistance genes. The presence of carbapenemase was determined by the identification of four genes: bla_NDM_, bla_KPC_, bla_OXA_, and bla_OXA-48_ (Figure 5). A total of 35 carbapenem-resistant enterobacterials were identified by disk diffusion method and verified by Vitek 2. The organisms identified were E. coli (n=21), Klebsiella pneumoniae (n=10), Pseudomonas aeruginoas (n=6), Acinetobacter baumanii (n=1), Morganella morganii (n=1) and Enterobacter cloacae (n=1). The most prevalent carbapenemase gene was NDM (18/35), followed by OXA (11/35), OXA-48 (5/35) and KPC (2/40). Some isolates had co-existence of two or more carbapenemase genes; four E. coli, one K. pneumoniae, and one Pseudomonas presented with OXA and OXA-48 genes, one E. coli with OXA and NDM genes, one K. pneumoniae with NDM and KPC genes, and two E. coli with OXA, OXA-48, and NDM genes. The* NDM* gene was present in 14 E. coli, four K. pneumoniae and one Enterobacter. The* OXA* gene was present in eight E. coli, two K. pneumoniae, and one Morganella morganii. OXA-48 was seen in five E. coli. KPC was in two K. pneumoniae (Figure 6). Those resistant to carbapenem were tested for colistin resistance by broth microdilution (BMD). Colistin resistance among CRE was 11% (Figure 7).
Gel electrophoresis for desired gene amplicon.The arrow indicates positive (P) control for the concerned gene. (L) is ladder. (N) is negative control.KPC - Klebsiella pneumoniae carbapenemaseNDM - New Delhi Metallo-β-lactamaseOXA-48 - Oxacillinase-48OXA - Oxacillinase
Gene representation of carbapenamase.KPC - Klebsiella pneumoniae carbapenemaseNDM - New Delhi Metallo-β-lactamaseOXA-48 - Oxacillinase-48OXA - Oxacillinase
BMD for colistin resistance in CRE.BMD - Broth Micro DilutionE. coli - Escheriachae coliK. pneumoniae - Klebsiella pneumoniaeE. cloacae - Enterobacter cloacaeS - Sensitive for colistinR - Resistant for colistin
We also compared the antibody resistance pattern in the CRE and CSE. This comparison revealed that all antibiotics showed significant results except fosfomycin, ticarcillin/clavulanate and tetracycline (Table 2).
Discussion
Antimicrobial resistance (AMR) is a worrisome epidemic that is slowly engulfing the whole world. Simple cases of uncomplicated UTI are also becoming difficult to manage due to AMR [7-9]. However, the burden of UTI and AMR may vary in different settings. UTI being the most common infection in the outpatients [10], and the second most common infection for an antimicrobial prescription (after respiratory infection) [11], this study was conducted to find the burden of carbapenem resistance in these patients.
Our study highlighted the prevalence of UTI and AMR in an outpatient setting, which has not been addressed in many other studies before. It was a prospective observational study, conducted over 12 months. A total of 6829 urine samples had 9.79% (669) pathogenic isolates. Sample positivity was also lower compared with the studies from North India [12]. The study was conducted during the COVID-19 pandemic when there was an upsurge of telemedicine (a remote provision of clinical care), where common ailments were treated by empirical therapy and also the outpatient service were running in limited capacity, which might also have affected the outcome of the study.
Microbial profile of uropathogens
In our study, the gram-negative organisms were 84.75%, gram-positive 15.25%. Escherichia coli (56.65%) was most prevalent among gram-negative organisms. This result was consistent with other studies from India [9,13,14]. The result was also consistent with studies from Africa [15], Europe [16], the Middle East [17], and Caribbean countries [18].
Other organisms included were* K. pneumoniae* (15.54%), S. aureus (9.56%), P. aeruginosa (8.37%), Proteus spp. (1.19%), and Enterobacter spp. (0.29%). Similar to our study other studies also showed *Klebsiella *spp. as the second most frequently isolated organism in UTI [19-23].
The studies on UTI done in other parts of the world also showed that E. coli and *Klebsiella *spp. are the commonest uropathogens in UTI [13,24-26]. Enterobacteriaceae have several virulent factors that enable them to cause UTI. They can easily attach to the uroepithelium of urogenital mucosa by adhesins, pili, fimbriae, and P-1 blood group phenotype receptors [27].
Carbapenemase in carbapenem-resistant Enterobacteriaceae
PCR was done for the detection of carbapenemase-producing genes such as blaKPC, blaoxa, blaNDM, and blaOXA-48. The most prevalent carbapenemase gene was NDM (20/40), followed by OXA (12/40), OXA-48 (6/40), and KPC (3/40). The* NDM* gene was present in 14 E. coli isolates, four K. pneumoniae isolates, one Pseudomonas and one Enterobacter. The OXA gene was present in eight E. coli isolates, two K. pneumoniae, one Morganella morganii, and one Pseudomonas aeruginosa. OXA-48 was seen in five E. coli and one Pseudomonas. KPC was found in two K. pneumoniae and one Pseudomonas [28].
Similar findings were seen in other studies from India, where the NDM gene was seen in most of the carbapenem-resistant isolates, followed by OXA-48 [29,30]. Whereas in some studies OXA-48 gene was most prevalent followed by NDM, wherein the authors have suggested that OXA-48 is becoming the most prevalent carbapenemase gene in K. pneumoniae [27].
In our study some isolates had co-existence of two or more carbapenemase genes. Four E. coli, one K. pneumoniae and one Pseudomonas presented with OXA and OXA-48 genes, one E. coli with OXA and NDM genes, one K. pneumoniae with NDM and KPC genes and two E. coli with OXA, OXA-48 and NDM genes. This similar co-existence of carbapenamase genes has also been reported in other studies [28-30]. Nine isolates did not show any of the carbapenemase out of four genes that were detected. which can be due to structural cause (porin loss) or hyperproduction of AmpC beta-lactamase or other carbapenemases [4].
Limitations
The sample size was small and the samples collected were during the COVID pandemic. A large-scale study is required in this region. All known causes of carbapenem resistance and colistin resistance were not included; thus, all potential resistance mechanisms were not included due to time and budget constraints. If modern sequencing-based molecular techniques could be used it would facilitate precise detection of all mechanisms of underlying carbapenem and colistin resistance.
Conclusions
Against the background of paucity of reports on prevalence of carbapenem and colistin resistance in uropathogens in an outpatient setting, this is the first study to determine the resistance in Enterobacteriaceae for last resort antibiotic i.e., carbapenems by molecular methods in the community. This study also fills the void in determining the epidemiology of uropathogens and antimicrobial resistance by conventional and automated methods in the outpatient setting. Our study showed that ampicillin, amoxicillin/clavulanic acid, ciprofloxacin, levofloxacin, cefoxitin, cefepime and cotrimoxazole had resistance >50%. Carbapenem-resistant gram-negative bacilli were 7.47%, which is a significant level in a community setting. Overall, we observed carbapenem-resistant isolates had carbapenemase-producing genes NDM, KPC, OXA and OXA-48. Some E. coli had the three carbapenemase genes (NDM, KPC and OXA).
Thus, we conclude community isolates are also showing multi-drug resistance to antibiotics and even against the last resort antibiotics. Carbapenem resistance that was prevalent in inpatient settings is now creeping into the community. Multiple studies with a larger sample should be conducted for carbapenem and colistin resistance in the region. It is recommended that empirical antimicrobial treatment should be based on the localized epidemiological trend. Our study reports status of antimicrobial resistance in the outpatient setting in our hospital, in order to establish guidelines for the correct use of antimicrobials. Therefore, action is needed from a broad range of stakeholders including clinicians, laboratory physicians and public health officers to limit the spread of antimicrobial resistance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Resistance of Gram-negative bacteria to current antibacterial agents and approaches to resolve it Molecules Breijyeh Z Jubeh B Karaman R 25202010.3390/molecules 25061340 PMC 714456432187986 · doi ↗ · pubmed ↗
- 2Carbapenem resistance: overview of the problem and future perspectives Ther Adv Infect Dis Meletis G 1521320162686239910.1177/2049936115621709 PMC 4735501 · doi ↗ · pubmed ↗
- 3Critically Important Antimicrobials for Human Medicine: 6th Revision Geneva World Health Organization 2019 https://www.who.int/publications/i/item/9789241515528
- 4The epidemiology of carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace J Infect Dis Logan LK Weinstein RA 036215201710.1093/infdis/jiw 282PMC 585334228375512 · doi ↗ · pubmed ↗
- 5Carbapenem and colistin resistance in Enterobacteriaceae: worldwide spread and future perspectives Rev Med Microbiol Ghasemian A Shafiei M Hasanvand F Shokouhi Mostafavi SK 173292018
- 6A-254 molecular characterization of carbapenem and colistin resistance in isolates causing UTI at an outpatient setting of a tertiary care hospital Clin Chem Mishra C Meena S Mathur P 712025 https://academic.oup.com/clinchem/article/71/Supplement_1/hvaf 086.243/8270226?login=false
- 7Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: a review J Chemother Mazzariol A Bazaj A Cornaglia G 292920172927173610.1080/1120009 X.2017.1380395 · doi ↗ · pubmed ↗
- 8Urinary tract infection: bacteriological profile and its antibiotic susceptibility in western India Natl J Med Res Shah LJ Vaghela GM Mahida H 452015 https://njmr.in/index.php/file/article/view/351