Fragile X and Fatal Rhythms: Electroconvulsive Therapy–Induced Ventricular Tachycardia
Muhammad Salman Sabri, Nimra Klair, Joshua Wiener, Maria T. Gamero, Drew Johnson

TL;DR
A man with Fragile X syndrome experienced dangerous heart rhythms during electroconvulsive therapy, highlighting the need for special precautions.
Contribution
This case highlights the risk of ECT-induced arrhythmias in FXS and suggests strategies like stellate ganglion block for prevention.
Findings
A patient with FXS developed ventricular tachycardia and cardiac arrest during ECT despite standard antiarrhythmic treatment.
Pretreatment with left stellate ganglion block and intravenous amiodarone was considered to mitigate arrhythmia risk.
FXS may increase arrhythmia susceptibility due to elevated sympathetic tone and ion channel abnormalities.
Abstract
Fragile X syndrome (FXS) is associated with autonomic dysfunction and ion channel abnormalities that increase the risk of arrhythmias. Electroconvulsive therapy (ECT), used to treat catatonia in FXS, can trigger a sympathetic surge, potentially inducing ventricular tachycardia. A 52-year-old man with FXS and catatonia developed recurrent wide complex tachycardia and cardiac arrest during ECT sessions, despite normal electrolytes, no structural heart disease, and a normal baseline electrocardiogram. The patient had recurrent cardiac arrest despite scheduled oral amiodarone 200 mg 3 times a day and premedication with 30 mg of esmolol. Pretreatment with a left stellate ganglion block and intravenous amiodarone infusion was considered before ECT sessions. FXS may increase susceptibility to arrhythmia owing to elevated sympathetic tone and channelopathies associated with fragile X mental…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
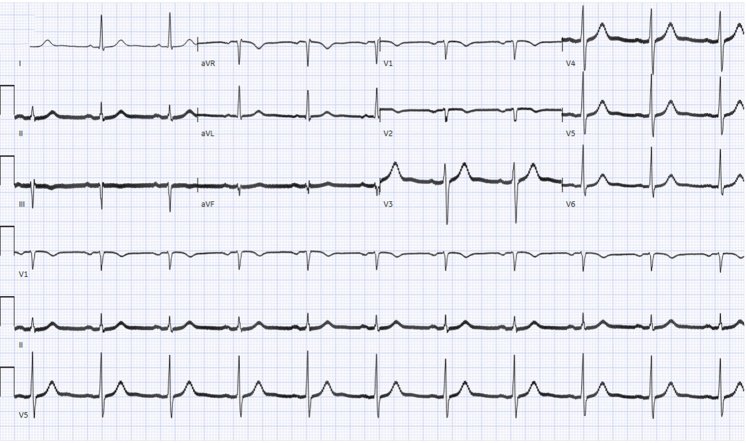 Figure 1
Figure 1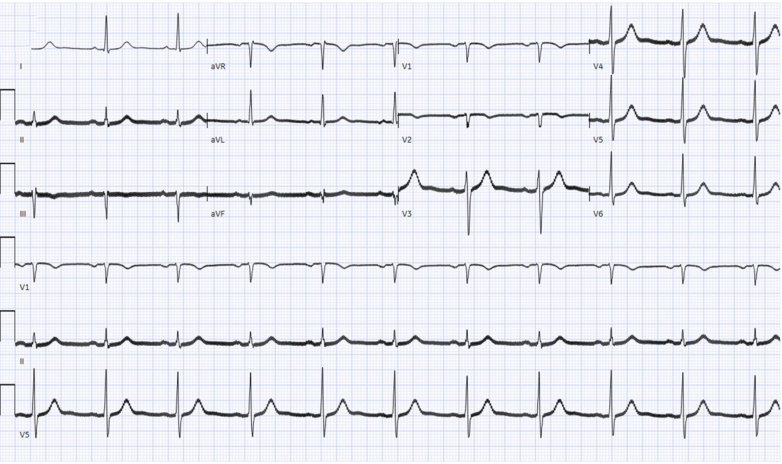 Figure 2
Figure 2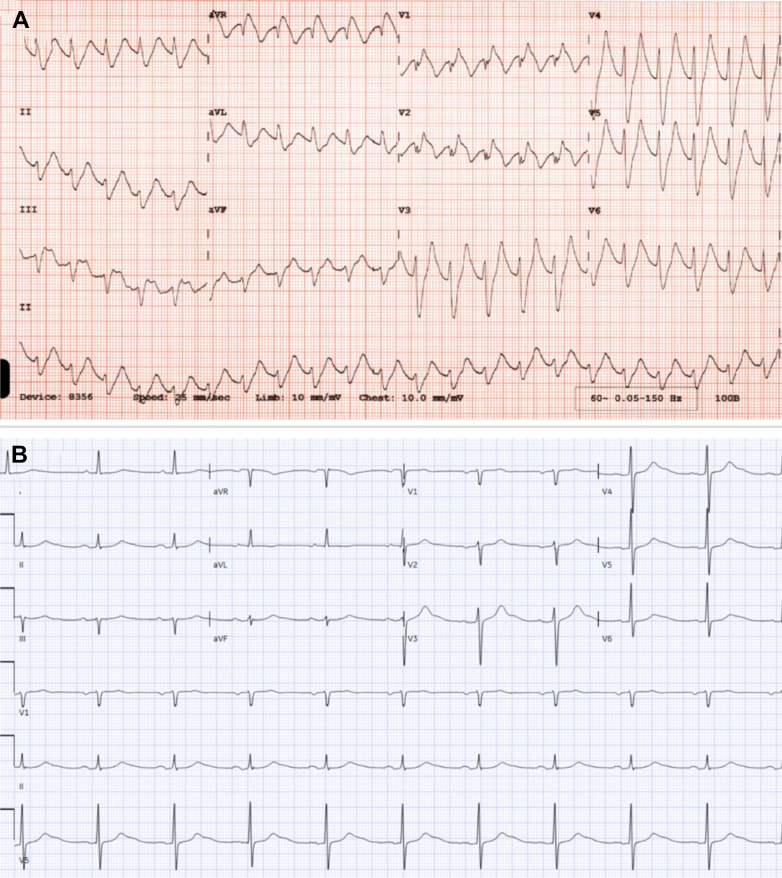 Figure 3
Figure 3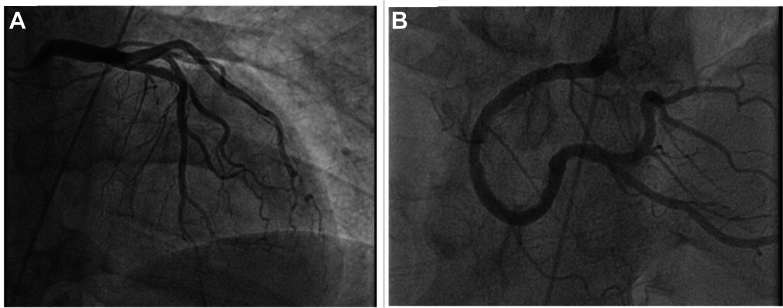 Figure 4
Figure 4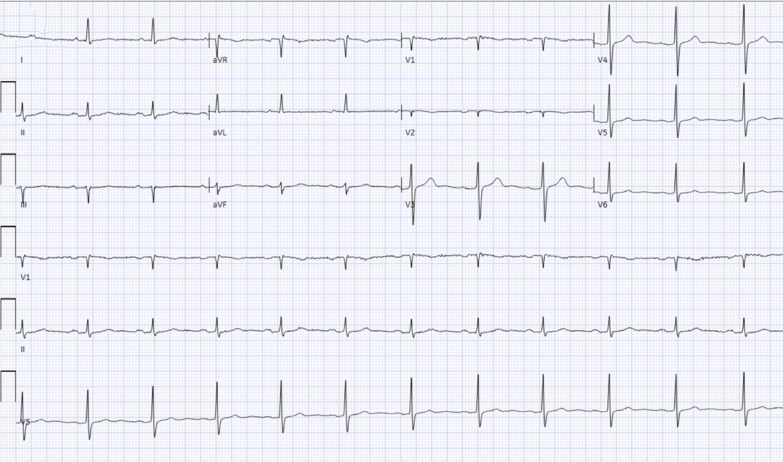 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenetics and Neurodevelopmental Disorders · Bipolar Disorder and Treatment · Cognitive Functions and Memory
Fragile X syndrome (FXS) is a genetic disorder characterized by a trinucleotide expansion that results in intellectual disability. It is associated with various cardiovascular issues, including hypertension, arrhythmias, and connective tissue disorders such as spontaneous coronary artery dissection and aortic dilatation. Patients with FXS can also develop catatonia due to underlying neurological and psychiatric conditions, which is often managed with electroconvulsive therapy (ECT). While ECT typically causes bradyarrhythmia, evidence suggests excessive sympathetic surge during the procedure can lead to ventricular tachycardia (VT). Reports of VT in patients with FXS are rare. We present a case of VT and cardiac arrest in a patient with FXS after ECT, and the therapeutic dilemma in management of VT.
History of Presenting Illness
A 52-year-old man was admitted for evaluation and management of encephalopathy and catatonia. Because of ongoing catatonia that did not respond to increasing doses of benzodiazepines, ECT was initiated. Before the initiation of ECT, his baseline electrocardiogram (Figure 1) revealed normal sinus rhythm with a QTc interval of 421 ms. Laboratory findings showed normal electrolyte and hemoglobin levels. He was not taking any medications known to prolong the QT interval. During the third ECT session, the patient experienced a pulseless cardiac arrest associated with wide complex tachycardia (Figure 2A), likely VT, necessitating defibrillation and cardiopulmonary resuscitation. Return of spontaneous circulation was achieved within 4 minutes. The patient was intubated during the event.Figure 1. Baseline Electrocardiogram Demonstrating Normal Sinus RhythmThe calculated QT was 421 ms.Figure 2. Electrocardiogram Showing Wide-Complex TachycardiaElectrocardiograms demonstrating (A) a wide complex tachycardia and (B) after cardiac arrest with normal sinus rhythm and a calculated QT interval of 440 ms.
On physical examination after the arrest, the patient remained intubated and sedated. Cardiovascular examination revealed a regular heart rate and rhythm without murmurs, gallops, or rubs. Lungs were clear to auscultation, the abdomen was soft, and the skin was warm and dry.
Past Medical History
The patient's history was notable for FXS, hypertension, type 2 diabetes mellitus (not requiring long-term insulin therapy), coronary artery calcifications, and a seizure disorder.
Investigations
The electrocardiogram after cardiac arrest (Figure 2B) demonstrated normal sinus rhythm with normal QTc and poor R-wave progression. A transthoracic echocardiogram (subcostal view) (Video 1) showed preserved left ventricular ejection fraction (65%) with small pericardial effusion. Coronary angiography (Figure 3) demonstrated nonobstructive coronary artery disease, including minimal luminal irregularities in the left main and left circumflex arteries, 30% stenosis in the proximal left anterior descending artery, and diffuse mild atherosclerosis in the right coronary artery.Figure 3. Cardiac CatheterizationCardiac catheterization using the right anterior oblique caudal view showing (A) a patent left anterior descending artery and left circumflex artery as well as (B) a patent right coronary artery.
Despite these cardiac events, and after a family discussion owing to the severity of his catatonia, another ECT session was carried out. During that session, the patient experienced a brief episode of VT that resolved spontaneously.
Management
Given concerns about a proarrhythmic state potentially linked to FXS and the arrhythmogenic nature of ECT, the patient was started on intravenous amiodarone with bolus of 150 mg, later transitioned to oral amiodarone at 200 mg daily. He was also receiving esmolol 30 mg before the ECT sessions. Additionally, aspirin and statin therapy were initiated for management of nonobstructive coronary artery disease.
Despite these measures, the patient suffered a third episode of sustained VT arrest during an ECT session while on amiodarone. Return of spontaneous circulation was achieved after 30 minutes. Electrocardiogram (Figure 4) performed earlier that morning showed normal sinus rhythm with a QTc of 410 ms. The electrophysiology team recommended considering intravenous amiodarone infusion (0.5 mg/min for 24 hours) and performing a stellate ganglion block before further ECT treatments. After this, the patient successfully completed 25 ECT sessions without further major cardiac complications.Figure 4. Electrocardiograms Demonstrating Normal Sinus Rhythm and Corrected QT of 410 ms
Discussion
FXS is characterized by a deficiency of the fragile X mental retardation protein (FMRP), which plays a critical role in cellular function, including the regulation of ion channels. The absence or reduction of FMRP has been implicated in connective tissue abnormalities, such as valvular heart disease, particularly mitral valve prolapse, as well as vascular fragility that may predispose to arterial dissections.1 Additionally, cardiac arrhythmias, including atrial fibrillation and premature ventricular complexes, have been reported in this population.1
Recent evidence suggests that individuals with FXS demonstrate elevated baseline heart rates, likely reflecting an imbalance in autonomic tone, as well as increased sympathetic activity and reduced parasympathetic input.2 FMRP is also involved in the regulation of multiple ion channels, including sodium, potassium, and calcium channels. Its deficiency may lead to channelopathies, which not only contribute to the neurocognitive phenotype of FXS but may also increase the risk of arrhythmogenesis, including ventricular tachycardia.
ECT is a recognized intervention for severe, treatment-resistant psychiatric conditions and is designed to induce a controlled generalized cerebral seizure.3^,^4 The autonomic response to ECT involves an initial parasympathetic surge, often resulting in transient bradyarrhythmias, followed by a sympathetic surge during seizure induction, which may lead to tachyarrhythmias.3 Although ECT-induced VT has been previously reported (Table 1), these cases invariably involve additional risk factors such as electrolyte abnormalities, structural cardiac disease, or use of agents such as atropine that are known to predispose to arrhythmias.3 To date, no documented cases have described ECT-induced VT occurring in the absence of these contributing factors.Table 1. Summary of Case Reports on ECT-Related Ventricular TachycardiaFirst AuthorComorbiditiesArrhythmiaProposed MechanismPostulated PreventionLarsen et al6AF and CHFNSVT for 17 s after ECTSympathetic surge and atropine useAvoid atropineUrabe et al7SchizophreniaVT for 30 s after ECT in setting of suxamethonium anesthesiaSuxamethonium-induced hyperkalemiaUse of thiamylal 250 mg and vecuronium 8 mg instead of suxamethonium along with magnesium prophylaxis prevented future episodesKim et al8UnknownNSVT of unknown durationCatecholamine-inducedResolved with IV landiolol; no recurrenceBailey et al9CatatoniaVT for 9 minHyperkalemia from succinylcholineAvoiding succinylcholine before ECTUsui et al10DepressionVT for unknown durationAdrenaline surgeProphylaxis with esmololKoga et al11Drug-resistant depressionVT for 10 sAdrenaline surge causing tachycardia and hypertensionNo future ECT sessionsPal et al12PsychosisVT for 2 minHypokalemia and adrenaline surgeManaging hypokalemia and hypomagnesemiaGrover and Aggarwal13SchizophreniaRecurrent VTAtropine and adrenaline surgeAvoid atropine before ECTSu et al5HFrEF, AF, TAVRNSVT that converted to AFAdrenaline surgeTreatment with esmolol/amiodaroneSabri et al (our case)FXS, HTN, DM2, CAD, seizure disorderMultiple NSVTs and sustained pulseless VTs of variable durationFMRP-related channelopathy and sympathetic surgeAddition of standing oral amiodarone, premedication with esmolol and consideration of IV amiodarone infusion 24 h before ECT and stellate ganglion blockAF = atrial fibrillation; CAD = coronary artery disease; CHF = congestive heart failure; ECT = electroconvulsive therapy; FMRP = fragile X mental retardation protein; HFrEF = heart failure with reduced ejection fraction; HTN = hypertension; DM2 = type 2 diabetes mellitus; IV = intravenous; NSVT = nonsustained ventricular tachycardia; TAVR: transcatheter aortic valve replacement; VT = ventricular tachycardia.
In the present case, our patient with FXS developed VT in the setting of ECT despite having normal electrolyte levels before and after arrhythmia, no structural heart disease on echocardiogram or catheterization, a normal baseline QTc, and no exposure to proarrhythmic medications such as atropine. We postulate that the underlying autonomic dysregulation in FXS marked by elevated baseline sympathetic tone and potential FMRP-related channelopathy synergistically increased the susceptibility to ECT-induced VT in our patient. The additional sympathetic surge induced by the seizure likely exceeded this patient's arrhythmic threshold, resulting in life-threatening VT.
Despite the occurrence of cardiac arrest, ECT sessions continued given the presence of profound catatonia, severe functional impairment, and alignment with family wishes. Initial management with standard antiarrhythmic therapy and beta-blocker prophylaxis was insufficient to prevent recurrence. However, a strategy involving pretreatment with intravenous amiodarone 24 hours before ECT and stellate ganglion block was successful in preventing further episodes of ECT-induced VT.
Although there is limited literature on the use of ECT in patients with FXS,5 this case highlights the potential risk of fatal arrhythmias in this unique population. The findings underscore the importance of recognizing FXS as a condition that may inherently predispose individuals to arrhythmias due to elevated sympathetic tone and possible ion channel dysfunction. Future research is warranted to better understand the arrhythmogenic risk in FXS, to guide the development of prophylactic strategies for VT in the setting of ECT, and to explore sympathetic modulation techniques such as stellate ganglion blockade as potentially more effective interventions than antiarrhythmics alone, particularly in cases not associated with scar-mediated VT.
Conclusions
This case highlights FXS as a potentially underrecognized risk factor for VT, particularly in the context of ECT. The interplay of autonomic dysregulation increased sympathetic tone, and potential FMRP-related ion channel abnormalities may elevate arrhythmogenic risk in this population. Given this vulnerability, thorough pre-ECT cardiac evaluation including baseline electrocardiogram and assessment for structural or conduction abnormalities should be considered. Continuous telemetry monitoring during and after ECT sessions is essential for early detection and management of arrhythmias. This case also underscores the urgent need for further research to better understand the electrophysiological phenotype of FXS and to develop evidence-based guidelines for arrhythmia prevention and monitoring in this high-risk group undergoing ECT.Take-Home Messages
- •FXS may predispose patients to VT owing to underlying autonomic dysfunction and ion channel abnormalities (channelopathies), even in the absence of structural heart disease.
- •ECT-induced sympathetic surge can trigger VT in vulnerable populations such as patients with FXS, warranting careful preprocedural risk assessment.
- •Sympathetic modulation strategies, including stellate ganglion block, may be essential adjuncts to antiarrhythmic therapy in preventing ECT-induced VT in high-risk cases.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tassanakijpanich N.Cohen J.Cohen R.Srivatsa U.N.Hagerman R.J.Cardiovascular problems in the fragile X premutation Front Genet 11202058691010.3389/fgene.2020.586910 PMC 757838233133171 · doi ↗ · pubmed ↗
- 2Heilman K.J.Harden E.R.Zageris D.M.Berry-Kravis E.Porges S.W.Autonomic regulation in fragile X syndrome Dev Psychobiol 538201178579510.1002/dev.2055121547900 PMC 3206129 · doi ↗ · pubmed ↗
- 3Deng P.Y.Klyachko V.A.Channelopathies in fragile X syndrome Nat Rev Neurosci 225202127528910.1038/s 41583-021-00445-933828309 PMC 8863066 · doi ↗ · pubmed ↗
- 4Baroud E.Bond J.B.Luccarelli J.Olusunmade M.Henry M.E.Abrams A.N.Safe administration of electroconvulsive therapy in a patient with catatonia and neuropsychiatric lupus comorbid with fragile X syndrome J ECT 384202225826010.1097/YCT.000000000000086235536988 PMC 9636063 · doi ↗ · pubmed ↗
- 5Su S.Shah P.Jassal D.S.Ventricular tachycardia triggered by electroconvulsive therapy: case report and review of the literature Clin Case Rep 1162023 e 745010.1002/ccr 3.7450 PMC 1022720037260618 · doi ↗ · pubmed ↗
- 6Larsen J.R.Hein L.Strömgren L.S.Ventricular tachycardia with ECTJ ECT 14219981091149641807 · pubmed ↗
- 7Urabe K.Koguchi T.Ishikawa K.[A case of ventricular tachycardia immediately after electroconvulsive therapy in a schinzophrenic patient] Article in Japanese Masui 5012001505211211751 · pubmed ↗
- 8Kim C.Sakamoto A.Ogawa R.Effect of landiolol on nonsustained ventricular tachycardia during electroconvulsive therapy Anesth Analg 10142005124710.1213/01.ANE.0000173762.12938.3716192565 · doi ↗ · pubmed ↗