Acute Rejection With DSA‐Negative Severe Microvascular Inflammation in a Kidney Transplant Recipient With an Isolated DPB1*04‐Mismatch Successfully Stabilised With Daratumumab
Laura Knödl, Maike Büttner‐Herold, Markus Götz, Markus Luber, Bernd Spriewald, Michael Oellerich, Julia Beck, Bernhard Banas, Daniel Zecher

TL;DR
A kidney transplant patient with severe inflammation but no detectable antibodies was successfully treated with daratumumab, suggesting new mechanisms of rejection.
Contribution
Demonstrates successful treatment of DSA-negative microvascular inflammation with daratumumab in a kidney transplant case.
Findings
Severe microvascular inflammation was reversed with daratumumab in a DSA-negative kidney transplant recipient.
The patient had an HLA-DPB1*04 mismatch but no detectable donor-specific anti-HLA antibodies.
The case suggests NK cell alloreactivity as an alternative mechanism of rejection in the absence of B cell alloreactivity.
Abstract
Microvascular inflammation (MVI) in kidney allografts in the absence of detectable donor‐specific anti‐HLA antibodies (DSA) is increasingly recognised as a cause of premature graft failure following kidney transplantation. Potential mechanisms include NK cell alloreactivity mediated by recognition of mismatched HLA class I molecules (missing‐self) via killer‐immunoglobulin‐like receptors. Here, we report the case of an early kidney allograft rejection with severe MVI on biopsy in a patient that was fully HLA‐matched except for a HLA‐DPB1*04 mismatch in the donor. There were no detectable DSA at any time. MVI was successfully reversed and clinically stabilised with a 9‐month course of daratumumab (anti‐CD38 mAb). This case suggests alternative mechanisms of alloreactivity, such as NK cell‐mediated effects, and highlights the existence of MVI in the absence of detectable B cell…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
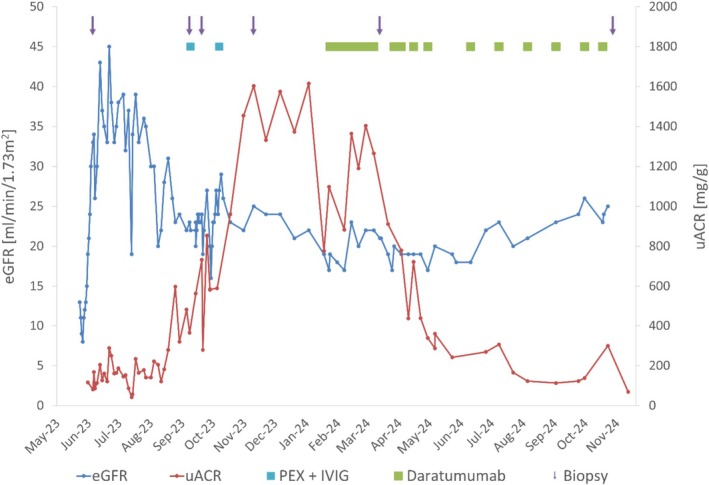 FIGURE 1
FIGURE 1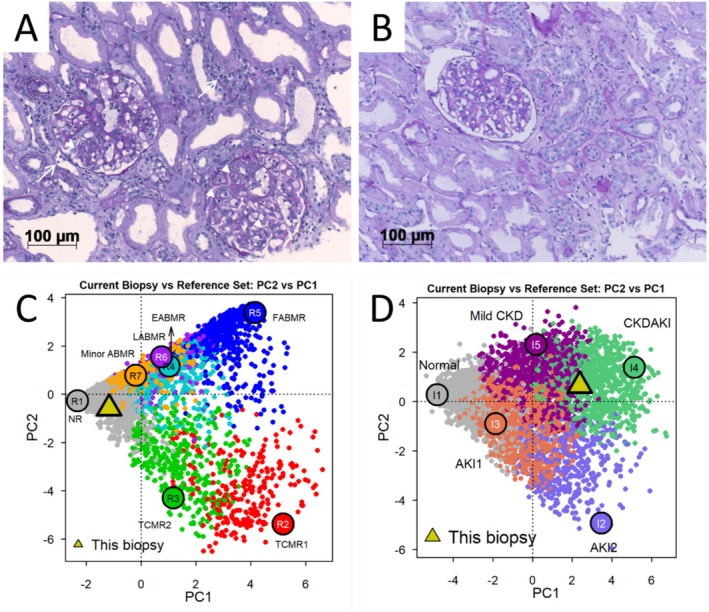 FIGURE 2
FIGURE 2| HLA locus | Donor | Recipient |
|---|---|---|
| A | *01:01, *68:01 | *01:01, *68:01 |
| B | *08:01, *44:02 | *08:01, *44:02 |
| C | *07:01, *07:04 | *07:01, *07:04 |
| DRB1 | *03:01, *11:01 | *03:01, *11:01 |
| DRB3 | *01:01, *02:02 | *01:01, *02:02 |
| DQA1 | *05:01, *05:01 | *05:01, *05:01 |
| DQB1 | *02:01, *03:01 | *02:01, *03:01 |
| DPA1 | *01:03 | *01:03, *02:07 |
|
|
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Transplantation Outcomes and Treatments · Organ and Tissue Transplantation Research · Renal Diseases and Glomerulopathies
Introduction
1
Antibody‐mediated rejection (AMR), histologically characterised by microvascular inflammation (MVI) in glomeruli and peritubular capillaries, is one of the most common causes of premature kidney allograft loss [1]. Several observational studies have highlighted the existence of MVI in the absence of detectable donor‐specific anti‐HLA antibodies (DSA) [2], raising strong interest in deciphering alternative mechanisms of alloreactivity in addition to T‐ and B cell‐mediated graft injury [3]. NK cells have recently emerged as a potent mediator of MVI [4, 5], strongly supported by clinical data showing that NK cell depletion by anti‐CD38 treatment can resolve MVI in the context of AMR [6]. NK cells recognise ‘missing self’, that is, the absence of own HLA molecules on donor cells, primarily via killer‐immunoglobulin‐like receptors (KIR). ‘Missing self’ has been traditionally linked to the expression of HLA class I molecules [7]. Herein, we present the case of an early severe and persistent kidney allograft rejection in a recipient with no detectable DSA exclusively mismatched in HLA‐DPB1, suggesting alternative and clinically relevant mechanisms of alloreactivity.
Materials and Methods
2
Treatment Protocol and Immunosuppression
2.1
Daratumumab was administered intravenously at a dose of 16 mg/kg body weight. Initially, the antibody was given weekly for 8 weeks, following every other week (16 weeks) and every 4 weeks thereafter [8]. The patient was notified about the off‐label use of daratumumab and gave written informed consent. Throughout daratumumab treatment, the patient was kept on triple immunosuppression with tacrolimus, mycophenolate‐mofetil, and prednisolone. Following the diagnosis of AMR, tacrolimus trough levels were kept between 8 and 10 μg/L until month 12 post‐transplantation and between 6 and 8 μg/L thereafter. Mycophenolate‐mofetil was kept at the maximum tolerable dose. Prednisolone was kept at 5 mg qd.
Renal Biopsies
2.2
Kidney biopsies were classified according to the Banff 2022 scheme [9]. The follow‐up biopsy 9 months after treatment initiation with daratumumab was also examined using the Molecular Microscope Diagnostic System (MMDx). Therefore, kidney biopsy tissue is analysed by measuring gene expression patterns using microarray technology. mRNA extracted from biopsy tissue hybridises to probes representing key transplant‐related genes. Machine learning algorithms compare these molecular profiles to a reference set of previously characterised biopsies to classify transplant rejection phenotypes such as T cell‐mediated rejection (TCMR) and antibody‐mediated rejection (AMR). In addition, scores for parenchymal injury, including acute kidney injury (AKI), irreversible atrophy and fibrosis, and probability of graft survival are calculated [10].
HLA‐Typing and HLA‐Antibody Detection
2.3
High‐resolution HLA typing of donor and recipient was performed according to the standards of the European Federation for Immunogenetics (EFI) using a CE‐certified NGS typing assay (MiaFora MFlex 11, SR‐800‐10534; Werfen) following the manufacturer's instructions. Sequencing was carried out on a MiSeq device (Illumina). Antibody testing was performed according to EFI standards. Anti‐HLA antibody detection was carried out using a screening assay for both HLA class I and II (Labscreen Mixed Class I + II, LSM12; One Lambda). The anti‐HLA antibody specificity of sera was determined using a single antigen assay for HLA class I (i.e., HLA‐A/B/C; LABScreen Single Antigen Assay, LS1A04; One Lambda) and HLA class II antigens (i.e., HLA‐DR/DQ/DP; LABScreen Single Antigen Assay, LS2A01; One Lambda). Tests were carried out according to the manufacturer's instructions and analysed on a Luminex Flexmap 3D flow analyzer (Luminex). A positive result for antibody specificities in Single Antigen bead array was defined as a baseline normalised MFI > 500.
Donor‐Derived Cell‐Free DNA
2.4
Donor‐derived cell‐free DNA levels (dd‐cfDNA) were determined by droplet digital PCR with preselected SNPs [11].
Case Report
3
In May 2023, a 48‐year‐old female with a 4‐year history of end‐stage renal disease due to hypertensive nephropathy received a first kidney transplant at our institution. High resolution (2‐field) HLA typing of donor and recipient revealed a complete HLA match between donor and recipient in HLA‐A, ‐B, ‐C, ‐DR, ‐DQA1, ‐DQB1 and ‐DPA1 with an isolated mismatch in HLA‐DPB1 (Table 1). There were no preformed DSA (Table S1). Induction therapy consisted of basiliximab followed by tacrolimus, mycophenolate mofetil and prednisolone maintenance immunosuppression. Blood type of donor and recipient was O. Cold and warm ischemia times were 17 h and 45 min, respectively. Due to CMV D+/R‐ high risk constellation, prophylaxis with valganciclovir was given for 3 months. From July 2023 on, a low‐level viremia for CMV was detected intermittently with a maximum of 710 copies/ml, without evidence for CMV disease. Throughout the therapy with daratumumab, no relevant CMV viremia was detected.
Graft function stabilised at an eGFR of 30–40 mL/min/1.73m^2^ (CKD‐EPI) 2 weeks after surgery when a first protocol biopsy revealed isolated glomerulitis (Table S2), that was not treated. Following several episodes of urinary tract infections, eGFR deteriorated to 20 mL/min/1.73m^2^ over the next months. In September 2023, another biopsy now showed severe C4d‐positive MVI with glomerulitis (g) and peritubular capillaritis (ptc) together with borderline changes (Banff lesion score: g3 ptc2 cg0 t1 i1 ti1 v0 ct1 cv1 aah3, C4d1) and 10% interstitial fibrosis and tubular atrophy (IFTA) (Table S2). Light microscopy showed no evidence for thrombotic microangiopathy (TMA, Figure S1A) and immunohistochemistry was minimally positive for C4d in the peritubular capillaries (Figure S1B). Luminex single antigen bead (SAB) testing was negative for DSA. In addition, non‐HLA antibodies (AT1R‐, Endothelin‐Receptor‐ and MICA‐Abs) were undetectable. Nevertheless, treatment with plasma exchange and intravenous immunoglobulins resulted in stabilisation of graft function (Figure 1). A biopsy 4 weeks after treatment revealed complete resolution of MVI but progression of IFTA to 20% (Table S2).
Impact of daratumumab (anti‐CD38) on graft function and albuminuria. Estimated glomerular filtration rate (eGFR in ml/min/1.73m2 according to CKD‐EPI) and urinary albumin/creatinine ratio (uACR in mg/g creatinine) during follow‐up. IVIG, intravenous immunoglobulins; PEX, plasma exchange.
In November 2023, a marked increase in albuminuria (1.7 g/g creatinine) triggered another biopsy showing recurrence of MVI (g2, ptc1) without C4d‐deposition but signs of chronic transplant glomerulopathy (cg2) (Figure 2A and Table S2). Luminex SAB testing was repeatedly negative for DSA during follow‐up (Table S1). After approval by the patient's health insurance, treatment with daratumumab was initiated in January 2024 following a protocol for multiple myeloma at a dose of 16 mg/kg body weight over 9 months. Daratumumab treatment resulted in a profound decrease in albuminuria and stabilisation of allograft function (Figure 1). Follow‐up biopsies 2 and 9 months after treatment initiation revealed complete resolution of MVI (Figure 2B and Table S2). Molecular analysis of the last biopsy revealed low molecular scores for overall rejection (0.24, range 0.0–1.0, upper limit of normal 0.30), T‐cell mediated rejection (TCMR) (0.06, range 0.0–1.0, upper limit of normal 0.10) and antibody‐mediated rejection (ABMR) (0.09, range 0.0–1.0, upper limit of normal 0.20, Figure 2C). The overall inflammation score was moderately increased (1.46, range −3.9 to 5.5, upper limit of normal −0.93) with a markedly elevated fibrosis score (0.8, range 0.0–1.0, upper limit of normal 0.30, Figure 2D), the latter consistent with the histomorphologic findings. Donor‐derived cell‐free DNA levels (dd‐cfDNA) were within normal limits (7 cp/mL; 0.1% of total cell‐free DNA), indicating no ongoing graft injury [12]. Daratumumab treatment was stopped in October 2024. At the last clinical follow up in August 2025, eGFR was stable at 22 mL/min/1.73m^2^ (CKD‐EPI) and albuminuria was low at 66 mg/g creatinine. Dd‐cfDNA levels remained low throughout follow‐up (not shown).
Histological and molecular resolution of microvascular inflammation on kidney biopsies before and after daratumumab treatment. Light microscopy before (A, biopsy #4 in Table S2) and after a 9 months course of daratumumab (B, biopsy #5 in Table S2) revealed glomerulitis (arrow heads) and peritubular capillaritis (arrows) in (A) that was absent in (B) (Periodic acid‐Schiff reaction, original magnification × 200). Molecular analysis after daratumumab treatment shown in principal component plots (PC2 vs. PC1) in relation to a set of reference biopsies (10). (C) The biopsy is classified as no rejection (yellow triangle). The coloured circles indicate archetype rejection phenotypes (R1: non‐rejecting; R2: TCMR 1; R3: TCMR 2; R4: early‐stage ABMR; R5: fully developed ABMR; R6: late‐stage ABMR; R7: minor ABMR). (D) Molecular analysis of injury archetypes indicates chronic kidney damage (CKD). The coloured circles indicate injury phenotypes (I1: normal; I2: AKI2; I3: AKI1; I4: CKDAKI; I5: mild CKD). ABMR, antibody‐mediated rejection; AKI, acute kidney injury; TCMR, T cell‐mediated rejection.
Discussion
4
We report on a kidney transplant patient with an isolated HLA‐DPB104*‐mismatch in the donor that unexpectedly developed fulminant early rejection with severe MVI in the absence of detectable DSA. Daratumumab treatment resulted in histological and molecular resolution of MVI and stabilisation of graft function. Our case is remarkable for several reasons. First, our patient was prioritised within the Eurotransplant Kidney Allocation System due to a ‘full‐house’ match in HLA‐A, ‐B and ‐DR but had early clinical rejection. Second, our case highlights the fluctuating nature of allograft pathology. Most biopsies were classified as C4d‐negative, DSA‐negative MVI as recently defined by the Banff 2022 classification [13]. Despite repeat Luminex SAB testing both before and after transplantation using a low MFI cutoff for positivity (500), we were unable to detect DSA against DPB104*. Given the C4d‐positivity in the second kidney biopsy, we cannot rule out the existence of subthreshold antibody levels targeting the graft endothelium as recently proposed to underlie DSA‐negative C4d‐positive AMR [14]. Although there is a statistically significant relation between DSA‐positivity and C4d deposition, a causal relationship has never been proven [9]. Other potential causes for C4‐positivity such as TMA [15] were histologically absent. Third, given the near complete HLA match, our case suggests alternative mechanisms of alloreactivity. Of note, the complete HLA class I match between donor and recipient also excludes classic ‘missing‐self’ recognition by NK cells via KIR. Recently, Böhmig et al. reported a statistically significant correlation between various NK cell‐associated gene polymorphisms and MVI independent of DSA [4]. As we did not explore these polymorphisms, we cannot rule out a role for, for example, the C‐type lectin NKG2C receptor or other, so far unknown, innate allorecognition molecules [3, 16]. Interestingly, the concept of ‘missing‐self’ recognition involving exclusively HLA class I was recently challenged by a paper reporting on potent NK cell‐mediated cytotoxicity towards HLA‐DPB104:01* via the natural cytotoxicity receptor NKp44 [17], the former being the only mismatched HLA in our patient. NKp44 is only expressed on the cell surface upon activation. NK cells might have been preactivated during the early episodes of urinary tract and subclinical CMV infection [18] in our patient, lending support to the concept of trained innate immunity [19]. Although speculative at this time, exploring the clinical relevance of isolated DPB104:01* mismatches might deserve further investigation. Finally, to our knowledge, this is the first reported case of DSA‐negative MVI with a clinical, histological and molecular response to a 9 months course of daratumumab, highlighting the potential of anti‐CD38 treatment strategies even in patients without detectable DSA.
Author Contributions
L.K., M.G., B.B. and D.Z. were responsible for the clinical treatment of the patient. M.B.‐H., M.L., B.S., M.O. and J.B. performed data analysis and contributed to the writing of the manuscript. L.K. and D.Z. wrote the manuscript.
Funding
The authors have nothing to report.
Consent
Informed consent was obtained from the patient for off‐label use of daratumumab and publication of this case report. All efforts were made to ensure patient anonymity.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Table S1: Results of Luminex single antigen bead (SAB) testing in chronological order. Table S2: Kidney biopsy results as retrieved from the original reports. Figure S1: Histology of Biopsy #2 with diagnosis of C4d‐positive AMR. (A) Light microscopy shows MVI (g3, ptc2).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Loupy and C. Lefaucheur , “Antibody‐Mediated Rejection of Solid‐Organ Allografts,” New England Journal of Medicine 379, no. 12 (2018): 1150–1160.30231232 10.1056/NEJ Mra 1802677 · doi ↗ · pubmed ↗
- 2J. Callemeyn , E. Lerut , H. de Loor , et al., “Transcriptional Changes in Kidney Allografts With Histology of Antibody‐Mediated Rejection Without Anti‐HLA Donor‐Specific Antibodies,” Journal of the American Society of Nephrology 31, no. 9 (2020): 2168–2183.32641395 10.1681/ASN.2020030306 PMC 7461663 · doi ↗ · pubmed ↗
- 3J. Callemeyn , B. Lamarthee , A. Koenig , P. Koshy , O. Thaunat , and M. Naesens , “Allorecognition and the Spectrum of Kidney Transplant Rejection,” Kidney International 101, no. 4 (2022): 692–710.34915041 10.1016/j.kint.2021.11.029 · doi ↗ · pubmed ↗
- 4M. Diebold , H. Vietzen , M. Schatzl , et al., “Functional Natural Killer‐Cell Genetics and Microvascular Inflammation After Kidney Transplantation: An Observational Cohort Study,” Transplantation 109, no. 5 (2025): 860–870.39402708 10.1097/TP.0000000000005228 PMC 12011434 · doi ↗ · pubmed ↗
- 5A. Koenig , S. Mezaache , J. Callemeyn , et al., “Missing Self‐Induced Activation of NK Cells Combines With Non‐Complement‐Fixing Donor‐Specific Antibodies to Accelerate Kidney Transplant Loss in Chronic Antibody‐Mediated Rejection,” Journal of the American Society of Nephrology 32, no. 2 (2021): 479–494.33239394 10.1681/ASN.2020040433 PMC 8054908 · doi ↗ · pubmed ↗
- 6K. A. Mayer , E. Schrezenmeier , M. Diebold , et al., “A Randomized Phase 2 Trial of Felzartamab in Antibody‐Mediated Rejection,” New England Journal of Medicine 391, no. 2 (2024): 122–132.38804514 10.1056/NEJ Moa 2400763 · doi ↗ · pubmed ↗
- 7K. Karre , “NK Cells, MHC Class I Molecules and the Missing Self,” Scandinavian Journal of Immunology 55, no. 3 (2002): 221–228.11940227 10.1046/j.1365-3083.2002.01053.x · doi ↗ · pubmed ↗
- 8K. Doberer , J. Klager , G. A. Gualdoni , et al., “CD 38 Antibody Daratumumab for the Treatment of Chronic Active Antibody‐Mediated Kidney Allograft Rejection,” Transplantation 105, no. 2 (2021): 451–457.32235256 10.1097/TP.0000000000003247 · doi ↗ · pubmed ↗