A survey of parental experiences and perceptions of NAVA in neonatal intensive care
Donna Tolentino, Laura De-Rooy, Anay Kulkarni, Sandeep Shetty

TL;DR
This study surveyed parents about their experiences with a breathing support method called NAVA in neonatal care, finding most felt it was comfortable and would recommend it.
Contribution
The study provides new insights into parental perceptions of NAVA in neonatal intensive care, focusing on comfort and willingness to recommend.
Findings
81% of parents felt staff explained breathing support modes clearly.
53% of parents felt their baby was calmer during NAVA compared to other modes.
78% of parents stated they were very likely to recommend NAVA.
Abstract
To evaluate parental perceptions and experiences of neurally adjusted ventilatory assist (NAVA) in neonatal intensive care, focusing on understanding, comfort, and willingness to recommend its use. A survey of parents whose infants received NAVA or Non-invasive ventilation (NIV) NAVA at a tertiary NICU between January 2024 and July 2025. St George’s University Hospitals NHS Foundation Trust, London, UK. Fifty parents were invited; 32 returned completed surveys (response rate: 64%). Parent-reported understanding of ventilation modes, perceptions of infant comfort and willingness to recommend NAVA. Most respondents (81%, n = 26) felt staff explained different modes of breathing support clearly; 4 (13%) found explanations unclear, and 2 (6%) received none. Seventeen (53%) parents felt their baby was calmer and more settled during NAVA/NIV NAVA compared with other modes; 11 (34%) noticed no…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
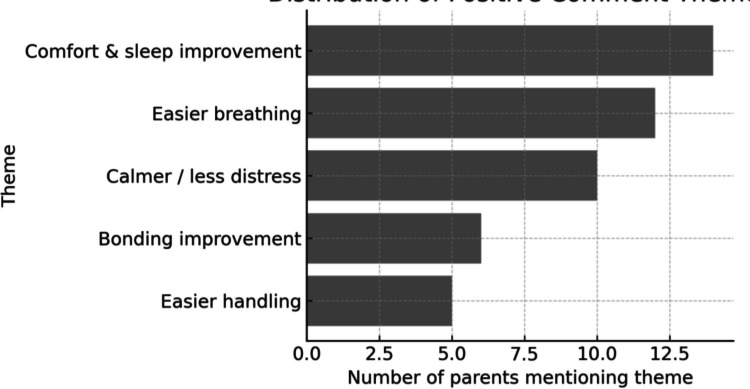 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal Respiratory Health Research · Infant Development and Preterm Care · Respiratory Support and Mechanisms
Introduction
Mechanical ventilation (MV), although lifesaving, is associated with chronic respiratory morbidity in both preterm and term born infants. New ventilation modes have been developed with the aim of minimising lung injury; these include invasive and non-invasive respiratory support strategies [1]. These can range from conventional invasive ventilation modes, such as pressure-regulated volume control (PRVC) and pressure control (PC) ventilation, to non-invasive methods, such as Heated, humidified, high-flow nasal cannula (HHFNC), continuous positive airway pressure (CPAP), non-invasive pressure control ventilation (NIV-PC) [1]. More recently, Neurally Adjusted Ventilatory Assist (NAVA) and its non-invasive variant (NIV-NAVA) have been introduced, offering a more synchronised form of support that uses the infant’s own diaphragmatic electrical activity to trigger and modulate breaths [2].
Studies comparing NAVA with conventional mechanical ventilation modes demonstrated that NAVA improved patient-ventilator interaction and comfort [3] and decreased peak inspiratory pressure (PIP) and mean airway pressure (MAP), work of breathing, oxygen requirement (FiO_2_) [4], sedation requirement [5] and episodes of apnoea [3]. Moreover, a review of ten studies comparing NAVA or NIV-NAVA to conventional respiratory support modes concluded that the application of NAVA appears to be safe and feasible in premature infants as no adverse events were reported [6]. In a randomised crossover study comparing NAVA with conventional ventilation modes in infants with evolving or established Bronchopulmonary Dysplasia (BPD), NAVA improved oxygenation by reducing oxygenation index (OI), FiO_2_, peak inspiratory pressure (PIP) and mean airway pressure (MAP) and compliance was higher [7]. In a retrospective case control study, infants with evolving BPD on NAVA/NIV NAVA had lower extubation failure rates (p = 0.002), shorter durations of invasive ventilation (p = 0.046), total duration of invasive and non-invasive ventilation (p = 0.026) and total length of hospital stay (p = 0.019). There were no significant differences, however, in the rates of BPD or home oxygen [7]. Data suggest that NAVA/NIV and NAVA ventilation in preterm infants improves their growth trajectory at the time of discharge, probably due to the improved synchronisation and patient comfort [8]. Evidence suggests that NAVA may reduce PIP, improve patient–ventilator synchrony, decrease the work of breathing, and promote greater comfort compared with conventional modes [7].
Effective communication between NICU staff and parents plays a central role in supporting families during their infant’s hospital journey [9]. The family-integrated care (FICare) model offers a framework to actively involve parents in the care of their baby during their neonatal unit admission and to encourage collaboration between parents and healthcare professionals [9]. In the context of advanced ventilation modes such as NAVA, providing clear information on how the mode works, and how this support might affect infant comfort and bonding is particularly important.
This survey was developed to capture the experiences of parents whose infants received NAVA or NIV-NAVA. By gathering these insights, this study aims to identify opportunities to improve communication, education, and support for families, while highlighting parental experience with advanced ventilatory care in neonates.
Methods
NAVA was introduced at St George’s Hospital in June 2019. Since then, a total of 200 patients received NAVA/NIV NAVA. For this survey, we targeted parents of infants who had been offered NAVA between January 2024 and July 2025, to minimise recall bias. Parents of infants who had died were not contacted, in line with ethical considerations. Eligibility was confirmed by cross-referencing records with the neonatal database (BadgerNet).
An online questionnaire (Appendix S1) designed in collaboration with a neonatal psychologist, accessible via a QR code linking to Google Forms, was distributed by post to 50 eligible parents. The survey explored parents’ recollections of the different respiratory support modes used, their understanding of how these methods help their baby, and their perceptions of their baby’s comfort and interaction during NAVA compared with other modes. It also examined views on the NAVA-specific feeding tube and willingness to recommend NAVA to others. Demographic details were also collected.
Data obtained were analysed descriptively, with results presented as percentages. Where appropriate, bar plots were used to visualise the distribution of responses.
This project was registered as an audit with St George’s University Hospitals NHS Foundation Trust Audit Department (Registration number AUDI004527).
Results
A total of 50 parents were invited to participate; 32 completed surveys were returned (response rate: 64%) (Table 1). Parents reported their infants had received various forms of respiratory support during admission, including NAVA (n = 24, 75%), NIV NAVA (n = 26, 81%), PRVC (n = 23, 72%), CPAP (n = 22, 69%), pressure control (PC) ventilation (n = 19, 59%), and NIV PC (n = 23, 72%); 3 (9%) parents reported other modes. Most respondents (81%, n = 26) felt staff explained different modes of breathing support clearly; 4 (13%) found explanations unclear, and 2 (6%) received none. Seventeen (53%) parents felt their baby was calmer and more settled during NAVA/NIV NAVA compared with other modes; 11 (34%) noticed no difference, and 4 (13%) perceived less comfort. The NAVA catheter scored a mean of 3.77/5 for comfort. Positive observations included “longer, deeper sleep,” “less fighting the machine,” and “breathing seemed easier” (Fig. 1). Twenty-three parents (78%) stated they were “very likely” to recommend NAVA, 5 (16%) were “likely,” 1 (6%) was “neutral,” and 2 (12%) would not recommend it. Respondents included mothers (n = 19, 59%), fathers (n = 3, 9%), and both parents together (n = 10, 31%). Ethnic backgrounds included Black Caribbean, Black British, and White/Other. Table 1. Parent survey responses (n = 32)Outcome categorySubcategoryn (%)Breathing support modesNAVA24 (75)NIV NAVA26 (81)PRVC23 (72)CPAP22 (69)Pressure support ventilation19 (59)NIV PC23 (72)Other modes3 (9)Staff explanationsClear/good understanding26 (81)Unclear4 (13)None2 (6)Comfort (NAVA/NIV NAVA)More comfortable17 (53)Less comfortable4 (13)No difference11 (34)NAVA catheter comfortMean (SD) score (1–5)3.77RecommendationVery likely23 (72)Likely5 (16)Neutral1 (3)Unlikely2 (6)Fig. 1. Distribution of Free-text Responses Themes
Discussion
This single-centre survey found that parents whose infants received NAVA or NIV-NAVA generally perceived these modes as providing improved comfort compared with conventional ventilation. More than half of respondents reported their infant was calmer on NAVA-based support. Qualitative comments suggested perceived benefits of NAVA included longer sleep periods, reduced visible effort of breathing, and greater overall calmness. While subjective, such perceptions are aligned with clinician observations of reduced respiratory drive variability and more stable breathing patterns in infants on NAVA [10]. Continuous electrical activity of the diaphragm (Edi) catheter readings and ventilatory parameters recorded during 65 skin-to-skin contact (SSC), peak Edi (µV) was significantly reduced at end SSC (median 11.5 [2.7–38.7] vs. 15.8 [4.0–36.6], p < 0.001), as was mean airway pressure (Pmean, cmH₂O) (9.7 [7.3–15.4] vs. 10.3 [7.5–15.5], p = 0.008), and respiratory rate (breaths/min) (52.9 [31.1–78.1] vs. 53.4 [35.1–74.1], p = 0.031) [11].
The majority of respondents felt that staff explained breathing support modes clearly, underscoring the role of effective communication in supporting family-centred care [12].
The high proportion (72%) who were “very likely” to recommend NAVA to others indicates overall satisfaction, and this is consistent with wider evidence linking perceived infant comfort to parental satisfaction [11, 13]. Family experience is increasingly recognised as an important quality metric in neonatal care [14]. Although our survey was not designed to assess clinical outcomes, positive parental perceptions may contribute to enhanced parent–infant bonding and participation in care, which are themselves associated with improved developmental and psychosocial outcomes [15].
This study has limitations. The sample size was modest and limited to a single centre, and participation was restricted to parents whose infants survived to discharge. Recall bias may have influenced responses, though the survey was timed to minimise long-term recall error. Despite these limitations, the findings highlight the value of integrating parental perspectives into evaluations of respiratory support modalities. We reported quantitative and qualitative data, which gave a more comprehensive understanding of visiting policies.
In conclusion, parents perceived NAVA and NIV-NAVA as providing greater comfort and valued clear staff communication. As NICU care moves towards more personalised and family-centred approaches, incorporating parental perspectives into assessments of new technologies will be essential for ensuring that innovation meets both clinical and family needs.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary Material 1 (PDF 153 KB)