Postmastectomy radiation therapy for autologous breast reconstruction: a systematic review and meta-analysis for the 2022 Japanese Breast Cancer Society Clinical Practice Guideline
Mami Ogita, Subaru Sawayanagi, Haruka Jinnouchi, Michio Yoshimura, Chikako Yamauchi, Naoko Sanuki, Yasushi Hamamoto, Kimiko Hirata, Mariko Kawamura, Yutaka Yamamoto, Shigehira Saji, Tatsuya Toyama

TL;DR
This study reviews the safety of radiation therapy after breast reconstruction, finding it increases fat necrosis risk but not major complications.
Contribution
A systematic review and meta-analysis on PMRT safety after autologous breast reconstruction for the 2022 Japanese Breast Cancer Society guidelines.
Findings
PMRT was not significantly associated with major complications (OR 1.58, P = 0.09).
PMRT significantly increased fat necrosis risk (OR 2.71, P = 0.0003).
Cosmetic outcomes data were limited and not pooled.
Abstract
The safety of postmastectomy radiation therapy (PMRT) after autologous breast reconstruction remains unclear. Therefore, we conducted a systematic review and meta-analysis to investigate the effects of PMRT on patients with breast cancer who underwent autologous breast reconstruction. A comprehensive literature search of English and Japanese articles until March 2021 was performed using PubMed/MEDLINE, the Cochrane Library, and Ichushi-Web. We included studies that compared the outcomes of patients with breast cancer who underwent immediate autologous breast reconstruction with and without PMRT. Outcomes including major complications, fat necrosis, and cosmetic results were assessed. Pooled odds ratios (OR) with 95% confidence intervals (CI) were calculated using a random effects model. Ten studies (two retrospective case-controlled and eight retrospective cohort studies) comprising…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
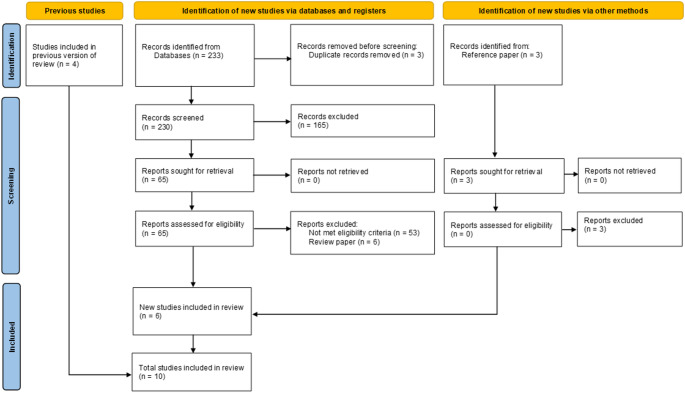 Figure 1
Figure 1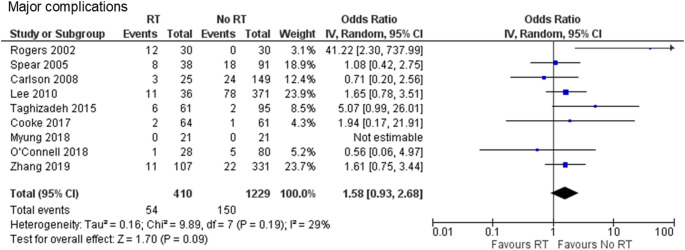 Figure 2
Figure 2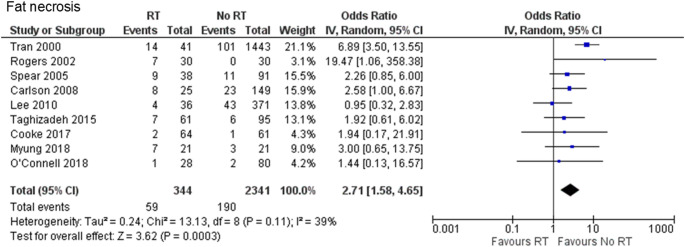 Figure 3
Figure 3- —The University of Tokyo
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Implant and Reconstruction · Reconstructive Surgery and Microvascular Techniques · Lymphatic System and Diseases
Introduction
Over the years, the number of patients undergoing breast reconstruction has been increasing [1]. Two major methods for breast reconstruction after mastectomy are available: autologous reconstruction, wherein the patient’s own tissue such as skin, fat, and blood vessels are used, and implant-based prosthetic reconstruction, which utilizes silicone implants to recreate the breast shape. Depending on the situation, a combination of implants and autologous flaps can also be used. Autologous breast reconstruction has several advantages over implant-based prosthetic reconstruction. Autologous breasts appear to be more natural and last a lifetime with a single procedure. With no risk of rejection or allergic reactions, concerns regarding implant-related issues are alleviated. Additionally, autologous reconstruction results in higher satisfaction with both the overall outcome and the breast itself and may also reduce the risk of infection and surgical complications [2–4]. The patients chose the reconstruction type based on their health and personal preferences.
A substantial proportion of patients undergoing breast reconstruction after mastectomy require post-mastectomy radiation therapy (PMRT). This therapy has been shown to reduce breast cancer recurrence and mortality in patients with high-risk features, such as positive axillary lymph nodes [5–12]. However, PMRT may be associated with an increased risk of reconstruction-related complications and may negatively affect patient-reported quality of life [13].
Among the various breast reconstruction options available following mastectomy, autologous breast reconstruction is generally considered more resilient to the adverse effects of radiation than implant-based reconstruction. A prospective study showed that autologous reconstruction yielded better patient-reported satisfaction and a lower risk of complications than did implant-based reconstruction in patients undergoing PMRT [14]. Nonetheless, the effect of PMRT on autologous reconstructed breast tissue remains a concern. Several studies have reported that PMRT adversely affects reconstructed breasts. A meta-analysis by Schaverien et al. in 2013 explored this issue and reported no significant differences in the overall complications and revision surgery between patients receiving PMRT and those who did not, although a significantly increased risk of fat necrosis was noted in the PMRT group [15]. Given that the existing evidence is limited and outdated too, particularly with respect to evolving oncoplastic techniques and advancements in radiotherapy, a comprehensive and updated assessment is warranted. Therefore, we conducted an updated systematic review and meta-analysis to evaluate the effect of PMRT on patients undergoing autologous breast reconstruction.
Materials and methods
The results are reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. The meta-analysis was conducted as a part of the development of the Japanese Breast Cancer Society’s Clinical Practice Guidelines for Radiation Treatment of Breast Cancer, 2022 edition [17].
Eligibility criteria
We included all randomized or non-randomized controlled trials as well as prospective or retrospective observational studies that evaluated the effect of PMRT on immediate autologous breast reconstruction in breast cancer patients. Articles comparing irradiated and non-irradiated autologous reconstructed breasts groups were included. Review articles, case reports with fewer than 10 patients in one arm, single-arm studies, studies reporting delayed breast reconstruction (breast reconstruction performed after PMRT), and studies that did not assess the outcomes specified for this review were excluded. The studies were limited to those published in English or Japanese.
Search strategy
The PubMed/MEDLINE, Cochrane Library, and Ichushi-Web databases were systematically searched from January 2016 to March 2021. A combination of MeSH terms and keywords, including “Breast Neoplasms,” “Radiotherapy,” “Mammaplasty,” “Autografts,” “Transplantation, Autologous,” “Breast Implants,” and “Breast Reconstruction,” were used for the literature search (Supplementary Table 1). Additionally, we manually searched the reference lists of the relevant review articles. This review is an updated version of a previous systematic review and meta-analysis conducted in 2018 according to the Japanese Breast Cancer Society’s clinical practice guidelines for breast cancer [9]. The previous systematic review and meta-analysis was performed by searching PubMed/MEDLINE, the Cochrane Library, and Ichushi-Web from the earliest dates until November 2016. Studies selected from the previous meta-analysis were rereviewed and combined in this analysis.
Selection and data collection process
Two reviewers (SS and HJ) independently reviewed the titles and abstracts from the initial screening. Subsequently, the same two reviewers (SS and HJ) screened the articles by reviewing their full texts. Data were extracted by two independent reviewers (SS and HJ) using a standardized form. Any disagreements were resolved through discussions between the two reviewers (SS and HJ), and if no consensus was reached, a third reviewer (MO) intervened to resolve the issue.
Outcomes
We assessed major complications, fat necrosis, and cosmesis as the primary outcomes. Major complications were defined as those requiring surgical intervention and/or hospitalization. Any instance of fat necrosis, regardless of its severity, was categorized as ‘fat necrosis’ in this analysis. Regarding cosmesis, outcomes categorized as “good” or “better” were considered acceptable, while those rated below “good” were regarded as a decline in cosmesis.
Study risk of bias and certainty assessment
The risk of bias in non-randomized studies was assessed using the Medical Information Distribution Service (Minds) tool [18For each study, two independent reviewers (SS and HJ) evaluated six domains—baseline differences, care differences, outcome measurement, follow-up completeness, confounding adjustment, and other bias—on a scale of high risk (− 2), some concerns (− 1), or low risk (0). Disagreements were resolved by consensus. An overall study-level judgement was assigned according to the Minds manual. A study is classified as “very serious risk” when most domains are scored − 2, as “serious risk” when the domain ratings are mixed (0/−1/−2), and as “no risk” when most domains are scored 0. The levels of indirectness, inconsistency, imprecision, and publication bias were evaluated for each study, and a body of evidence was established for each outcome.
Data synthesis
We performed a meta-analysis to compare outcomes between patients receiving PMRT to the autologous reconstructed breast and those not receiving PMRT. Odds ratios (OR) and the corresponding 95% confidence intervals (CI) were calculated using random effects models and the inverse-variance method. To account for temporal changes in PMRT techniques, we conducted sensitivity analyses excluding pre-2000 cohorts, using the same random-effects model as the primary analysis. Publication bias was assessed using funnel plots. All tests were two-sided, and a p-value < 0.05 was considered statistically significant. Statistical analysis was performed using Review Manager (RevMan) v5.4 software by the Cochrane Collaboration.
Results
Study selection and characteristics
Our search identified a total of 233 articles. After removing three duplicates, 230 citations remained for screening. We excluded 165 citations after the initial screening and proceeded with the full-text screening of 65 studies. Further, 59 studies were excluded because they did not meet the eligibility criteria. This meta-analysis was conducted with 10 studies, including 6 from the current literature search and 4 from previous analyses. Figure 1 shows the flow diagram of the study selection process. Two retrospective case-control [19, 20] and eight retrospective cohort studies [21–28] were included in this meta-analysis. The study characteristics are summarized in Table 1.
Fig. 1. Flow diagram of literature screening according to PRISMA 2020
Table 1. Characteristics of the included studiesStudyInstitutionStudy PeriodStudy DesignNumber of Patients or Flaps for AnalysisFollow-up Period (Months)Type of Autologous ReconstructionRT Dose to the Reconstructed Breast (Gy)BoostBolusTran, NV. 2000The University of Texas M. D. Anderson Cancer Center, US1988–1998Retrospective CohortTotal 1484RT 41,No RT 1443NATRAMMean 50.99NANARogers, NE. 2002Memorial Medical Center in New Orleans, US1994–1999Case-ControlTotal 60RT 30,No RT 30MedianRT 19.9,No RT 17.4DIEPMean 50.5(range 44.0-61.2)NANASpear, SL. 2005Georgetown University Hospital, US1988–1999Retrospective CohortTotal 129RT 38,No RT 91NATRAMNANANACarlson, GW. 2008Emory University School of Medicine, USNARetrospective CohortTotal 174RT 25,No RT 149NATRAMNANANALee, BT. 2010Guy’s and St Thomas’ NHS Foundation Trust, UK1999–2006Retrospective CohortTotal 407RT 36,No RT 371MedianRT 63.6,No RT 56.8LD, TRAM, DIEP, SIEA, SGAPNANANATaghizadeh, R. 2015Memorial Sloan Kettering Cancer Center, USNARetrospective CohortTotal 156RT 61,No RT 95MeanRT 33.3,No RT 32.9DIEP40–50Yes (few)NACooke, AL. 2017CancerCare Manitoba, Canada2012–2015Substudy of Prospective CohortTotal 125RT 64,No RT 61NADIEP, SIEA50-50.433%NAMyung, Y. 2018Seoul National University Bundang Hospital, Korea2012–2016Retrospective Propensity Score Matched Case-Control StudyTotal 42RT 21,No RT 21NATRAM, DIEPMean 52.4NAYes (if necessary)O’Connell, RL. 2018The Royal Marsden NHS Foundation Trust, UK2009–2014Retrospective CohortTotal 108RT 28,No RT 80MedianRT 27.5,No RT 48.7DIEP40NAYes (only 1 case)Zhang, L. 2019Fudan University Shanghai Cancer Center, China2001–2015Retrospective CohortTotal 438RT 107,No RT 331NANANANANART: radiation therapy; NA: Not Applicable; TRAM: transverse rectus abdominis musculocutaneous; DIEP: deep inferior epigastric perforators; LD: latissimus dorsi; SIEA: superficial inferior epigastric artery; SGAP: superior gluteal artery perforator
Risk of bias assessment
Risk of bias was assessed using the Minds approach by two independent reviewers with consensus resolution, rating six domains on a 0/−1/−2 scale. The included studies were not blinded or randomized, as they were observational in nature, and only two studies were adjusted for confounding factors. Using the Minds criteria, most studies were judged to have a serious overall risk of bias, driven mainly by unblinded outcome assessment and heterogeneous adjustment practices,with additional concerns regarding baseline imbalances and care differences. Detailed domain-level ratings for each outcome are provided in Supplementary Tables 2 and 3. Both indirectness and inconsistency were low for all outcomes. A publication bias was noted for fat necrosis (Supplementary Figs. 1 and 2).
Results of synthesis
Major complications
Two retrospective case-control [19, 20] and seven retrospective cohort studies [22–28] were included. A total of 1,639 cases were analyzed, including 410 and 1,229 cases in the PMRT and no-PMRT groups, respectively. Major complications were documented to occur in 13.2% of cases in the PMRT group and 12.2% in the no-PMRT group (OR 1.58, 95% CI 0.93–2.68, P = 0.09), with no heterogeneity (Chi^2^ = 9.89, df = 7, P = 0.19, I^2^ = 29%) (Fig. 2).
Fig. 2. Forest plot illustrating the impact of PMRT on major complications. PMRT: postmastectomy radiation therapy; IV: inverse-variance
Fat necrosis
Two retrospective case-control [19, 20] and seven retrospective cohort studies [21–27] were included to evaluate fat necrosis. A total of 2,685 cases were analyzed (344 and 2,341 in the PMRT and no-PMRT groups, respectively). Fat necrosis occurred significantly more frequently in the PMRT group than in the no-PMRT group (17.2% vs. 8.1%, OR 2.71, 95% CI 1.58–4.65, P = 0.0003), with no heterogeneity (Chi^2^ = 13.13, df = 8, P = 0.11, I^2^ = 39%) (Fig. 3).
Fig. 3. Forest plot illustrating the impact of PMRT on fat necrosis. PMRT: postmastectomy radiation therapy; IV: inverse-variance
Sensitivity analysis
In sensitivity analyses that excluded pre-2000 cohorts, the results remained consistent with the primary analysis, and the conclusions did not change. There was no significant difference in major complications; however, the PMRT group exhibited a higher risk of fat necrosis (Supplementary Fig. 3 and 4). There was no evidence of publication bias for major complications or fat necrosis (Supplementary Fig. 5 and 6).
Cosmesis
Due to insufficient and heterogeneous reports, a meta-analysis of cosmetic decline could not be performed.
Certainty of evidence
Supplementary Table 4 presents evidence for each outcome. The certainty of evidence was low for all outcomes.
Discussion
In this study, we evaluated the effect of PMRT on adverse events in patients with breast cancer who underwent autologous breast reconstruction following mastectomy. Although PMRT was not associated with an increased rate of major complications, it increased the rate of fat necrosis.
Despite a comprehensive literature search, we were unable to find randomized controlled studies of PMRT in patients with breast cancer undergoing autologous breast reconstruction. The indication for PMRT is determined by the disease status, making randomization of the intervention impractical towards clarifing the impact of PMRT on reconstructed breasts. High-quality evidence does not currently exist, and is unlikely to be produced in the future. Available evidence on the effect of PMRT on autologous reconstructed breast tissues is limited. Because no randomized trials exist and the available evidence comes from observational studies, we combined the best available data to estimate pooled effects and their uncertainty. We interpret these findings with caution, acknowledging that residual confounding exists in observational studies. Despite the limited certainty of individual observational studies, a transparently conducted meta-analysis remains useful: it synthesizes evidence from multiple cohorts, clarifies the direction and approximate magnitude of effects, and explicitly reports remaining uncertainties and study limitations.
Among the studies, the rates of major complications varied between 0.0% and 40.0% in the PMRT group and from 0.0% to 21.0% in the no-PMRT group. Most studies included in our analysis did not show statistically significant differences in major complications between the two groups. An exception was the study by Rogers et al. [19], according to which the major complication rate was significantly increased with PMRT (23.3% vs. 0%, OR 41.2, 95% CI 2.3–738.0). However, the study was conducted between 1994 and 1999, and the techniques used for breast reconstruction and radiation therapy are now considered outdated. Therefore, the differences in the complication rates may have been more pronounced.
A previous meta-analysis by Schaverien et al. (2013) demonstrated a significantly increased risk of fat necrosis in patients receiving PMRT compared to those without PMRT (OR 2.8, 95% CI 1.4–5.9, p = 0.006), while no significant differences were observed in overall adverse events (OR 1.1, 95% CI 0.8–1.5, p = 0.59) or revisional surgery (OR 0.7, 95% CI 0.3–1.7, p = 0.38) [15]. Our updated meta-analysis included recently published studies and conducted a formal assessment of the study quality and risk of bias. Our results are consistent with those of Schaverien et al., and confirm a significantly increased incidence of fat necrosis associated with PMRT, while showing no significant increase in major complications. We also conducted sensitivity analyses excluding pre-2000 cohorts to account for differences in PMRT techniques as practice evolved from 2D to CT-based 3D-CRT/IMRT. The pooled estimates and their interpretation were consistent with those of the primary meta-analysis. This supports the robustness of our findings and their relevance to current practice.
Patient and treatment-related factors likely contribute to the variability in adverse events across studies. Obesity and diabetes are associated with an increased risk of complications in autologous reconstruction [29], while smoking increases wound-related complications, including flap/fat necrosis [30]. Chemotherapy has been associated with increased rates of fat necrosis in some cohorts, but findings are inconsistent [31, 32]. Additionally, reconstructive techniques alter risk profiles: meta-analyses report differences in fat necrosis and related events between pedicled TRAM flaps, free TRAM flaps, and DIEP flaps [33]. Because these variables were inconsistently reported and rarely adjusted for in the included studies, our pooled estimates should be interpreted with caution.
Although we did not have sufficient data to analyze cosmetic outcomes, several cohort studies suggest that PMRT adversely affects aesthetic appearance after autologous reconstruction. In a propensity-matched series, a decline in cosmesis (fair or poor) was observed in 7 of 21 patients (33.3%) after PMRT, compared to 2 of 21 patients (9.5%) without PMRT. Additionally, flap volume decreased by 12.3% after PMRT, compared to a 2.6% decrease in no PMRT group (P < 0.01) [20]. In a cohort using pedicled TRAM flaps with blinded reviewer assessments, PMRT was associated with worse overall aesthetic appearance, symmetry, and greater contracture compared to no PMRT [22]. Blinded photographic evaluations also revealed declines in scores for symmetry, superior-pole contour, and overall proportion in irradiated flaps, while scores improved in non-irradiated controls [19]. A systematic review by Shah et al. concluded that PMRT may worsen cosmetic outcomes in autologous reconstructions, although this has not been definitively proven. Volumetric findings are inconsistent across techniques [34]. In a DIEP-specific cohort, PMRT did not significantly affect flap volume [35]. These data indicate that PMRT may negatively affect cosmesis in at least some autologous reconstructions, though the extent likely varies by flap type, technique, and study populations. To clarify the effect of PMRT, larger studies employing standardized aesthetic endpoints and validated patient-reported outcome measures are warranted.
The patients who underwent immediate implant-based reconstruction with PMRT had a higher risk of reconstruction failure and reported lower satisfaction than those who underwent immediate autologous reconstruction [36]. A recent meta-analysis examining adverse events between patients who underwent immediate implant-based and autologous breast reconstruction in the context of PMRT found that patients who underwent implant-based reconstruction experienced more reconstruction failures than those who underwent autologous reconstruction (RR = 8.61, 95% CI: 2.84–26.08, P < 0.05) [37]. Because PMRT for autologous breast reconstruction seems safer than PMRT for prosthetic breast reconstruction, autologous reconstruction may be a more suitable option for patients who require PMRT and wish to undergo breast reconstruction.
This study had several limitations. First, most of the included studies were retrospective in nature, which may carry a risk of selection bias, unmeasured confounding factors, and limitations in data accuracy. Second, differences in reconstructive techniques within autologous breast reconstruction, such as deep inferior epigastric perforator (DIEP), transverse rectus abdominis musculocutaneous (TRAM), and latissimus dorsi flaps, were not analyzed separately. These technique differences may influence the rate of fat necrosis and other complications. Third, the severity of fat necrosis was not distinguished between minor, asymptomatic fat necrosis, and more severe cases requiring intervention, which may have different clinical implications.
In conclusion, although PMRT for autologous breast reconstruction may increase the incidence of fat necrosis, no significant increase in the incidence of major complications was observed. These findings suggest that PMRT is a safe and acceptable treatment option for patients undergoing autologous breast reconstruction. However, given methodological limitations and variability across studies, the applicability and certainty of these conclusions are limited and should be interpreted with caution. Although PMRT should be considered when indicated, clinicians are encouraged to discuss the potential risks of increased complications with patients.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1National Comprehensive Cancer Network. Nccn web site. Nccn practice guidelines in oncology—v.2.2024: Breast cancer. https://www.Nccn.Org/professionals/physician_gls/pdf/breast.Pdf. Accessed apr 13, 2024.
- 2Overgaard M, Jensen MB, Overgaard J, Hansen PS, Rose C, Andersson M et al. Postoperative radiotherapy in high-risk postmenopausal breast-cancer patients given adjuvant tamoxifen. Danish breast cancer cooperative group Dbcg 82c randomised trial. Lancet 1999;353:1641-8.10.1016/S 0140-6736(98)09201-010335782 · doi ↗ · pubmed ↗
- 3Overgaard M, Hansen PS, Overgaard J, Rose C, Andersson M, Bach F et al. Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. Danish breast cancer cooperative group 82b trial. N Engl J Med 1997;337:949-55.10.1056/NEJM 1997100233714019395428 · doi ↗ · pubmed ↗
- 4Yoshimura M, Yamauchi C, Sanuki N, Hamamoto Y, Hirata K, Kawamori J et al. The Japanese breast cancer society clinical practice guidelines for radiation treatment of breast cancer, 2022 edition. Breast Cancer 2024;31:347-57.10.1007/s 12282-024-01568-4PMC 1104556538578563 · doi ↗ · pubmed ↗