A Case of an 80-Year-Old Woman With Chronic Eosinophilic Pneumonia and Clinically Significant Giant Hepatic Hemangioma
Vicken Khazar, Samuel Escobar, Amy Huang, Anthony M Szema

TL;DR
An 80-year-old woman with multiple health issues had a large, growing hepatic hemangioma that did not require surgery due to her age and comorbidities.
Contribution
This case highlights the management of a mega hepatic hemangioma in an elderly patient with multiple comorbidities, emphasizing non-intervention when surgery is not feasible.
Findings
The patient's hepatic hemangioma increased in size over eight years but did not require surgical intervention.
Despite meeting criteria for resection, the patient was managed with observation due to her age and comorbidities.
The case suggests that elderly patients with comorbidities can tolerate large hemangiomas without surgery.
Abstract
An 80-year-old woman with a history of chronic eosinophilic pneumonia (CEP), severe persistent asthma, concomitant severe idiopathic urticaria, fibrous dysplasia of bone, osteoporosis resulting from years of oral corticosteroid usage, and arthralgia, presented to the allergy and immunology clinic with abdominal discomfort. Abdominal and pelvic CT scan showed a hepatic hemangioma, measuring approximately 8.2 x 6.4 cm. The patient underwent arterial embolization with no improvement in size or symptoms. CT scan of the same area taken eight years later had the same large, well-defined hypodense lesion in the right hepatic lobe that increased in size to 10.5 x 7.3 cm. The larger hemangioma now resulted in a mass effect on the upper pole of the right kidney, encroaching on the second portion of the duodenum, and pushing the vertebral column to the left. The patient’s CEP was well controlled…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1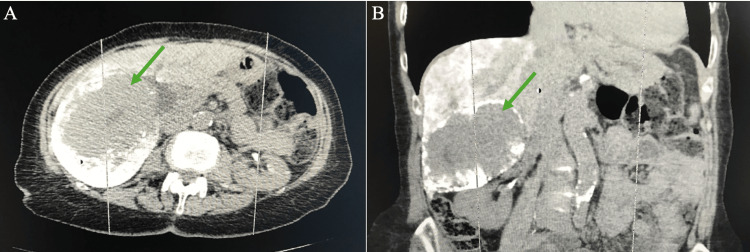 Figure 2
Figure 2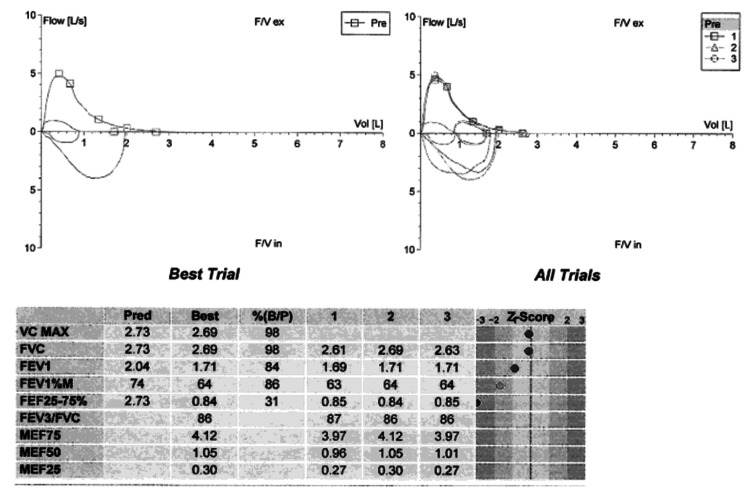 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Tumors and Angiosarcomas · Hepatocellular Carcinoma Treatment and Prognosis · Medical Imaging and Pathology Studies
Introduction
Hepatic hemangiomas (HH) are thought to be vascular malformations characterized by disorganized cavity enlargement via dilation, as opposed to hyperplasia or hypertrophy, and result in abnormal growth of blood vessels within the liver. They are the most common benign hepatic tumor at encompassing 20% of cases, typically present in individuals ages 30-50 years, and are more common in women than men [1-2].
While most HHs are small and benign, these tumors are considered “giant” when their diameter exceeds 5 cm and “enormous” when greater than 15cm. Hemangiomas are most commonly asymptomatic and are found incidentally on unrelated radiologic imaging, falling in the tumor category of “incidentalomas,” with a median age of presentation at 46 years old [1,3]. When giant hemangiomas present symptomatically, it is most often with abdominal pain or discomfort, early satiety, nausea, dyspnea, and postprandial bloating. Symptomatic HH warrants further workup for informed management [3].
Although the etiology of HH formation and progression is poorly understood, their enlargement has been associated with increased exposure to estrogen and progesterone, as in the setting of hormone replacement therapy (HRT), hormonal contraceptive use, and pregnancy. Given this, HHs are still seen in those without increased exposure to estrogen and progesterone, such as those not taking HRT or, as in our patient’s case, post-menopausal [1,4]. Despite being a relatively non-rare benign tumor, there is considerable interest in characterizing the epidemiology, progression, and modes of management of HHs given their unpredictable growth patterns, often vague symptoms, and potential for complications [5].
Chronic eosinophilic pneumonia (CEP) is a rare interstitial lung disease defined by marked eosinophilic infiltration of the alveolar spaces and pulmonary interstitium, leading to chronic pulmonary inflammation. Patients often develop symptoms over weeks to months, including progressive dyspnea, cough (often non-productive), low-grade fever, night sweats, weight loss, fatigue, and sometimes wheezing - though a history of asthma or atopy is common but not required [6]. On imaging, CEP typically manifests as bilateral peripheral or subpleural consolidations and/or ground-glass opacities on high-resolution CT or chest radiograph - sometimes described as a “photographic negative of pulmonary edema [7]." Bronchoalveolar lavage (BAL) frequently demonstrates marked eosinophilia (often ≥ 40 % of cells), which, in the correct clinical and radiologic context, may obviate the need for lung biopsy [8]. Treatment with systemic corticosteroids usually results in rapid clinical and radiographic improvement, often within days to a few weeks. However, relapse is common: long-term follow-up studies indicate that a substantial proportion of patients (≈ 50-60 %) require prolonged low-dose maintenance therapy to prevent recurrence. Over time - particularly in patients with repeated relapses - some may develop persistent impairment in pulmonary function, such as reduced diffusing capacity (DLCO) or airflow obstruction, underscoring the importance of long-term monitoring [9].
Case presentation
Our patient is an 80-year-old woman with a history of CEP, severe persistent asthma, severe idiopathic urticaria, fibrous bone dysplasia, arthralgia, osteoporosis, and resected papillary thyroid carcinoma who presented to the clinic with abdominal discomfort, early satiety, and increased dyspnea on exertion.
Initial abdominal CT scans from 2018 showed a hepatic hemangioma measuring approximately 8.2 x 6.4 cm (Figure 1). She underwent arterial embolization with no improvement in size or symptoms. Follow-up CT scan of the same area taken eight years later demonstrated that the same large well-defined hypodense lesion in the right hepatic lobe had increased in size to 10.5 x 7.3 cm (Figure 2). The hemangioma now resulted in a mass effect on the upper pole of the right kidney, encroaching on the second portion of the duodenum, and pushing the vertebral column to the left. Her transaminase testing was within normal limits with aspartate aminotransferase (AST) and alanine aminotransferase (ALT) levels at 15 IU/L (4-40 IU/L) and 9 IU/L (4-41 IU/L), respectively.
Initial axial CT of the abdomen demonstrates a hemangioma (red tracing) measuring 8.2 x 6.4 cm.
CT of abdomen with transverse (A) and sagittal (B) views taken after liquid embolization with lipiodol and bleomycin, 8 years after initial CT. Hepatic hemangioma (green arrow) measures approximately 10.3 x 7.3 cm.
Although her CEP and asthma have been well controlled with reslizumab, when she presented with her new onset abdominal discomfort, early satiety, and dyspnea on exertion, her spirometry results indicated worsened obstructive ventilatory defect despite her having normal lung volumes and diffusing capacity (Figure 3).
Spirometry indicates an obstructive ventilatory defectFVC: Forced vital capacity; FEV1: Forced expiratory volume in 1 second; FEF: Forced expiratory flow
Discussion
Surgical intervention is common among patients presenting with a giant hepatic hemangioma to prevent the possibility of spontaneous rupture, resulting in peritoneal cavity hemorrhage. Among 27 cases of spontaneous hepatic hemangioma rupture, 22 patients (95.7%) underwent surgery [4].
A multidisciplinary team met to discuss this patient’s management. Our patient was offered various treatment options, including surgical intervention. The patient opted for conservative treatment and declined surgery.
Our patient continued to physically and emotionally struggle with the symptoms resulting from the giant hemangioma, leading her to again seek medical management. Another multidisciplinary team convened to discuss viable treatments, which were then offered to the patient. This time, she decided to pursue a more conservative interventional radiology procedure.
She underwent liquid embolization with lipiodol and bleomycin. Though the hemangioma is largely the same size as prior to embolization, measuring approximately 10.3 x 7.3 cm, our patient endorsed resolution of early satiety, abdominal discomfort, and dyspnea on exertion back to baseline. This clinical response highlights that symptomatic relief may not correlate directly with changes in tumor size, particularly when mass effect rather than total lesion volume is the primary driver of symptoms. Embolization may reduce internal vascularity and pressure within the lesion, alleviating local compression of adjacent structures even without a substantial decrease in overall dimensions, for instance. As demonstrated in this case, meaningful improvement in quality of life can therefore be achieved through targeted intervention despite radiologic stability, emphasizing the importance of individualized assessment of symptom burden when considering treatment success.
This is an unusual case of a patient presenting with hepatic hemangioma and CEP, and it is especially rare to see large hepatic hemangiomas that continue to enlarge in the geriatric population. Although chronic eosinophilic disease and vascular malformations may coexist, current evidence does not support a mechanistic association between hepatic hemangiomas and chronic eosinophilic pneumonia or other eosinophilic inflammatory states. Hepatic hemangiomas are frequently encountered as incidental findings during the evaluation of unrelated conditions, reflecting their high prevalence rather than a shared pathological process. Their presence alongside complex diseases can inadvertently lead clinicians to pursue a unifying diagnosis despite the likelihood of independent processes. Recognizing HHs as common incidentalomas is therefore critical in preventing diagnostic overreach and ensuring that clinical decision-making remains grounded in evidence-based assessment rather than coincidental coexistence of findings.
Conclusions
Ockham’s razor, which states numquam ponenda est pluralitas sine necessitate (plurality must never be posited without necessity), has been a valuable teaching tool used by healthcare providers to make a unifying diagnosis, but it cannot be applied to every situation. Currently, there is no connection between CEP and hepatic hemangiomas.
However, with further testing, such as a liver biopsy and RNA sequencing, a link may surface. In the meantime, open communication, respecting patients’ decisions, providing emotional support, as well as utilizing a multidisciplinary approach are essential to provide individualized, quality care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Enormous haemangioma of the liver BMJ Case Rep Zerpa R Abdelghani EH Iliescu G Escalante C 012201910.1136/bcr-2018-226983 PMC 645330630936329 · doi ↗ · pubmed ↗
- 2A case report of giant hepatic hemangioma spontaneous regression in adult, non-cirrhotic patient and literature review Integr Cancer Sci Therap Andrea S Valerio DP Luca GG 82021
- 3Hepatic hemangioma -review- J Med Life Bajenaru N Balaban V Săvulescu F Campeanu I Patrascu T 41182015 https://pmc.ncbi.nlm.nih.gov/articles/PMC 4564031/26361504 PMC 4564031 · pubmed ↗
- 4Hepatic haemangiomas: Possible association with female sex hormones Gut Glinkova V Shevah O Boaz M Levine A Shirin H 135213555320041530659910.1136/gut.2003.038646 PMC 1774167 · doi ↗ · pubmed ↗
- 5A case report on enormous haemangioma of liver Ann Med Surg (Lond) Baral P Singh Bhandari R Pradhan S Maharjan N Mainali P Regmi D Kandel K 578257848520233791567110.1097/MS 9.0000000000001360 PMC 10617932 · doi ↗ · pubmed ↗
- 6Chronic eosinophilic pneumonia: A review South Med J Alam M Burki NK 495310020071726952510.1097/01.smj.0000242863.17778.1d · doi ↗ · pubmed ↗
- 7Chronic eosinophilic pneumonia: imaging findings [Article in Portuguese] Rev Fac Cien Med Univ Nac Cordoba Nuñez MM Castro HM Seehaus A 88907920223531224910.31053/1853.0605.v 79.n 1.33668 PMC 9004310 · doi ↗ · pubmed ↗
- 8Predictive factors for relapse in corticosteroid-treated patients with chronic eosinophilic pneumonia J Thorac Dis Takeuchi N Arai T Sasaki Y 435243601420223652408710.21037/jtd-22-511PMC 9745510 · doi ↗ · pubmed ↗