Prophylactic effect of omega-3 polyunsaturated fatty acids monotherapy in preventing recurrent major depressive disorder: A randomized controlled trial
Ikbal Andrian Malau, Cheng-Ho Chang, Wei-Jen Chen, Wen-Chun Liu, Halliru Zailani, Hsien-Feng Liao, Jane Pei-Chen Chang, Wei-Che Chiu, Kuan-Pin Su

TL;DR
This study found that omega-3 fatty acids as a standalone treatment may help prevent the recurrence of major depressive disorder.
Contribution
The study is the first to show the prophylactic effect of omega-3 monotherapy in preventing MDD recurrence.
Findings
Omega-3 monotherapy reduced MDD recurrence compared to placebo at 6 months.
Kaplan-Meier analysis confirmed omega-3's superiority in preventing MDD recurrence.
EPA levels were significantly higher in the omega-3 group, but not DHA.
Abstract
Omega-3 polyunsaturated fatty acids (n-3 PUFAs) have demonstrated efficacy as adjunctive treatment for MDD. In fact, fewer studies assessed the prophylactic properties of n-3 PUFAs as monotherapy on the recurrence of MDD. This study aimed to assess the prophylactic effect of n-3 PUFAs monotherapy against recurrent MDD. We conducted a 6-month randomized controlled trial to assess the prophylactic effect of n-3 in preventing recurrent MDD. We assigned 60 remitted MDD patients to the n-3 group (n = 30) and placebo (n = 30). Furthermore, we assessed the difference in depression severity and MDD recurrence based on the 21-item Hamilton Rating Scale for Depression (HRSD) at months 1, 2, 3, 4, and 6 between groups. The recurrent event of MDD was defined as an HRSD score >20. Furthermore, biochemical parameters in plasma were assessed as the secondary outcomes. There was no significant…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
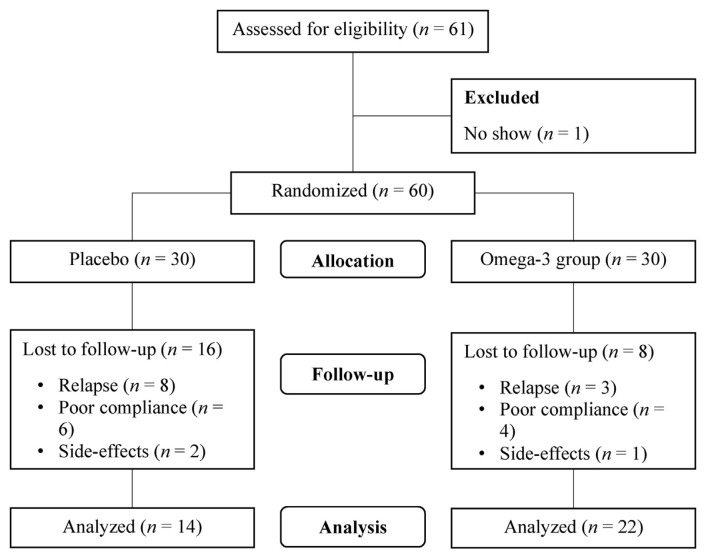 Figure 1
Figure 1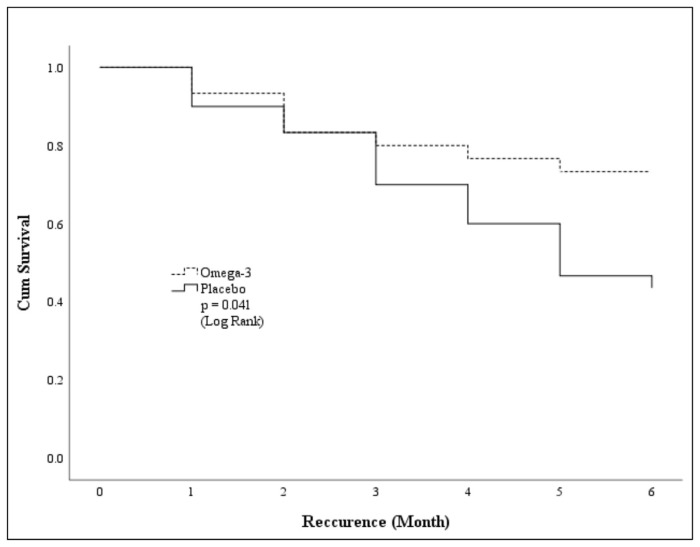 Figure 2
Figure 2- —Ministry of Science and Technology, Taiwan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFatty Acid Research and Health · Diet and metabolism studies · Treatment of Major Depression
Introduction
Major depressive disorder (MDD) is one of the leading causes of disability worldwide compared to other mental disorders [1] and is associated with multiple detrimental outcomes [2,3]. Persons with a history of MDD are at risk of experiencing a higher level of recurrence [4]. Moreover, MDD is challenging as the standard treatments often result in treatment-resistant depression followed by mild to severe adverse effects [5]. Given these complexities, omega-3 polyunsaturated fatty acids (n-3 PUFAs) are considered a potential alternative treatment for various psychiatric disorders [6–8]. Additionally, n-3 PUFAs have been studied for their potential benefits in managing MDD [9–11]. Hence, clinical evidence reveals a correlation between lower plasma n-3 PUFAs levels and an increased risk of depression [12]. N-3 PUFAs supplementation elevated plasma levels in MDD patients with higher baseline n-3 PUFA levels, leading to remission. Conversely, patients with lower baseline n-3 PUFA levels showed non-significant plasma level increases and ongoing depressive symptoms [13]. Therefore, the necessary dose and treatment duration might vary based on the individual’s baseline omega-3 fatty acid levels.
As an essential nutrient, n-3 PUFAs cannot be synthesized in the human body; therefore, it is crucial to emphasize the importance of n-3 PUFA-enriched diet and supplementation [14,15]. A prior network meta-analysis of ten clinical studies published in 2020 demonstrated that high-dose (≥2 g) n-3 PUFAs supplementation was associated with greater reductions in mood scores compared to low-dose (<2 g) [16] and well tolerated [17]. Highly concentrated EPA and DHA are the main components in n-3 PUFAs that have shown beneficial effect in mood disorders [18]. Particularly, supplementation with EPA-predominant n-3 PUFAs formulation is found to possess stronger potential for anti-inflammatory effects in depression [19]. The recommended ratio of eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) (>2:1) is considered effective in promoting antidepressant effect on MDD [20]. Therefore, supplementing n-3 PUFAs in dietary intake must be in accordance with the ratio of higher EPA than DHA for people with depression to reach the beneficial effects [20]. Nevertheless, it’s important to highlight that the precise effective dose of n-3 PUFAs for treating MDD remains unclear due to the mixed findings [19].
Several clinical trials were conducted to evaluate the therapeutic efficacy of n-3 PUFAs in MDD. However, the majority of studies have explored the adjuvant use of n-3 PUFAs in combination with antidepressants that contributed to lower mood scores [21,22]. Conversely, there are only a few studies considered n-3 PUFAs as monotherapy to treat MDD. Two studies highlighted the efficacy of DHA monotherapy [23,24], while another study reported beneficial effects of EPA monotherapy [25] in improving depressive symptoms among MDD patients. In addition, there is a study published in 2020 provided insight that EPA-predominant n-3 PUFAs monotherapy contributed to lowered mood scores in patients with cardiovascular diseases (CVD) comorbid MDD [26]. However, there has been no study evaluating the prophylactic effect of EPA-predominant n-3 PUFAs as monotherapy on MDD recurrence in remitted patients. Furthermore, this multi-site randomized controlled trial (RCT) aimed to fill this research gap by examining the potential of n-3 PUFAs monotherapy in preventing the recurrence of MDD, independent of antidepressant medications in remitted MDD patients. By investigating the prophylactic effects of n-3 PUFAs monotherapy, this study will provide significant insights into the role of nutritional interventions in maintaining remission and preventing the recurrence of depressive episodes in persons with a history of MDD.
Methods
2.1. Subjects and study design
We conducted a 6-month multi-center randomized controlled trial to assess the effectiveness of n-3 PUFAs monotherapy in preventing the recurrence of MDD. We recruited eligible participants from three outpatient psychiatry departments from different hospitals (China Medical University Hospital and Taipei Cathay Hospital) and the study adhered to the ethical principles laid out in the 1964 Declaration of Helsinki and its subsequent amendments.
The inclusion criteria for the study were: participants aged 18–65 years who had met the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) diagnosis of major depressive disorder in the past year and were currently in full remission, having two or fewer depressive symptoms in the last eight weeks, and a 21-item Hamilton Rating Scale for Depression (HRSD) score of less than 7 (non-depressive symptom) at the baseline. In addition, we ensured that the depression levels of all participants at baseline were classified as mild or less by using the Beck Depression Inventory (BDI) questionnaire, which was not greater than 18. The HRSD is a clinician-administered scale that objectively evaluates the severity of depression, focusing on somatic and physical symptoms. In contrast, the BDI is a self-reported questionnaire that captures patients’ subjective experiences, emphasizing emotional and cognitive aspects of depression. Using both scales provides a well-rounded assessment by integrating objective clinical observations with the patient’s personal perspective. All participants in this study did not receive antidepressants or psychosocial therapies during the study and were required to have a full understanding of the entire research plan before signing an informed consent. Participants who were diagnosed with schizophrenia, bipolar disorder, psychotic disorder, organic mental disorder, substance use disorder, acute psychotic state or strong suicidal intention, and allergy to fish oils were excluded from the study. Institutional review board (IRB) approvals were obtained from China Medical University Hospital (DMR93-IRB-87) and Taipei Cathay Hospital (CT9336). This trial was registered on the ClinicalTrials.gov with identifier: NCT00816322.
2.2. Randomization
Sixty eligible patients were included and randomly assigned to n-3 group and placebo, in a 1:1 ratio using computer-generated randomization with block randomization. An independent researcher performed the randomization, and the allocation sequence remained unknown to the research team until the databases were finalized.
2.3. Interventions
Intervention was given to n-3 group with a fish oil capsule of EPA and DHA (EPA 2.1 g, DHA 1.1 g) and the source of n-3 fatty acids is menhaden fish, while placebo group was provided with a high oleic oil capsule. Each subject in both groups consumed 4 capsules per day. The placebo group was administered an equal number of placebo capsules as the n-3 group for 6 months, and the physical characteristics such as appearance and weight of each capsule will be indistinguishable between the two groups. To minimize any potential bias, both the fish oil and placebo capsules were packaged to be odorless and had a similar flavor. This ensured masking participants from intervention. The cessation of treatment in the study was prompted by several reasons including recurrence, intention or risk of suicide (HRSD-21 suicide item score ≧3), condition requiring hospitalization, subjective decision to discontinue treatment, and discontinuation of treatment due to side effects. In the n-3 group, eight patients decided to discontinue the study, with three experienced MDD relapse with unstable emotion and prescribed with medication, four had poor compliance with irregular visit and did not show up, and one patient requested to stop due to mild side-effects such as unable to swallow the capsules. On the other hand, sixteen patients in the placebo group discontinued the study, of whom eight experienced MDD relapse and were prescribed with medication, six had poor compliance with irregular visit and did not show up, and two requested to stop due to mild side-effects such as an allergy and unable to swallow the capsules. The details of the subjects’ recruitment, allocation, and analysis are presented in Fig. 1.
2.4. Clinical assessment
This study used the 21-item HRSD scale as a reliable diagnostic tool to measure depression levels. The clinical team conducted interviews with participants using a semi-structured questionnaire and calculated the total score of the 21-item HRSD scale to assess the level of depression in all participants at month 1, 2, 3, 4, 5, and 6. Thus, further analysis of the incidence of depressive symptoms was assessed both in the n-3 group and placebo at each time point. Recurrent events of MDD were evaluated using an HRSD score greater than 20. Trained clinical nurses were masked and assigned for the clinical assessment.
2.5. Biochemical parameters
As part of the study, venous blood samples were collected for biochemical parameters analysis. Gas chromatography, a powerful and precise technique, was used to analyze the relative amounts fatty of acids in blood samples. The fatty acid compositions of the patients were analyzed using gas chromatography with fatty acid methyl esters (FAMEs). By comparing the retention times of the unidentified fatty acids with suitable standard FAME, their compositions were determined. Fatty acid levels were assessed using red blood cells (RBCs) because they can reflect long-term fatty acid status. The process involves isolating RBCs, extracting lipids, converting fatty acids to FAMEs through transesterification, and analyzing them using gas chromatography. Gas chromatography separates and quantifies fatty acids with results interpreted using reference standards. The protocol with detailed scheme was explained in previous study [27]. Subsequently, we compared erythrocyte fatty acid levels between two arm groups at baseline and endpoint (month 6) of study. This study also assessed the changes in major biochemical parameters related to the side effects of intervention on liver, kidneys, hearts, blood clotting, blood glucose. Thus, we assessed the levels of aspartate aminotransferase (AST/GOT), alanine aminotransferase (ALT/GPT), blood urea nitrogen (BUN), creatinine, cholesterol, triglycerides, low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol, prothrombin time (PT), activated partial thromboplastin time (aPTT), glucose, and prolactin. The biochemical parameters were assessed using standardized methods. AST, ALT, BUN, creatinine, cholesterol, triglycerides, LDL, HDL, and glucose were measured using enzymatic or colorimetric assays on automated biochemistry analyzers (e.g., Roche Cobas). PT and aPTT were evaluated through coagulation assays on coagulation analyzers (e.g., Sysmex CA-series). Prolactin levels were determined using ELISA. Serum samples were used for most parameters, while plasma was used for PT and aPTT. All subject data were kept confidential, and the examiner remained blinded to ensure intervention accuracy.
2.6. Sample size estimation
In this study, we expected that the intervention would lead to a decrease of 2 points in the HRSD (Hamilton Rating Scale for Depression) score. The population standard deviation is estimated to be 3 according to previous similar RCT study, indicating the variability of HRSD scores within the population. The study follows a balanced design with an equal number of participants assigned to both the control and intervention groups. The objective is to compare the mean HRSD scores between the two groups to evaluate the impact of the intervention on depression levels. To estimate the sample size, we assumed α = 0.05 and power = 0.80 (β = 0.20, therefore 1-β = 0.8). Initially, the number of patients in each group was set to 16, but to account for potential dropouts, we increased the sample size to 30 in each group.
Where n is sample size in each group, μ1-μ**2 is population mean in treatment group-population mean in placebo, σ*^2^* is population variance (SD), a is conventional multiplier for alpha* when alpha is 0.05, and b is conventional multiplier for power* when beta is 0.80.
2.7. Statistical analysis
We performed all statistical analysis using SPSS v.26 software (SPSS Inc., Chicago, IL, USA). The HRSD assessments before and after treatment were collected. The difference in characteristics and severity of depression at baseline and the HRSD scores at each month assessments between groups were compared by Mann–Whitney U-test. Chi-squared (χ2) test was used to compare the frequency of recurrences between two groups. Kaplan–Meier Survival analysis was used to evaluate survival function, and log-rank test to compare the difference survival rate in recurrence of MDD between two groups as the primary outcomes. We analyzed the comparison of erythrocyte PUFAs levels and other biochemical parameters between two groups at baseline and month 6 (endpoint) as the secondary outcomes using Mann–Whitney U-test. The significance of the difference was set at p-value< 0.05.
Results
3.1. Characteristics of participants at baseline
This study ensured that there were no differences in characteristics of subjects between placebo and the n-3 group at baseline. Table 1 shows from 60 subjects that assigned to two groups, there were no differences in age ( p-value = 0.765) and sex ratio ( *p-*value = 0.994) at baseline. Moreover, depression severity that assessed using both HRSD and BDI did not differ between the n-3 group and placebo group ( p-value> 0.05).
3.2. Comparison of HRSD scores between two groups at each time point
Table 2a shows that there is no significant difference in the HRSD mean score between groups at each time point of the study period ( p-value> 0.05). However, HRSD mean score was lower in the n-3 group than in placebo group at each time. Table 2b shows MDD patients in the n-3 group had a lower recurrence rate compared to the placebo group at month 6 ( p-value = 0.035).
Moreover, the 6-month survival rate of remitted MDD patients was higher in the n-3 group and statistically significant difference between groups ( p-value = 0.041) as shown in Fig. 2.
3.3. Comparison of erythrocyte PUFAs levels and other biochemical parameters between two groups at baseline and month 6 (endpoint)
Table 3 summarizes the changes in biochemical parameters at baseline and endpoint of intervention between groups. There were no significant differences of biochemical parameters such AST/GOT, ALT/GPT, BUN, creatinine, cholesterol, triglycerides, LDL, HDL, PT, aPTT, glucose, and prolactin between groups both at baseline and endpoint ( p-value> 0.05). In a comparison of AA, EPA, and DHA levels, there was no significant difference in AA level between the n-3 group and the placebo group at month 6 ( p-value = 0.141), but the EPA of the n-3 group after treatment was significantly higher than that of the control group ( *p-*value = 0.023), and the DHA in the n-3 group after treatment tended to be higher than those in the placebo but did not reach a significant difference ( *p-*value = 0.119).
Discussion
4.1. Main findings
To the best of our knowledge, this is the first study assessing the prophylactic effect of n-3 PUFAs monotherapy in preventing the recurrent events in remitted MDD patients for 6 months follow up. The results highlighted the potential of n-3 PUFAs monotherapy as a prophylactic treatment option for individuals with a history of MDD. The primary results of this study revealed a significant reduction in the recurrence of depressive episodes among participants receiving EPA-predominant n-3 PUFAs monotherapy with better survival rate at month 6 compared to the placebo. EPA-predominant n-3 PUFAs supplementation has been extensively studied and is believed to contribute to therapeutic effects in MDD [19,28]. Therefore, EPA-predominant n-3 PUFAs might protect against recurrent depressive episodes and mitigate inflammation-induced mood dysregulation by addressing inflammation, a recognized factor in the development of depression [29]. In addition, the beneficial effects of n-3 PUFAs, specifically DHA, may also contribute to its prophylactic properties, as it has been shown to support neuronal function and promote synaptic plasticity [30] that could affect the improvement of depressive symptoms. To explore the potential antidepressant-like effects of n-3 PUFAs, examining specific biomarkers associated with depression progression could provide valuable molecular insights. For instance, biomarkers such as S100β, high mobility group box 1 (HMGB1), and NSE can be analyzed in human tissues, particularly plasma. N-3 PUFAs may modulate the release of these DAMPs by interfering with their binding to their receptors such as toll-like receptors (TLRs) and receptor for advanced glycation end product (RAGE), thereby mitigating the activation of inflammatory responses linked to depression [31]. Even though this study’s findings presented that monthly HRSD scores did not show any significant differences at each time point (month) between groups. However, HRSD scores were lower in the n-3 group compared to the placebo group in each month. It is plausible that the observed trend could be attributed to the limited size of the sample, which may have hindered the attainment of statistically significant outcomes.
4.2. Secondary outcomes
Secondary outcomes showed the biochemical parameters related to side effects of n-3 PUFAs monotherapy on function of organs such as liver, kidney, heart. Our study demonstrated that no significant adverse effects were caused. The use of n-3 PUFAs supplementation has been confirmed for its efficacy [16,32] and safety without adverse effects in treating depressive symptoms [33]. Furthermore, our study revealed increased plasma levels of EPA and DHA, with only EPA demonstrating statistical significance. However, this indicates that n-3 PUFAs monotherapy induced changes in erythrocyte PUFAs composition. The lack of significant changes in DHA levels may be attributed to its distinct metabolic role, compared to EPA. While EPA is rapidly utilized in anti-inflammatory processes and mood regulation, DHA primarily supports neuronal membrane structure, which may result in slower turnover [34]. Additionally, adequate baseline DHA levels could lead to a plateau effect with supplementation. These findings suggest that EPA may have a more immediate impact on mood, while DHA plays a complementary, long-term role. Future studies should investigate the delayed effects of DHA on neural health and its interactions with EPA in mood stabilization. Likewise, previous study found that 12-week n-3 PUFAs supplementation significantly contributed higher level of EPA in plasma but not with DHA [35]. On the other hand, clinical studies also reported that 8-week and 12-week n-3 PUFAs supplementation contributed to higher levels of both EPA and DHA in plasma [36]. These various findings might be affected by different lengths of intervention and different doses of n-3 PUFAs. Nevertheless, previous meta-analytic studies have emphasized that EPA has more beneficial effect on treating depression compared to DHA [19]. Overall, our study supported the idea that EPA-predominant n-3 PUFAs have a beneficial effect in preventing the risk of recurrent depressive episodes without any significant adverse effects. This study demonstrated that a 3-g dose of n-3 PUFAs could be deemed tolerable and effective in preventing MDD recurrence. This aligns with a previous meta-analysis study recommending a ≥2 g dose of n-3 PUFAs to reach beneficial reductions in mood scores [16]. Our study has several strengths. First, it employed a randomized controlled trial design with a 6-month intervention. Second, by focusing solely on n-3 PUFAs monotherapy, the study provides valuable insights into the monotherapy effects of n-3 PUFAs in preventing MDD recurrence. The clear research objective adds to the strength of the study, allowing for a focus on prophylactic effect of n-3 PUFAs. We acknowledge several limitations in our study. Primarily, dietary intake, specifically the incorporation of n-3 food resources, may have influenced the observed outcomes as well as the effects of medication history. Thus, future studies should take these relevant factors into account.
Moreover, side-effects related factors including emotional instability, cognitive impairments, behavioral changes, worsening of symptoms, psychosocial distress, or relapse due to inadequate treatment, placebo effects, or trial-related stress should be considered in the future study. While the role of circulating PUFAs and their metabolites was not explored in this work, we acknowledge their potential importance in modulating neural and behavioral responses. Future studies are warranted to investigate the relationship between PUFA-related metabolites, targeted neural parameters, and MDD to provide a more comprehensive understanding of the underlying mechanisms. For example, eicosanoids and resolvins, which play roles in inflammation and cell signaling in depression [37,38]. Furthermore, the study’s findings should be interpreted with caution due to the relatively modest sample size, notwithstanding attempts to address this limitation through the recruitment of participants from multiple centers. A key limitation of this study is the high attrition rate, which may have introduced bias by creating imbalances between the groups and reducing the generalizability of the findings. Despite efforts to address missing data, the potential for systematic differences between those who completed the study and those who dropped out could have impacted the reliability of the results.
Another limitation of this study is the lack of initial assessment of co-morbid physical diseases, which could influence the results. However, the study focused on the primary variables under investigation, and future research should incorporate these factors to control for potential confounders and improve generalizability. While a longer follow-up would be ideal to fully evaluate the long-term effects of n-3 PUFAs, the six-month period was selected to capture the initial and potentially significant impact of treatment on depression-related outcomes. Future studies with extended follow-up durations are needed to assess the long-term prophylactic effects, especially for relapsing conditions like MDD. Finally, the HRSD was employed not for diagnostic purposes but rather for assessing the severity of MDD.
4.3. Conclusion
In conclusion, the findings of this study provide evidence supporting the use of n-3 PUFAs, particularly EPA-predominant monotherapy, as a prophylactic measure against the recurrence of MDD and contributed to a better survival rate at month 6 of intervention. Incorporating n-3 PUFAs into the treatment regimen for individuals with a history of MDD could offer a promising approach to long-term management and prevention. Further study is warranted to elucidate the underlying mechanisms and optimize the use of n-3 PUFAs as a prophylactic intervention in preventing recurrence of MDD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD 2019 Mental Disorders Collaborators Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet Psychiatry 2022 9 137 50 10.1016/s 2215-0366(21)00395-3 35026139 PMC 8776563 · doi ↗ · pubmed ↗
- 2Zhang X Zhou Y Sun J Yang R Chen J Cheng X A cohort study of adolescents with depression in China: tracking multidimensional outcomes and early biomarkers for intervention Gen Psychiatry 2022 35 e 100782 10.1136/gpsych-2022-100782 PMC 942279436118419 · doi ↗ · pubmed ↗
- 3Yan G Zhang Y Wang S Yan Y Liu M Tian M Global, regional, and national temporal trend in burden of major depressive disorder from 1990 to 2019: an analysis of the global burden of disease study Psychiatry Res 2024 337 115958 10.1016/j.psychres.2024.115958 38772160 · doi ↗ · pubmed ↗
- 4Malhi GS Mann JJ Depression Lancet 2018 392 2299 312 10.1016/s 0140-6736(18)31948-2 30396512 · doi ↗ · pubmed ↗
- 5Howes OD Thase ME Pillinger T Treatment resistance in psychiatry: state of the art and new directions Mol Psychiatry 2022 27 58 72 10.1038/s 41380-021-01200-3 34257409 PMC 8960394 · doi ↗ · pubmed ↗
- 6Chang JP Su KP Nutritional neuroscience as mainstream of psychiatry: the evidence-based treatment guidelines for using omega-3 fatty acids as a new treatment for psychiatric disorders in children and adolescents Clin Psychopharmacol Neurosci 2020 18 469 83 10.9758/cpn.2020.18.4.469 33124582 PMC 7609218 · doi ↗ · pubmed ↗
- 7Nishi D Su KP Usuda K Pei-Chen Chang J Chiang YJ Chen HT The efficacy of omega-3 fatty acids for depressive symptoms among pregnant women in Japan and Taiwan: a randomized, double-blind, placebo-controlled trial (SYNCHRO; NCT 01948596) Psychother Psychosom 2019 88 122 4 10.1159/000495296 30540990 · doi ↗ · pubmed ↗
- 8Su KP Tseng PT Lin PY Okubo R Chen TY Chen YW Association of use of omega-3 polyunsaturated fatty acids with changes in severity of anxiety symptoms: a systematic review and meta-analysis JAMA Netw Open 2018 1 e 182327 10.1001/jamanetworkopen.2018.2327 30646157 PMC 6324500 · doi ↗ · pubmed ↗