Weight loss and self-perceived quality of life following laparoscopic Roux-en-Y gastric bypass: is it important?
Gustavo Rodrigues Alves CASTRO, Laís Ducatti MACEDO, João Victor Vecchi FERRI, Isabella Benitez VULCANIS, Diancarlos Pereira de ANDRADE, José Alfredo SADOWSKI, Eduardo Lemos de Souza BASTOS, João Caetano Dallegrave MARCHESINI

TL;DR
This study shows that laparoscopic Roux-en-Y gastric bypass surgery improves quality of life, with greater weight loss and longer time post-surgery linked to better physical and emotional well-being.
Contribution
The study demonstrates a direct relationship between weight loss after LRYGB and long-term improvements in self-perceived quality of life, including both physical and emotional domains.
Findings
Greater weight loss is associated with significant improvements in general health and mental health domains of quality of life.
Older patients and those with longer post-surgery follow-up show better emotional and mental health outcomes.
Even nonsignificant weight loss can improve quality of life in physiological, psychological, and social aspects.
Abstract
Weight loss (WL) is the most commonly used datum to measure the results of metabolic and bariatric surgery. The amount of WL is generally directly and proportionally associated with the improvement in quality of life (QoL), as the greater the former, the greater the perception of well-being. To assess the relationship between the amount of weight lost after laparoscopic Roux-en-Y gastric bypass (LRYGB) and self-perceived improvement in quality of life (QoL). The medical records of patients who underwent LRYGB between January 2017 and December 2019 with a minimum follow-up of 3 years were analyzed. The data obtained in the subgroups made up according to percentage of total weight loss (%TWL), age, and time elapsed since surgery were compared with the self-perceived QoL by the Short Form Survey 36 (SF-36) questionnaire. A total of 95 individuals (71.6% women) with an average age of 45…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
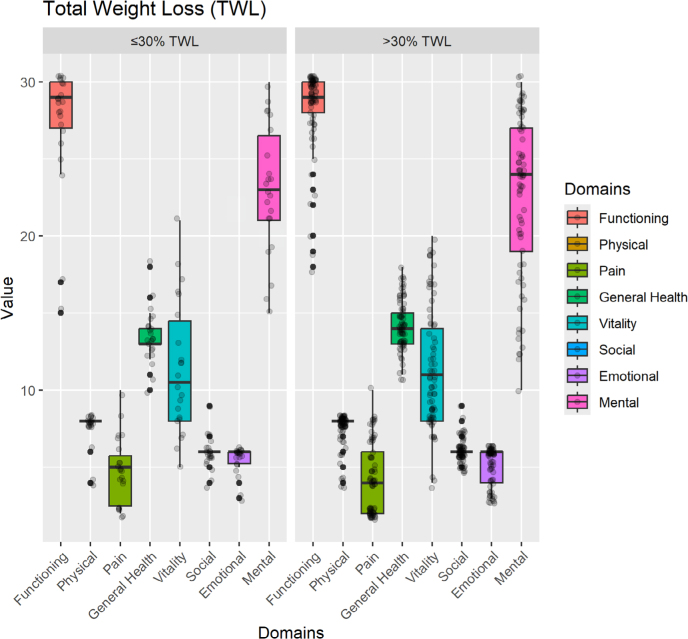 Figure 1
Figure 1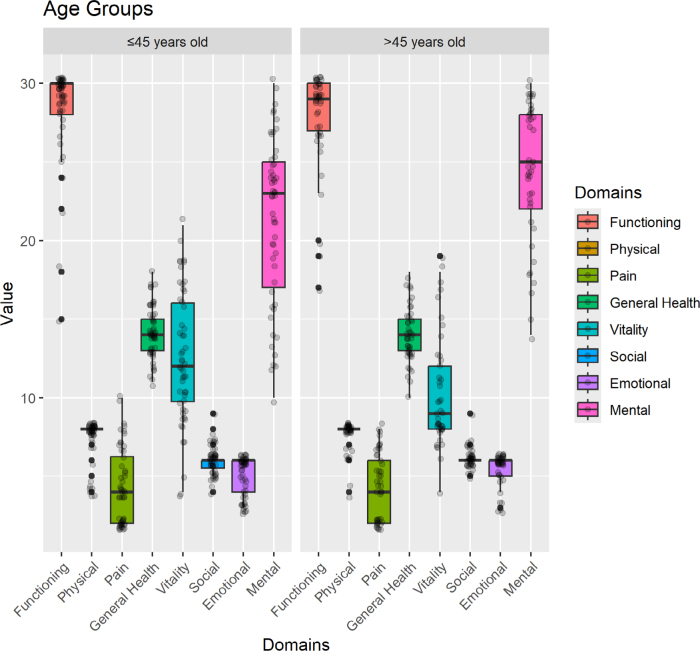 Figure 2
Figure 2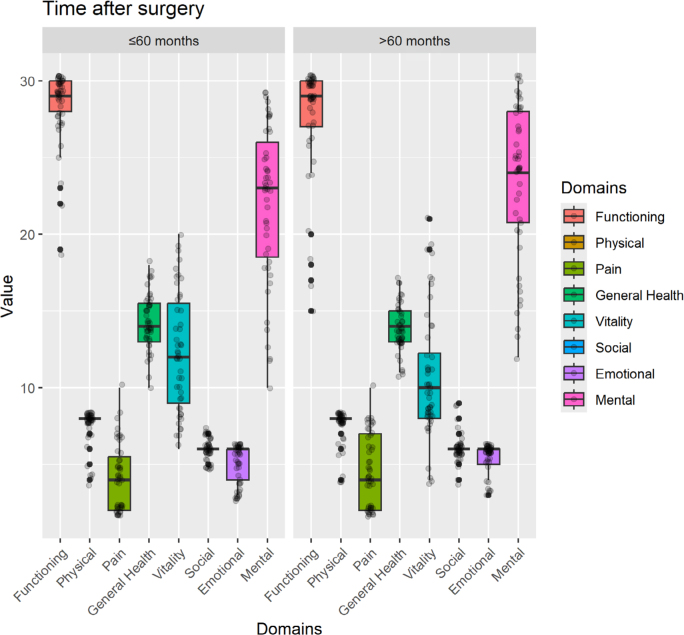 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Gastric Cancer Management and Outcomes · Enhanced Recovery After Surgery
INTRODUCTION
Weight loss (WL) is the most commonly used datum to measure the results of metabolic and bariatric surgery (MBS). According to the Position Statement of the Brazilian Society of Bariatric and Metabolic Surgery (SBCBM), at least 20% total WL must be achieved to be considered successful^ 2 ^, but a universally accepted consensus is still uncertain. Conversely, other parameters can also measure the outcome of a bariatric procedure such as quality of life (QoL) and improvement or remission of comorbidities^ 1,4,12 ^.
QoL is not very easy to accurately measure, as it is based on the patient’s subjective perception of the overall quality of their life after the bariatric procedure^ 1 ^. Even so, some tools have already been validated in the literature and are frequently used for this purpose^ 6,18 ^. One of them is the Short Form Survey 36 (SF-36) questionnaire, a widely-used and validated assessment method for both surgical and clinical conditions, providing important data on topics related to QoL^ 7,14 ^. It consists of eight domains, evaluating physical and mental aspects, being useful in comparing general and specific populations. Additionally, it can estimate the relative burden of different diseases and highlight the health benefits produced by a wide range of treatments^ 11,13 ^.
In the real world, the amount of WL is generally directly and proportionally associated with improvements in QoL, as the greater the former, the greater the perception of well-being^ 8 ^. However, improvements in QoL may also not be linearly related to the amount of weight lost, as nonsignificant reductions in body weight may already be sufficient to increase QoL in physiological, psychological, social, and economic aspects. Furthermore, QoL seems to be one of the main targets of patients seeking bariatric procedures, which is not always properly valued by doctors.
Therefore, in the present study, we aim to evaluate the QoL of patients undergoing laparoscopic Roux-en-Y gastric bypass to assess whether there is any linear relationship between the percentage of total weight loss (%TWL) and improvements in QoL.
METHODS
Study design
This is a retrospective study, with a quantitative approach carried out through document analysis and questionnaire application.
Study population
All patients who underwent MBS in a single center of excellence between January 2017 and December 2019 were considered eligible for the study. Inclusion criteria encompassed being over 18 years old, having undergone LRYGB surgery, and at least 3 years of follow-up. Exclusion criteria were applied to patients who underwent revisional LRYGB and patients who did not agree to answer the QoL assessment questionnaire, or did not fill it out correctly or completely.
Data collection
The study was approved by the Research Ethics Committee of our Institution (number 6029928) and consisted of two stages. First, demographic data — such as age, sex, date of surgery, type of procedure, preoperative weight, weight at the last postoperative (PO) consultation, preoperative body mass index (BMI), and BMI at the last PO consultation — were retrieved from medical records. In the second stage, patients who met the inclusion criteria were contacted via telephone and invited to participate in the study. Two phone call attempts were considered before excluding non-responding patients. For those who have been successfully contacted and agreed to take part in the study, the SF-36 Medical Outcomes Study questionnaire was electronically sent along with the Informed Consent Form. Patients were asked to send back, also electronically, the QoL assessment instrument and the signed Consent Form within two weeks.
Subgroups analyzed
Based on preoperative weight and the weight at the last PO consultation, the percentage of total weight loss (%TWL) was calculated using Equation 1:
[Preoperative weight – Current weight / Preoperative weight] x 100(1)
Subsequently, patients were divided into two groups according to %TWL at ≤30% and >30%. Furthermore, for comparative analysis with QoL, patients were divided according to age (≤45 and >45 years) and time elapsed since surgery (≤60 and >60 months).
QoL assessment questionnaire
The questionnaire used for the analysis was the Short Form Survey 36 (SF-36), a generic health survey consisting of 36 questions used to measure self-reported QoL. It assesses various domains of physical and mental health and provides summary scores for physical and mental components. It is necessary to observe the relevant domains of the questionnaire and the score belonging to each of them individually, that is, a total of 8 domains, with 36 questions. Therefore, the proportion of scores is standardized, making the comparison between dimensions feasible^ 11,13 ^.
The domains covered are: D1 (Physical Functioning); D2 (Role Limitations due to Physical Aspects, or Role Physical); D3 (Pain); D4 (General Health); D5 (Vitality); D6 (Social Function); D7 (Role Limitations due to Emotional Problems, or Role Emotional); and D8 (Mental Health). The values of each domain are scored from 0 (zero) to 100 (one hundred), from worst to best. Individuals who agreed to participate received an anonymous link to respond to the questionnaire electronically.
Primary end point
Assessment of the self-perceived QoL obtained through the application of the SF-36 according to %TWL with at least 3 years of follow-up.
Secondary end point
Comparison of the self-perceived QoL obtained through the application of the SF-36 with age and time elapsed since surgery.
Statistical analysis
The R program version 4.1.2 was used in all analyses. The descriptive analysis was carried out by checking quantities and percentages for categorical variables and descriptive measures (minimum, maximum, quartiles, mean, and standard deviation) for continuous variables. The Student’s t-test was used to compare the means of the variables on the Likert scale between two independent groups. If the calculated p-value is greater than the critical t-value for a given level of significance (p<0.05), the conclusion is that there is a significant difference between the means of the two samples.
RESULTS
Study population
Between January 2017 and December 2019, 536 patients with obesity underwent MBS at the study Hospital. Of these, 441 (82.2%) did not meet the inclusion criteria, were unreachable, refused to participate in the study, or did not adequately complete the QoL assessment instrument. Therefore, our final sample size comprised 95 (17.7%) patients undergoing primary LRYGB who adequately completed the QoL assessment instrument.
Demographic data
Of the 95 patients included in the study, 68 (71.6%) were women and the average age of the entire sample was 45 years (ranging from 22 to 74). The mean preoperative weight was 114 kg (74–193) and mean PO weight was 73.4 kg (47–158). According to BMI data, there were preoperative and PO means of 40.3 kg/m^2^ (32–58.9) and 25.9 kg/m^2^ (18.6–48.2), respectively.
The mean %TWL was 35.6%. Regarding time elapsed from surgery to the moment of application of the QoL assessment instrument, the average was 61.1 months (45–81 months).
Overall analysis
The best scored domain was D1 (Physical Functioning), with a maximum score of 90.7, followed by D2 (Role Physical) with 86.3, showing a greater functional capacity described by patients. Meanwhile, the minimum score was observed in the D3 domain (pain), with 23.58, highlighting it as a relevant negative factor following the procedure.
Assessment of QoL according to %TWL
As shown in Figure 1, individuals with %TWL greater than 30% reported better self-perception of their general health (D4 domain) (p<0.05). This finding allows us to infer that the greater the weight loss, the better the overall QoL after LRYGB surgery.
Comparative analysis of the eight quality of life domains according to the percentage of total weight loss.
Assessment of QoL according to age
We observed that the older group reported better scores in D7 (Role Emotional) and D8 (Mental Health) (p<0.05), showing a better performance than the younger group (Figure 2).
Comparison of qualify of life scores between age groups according to domains of the Short Form Survey 36 questionnaire.
Assessment of QoL according to PO period
According to the time elapsed since surgery, the sample was divided into a group with less than 60 months of follow-up and another with over 60 months of follow-up; the latter showed better results in D7 (Emotional Role; p<0.05), as shown in Figure 3.
Comparison of quality of life scores between groups according to the time elapsed since surgery.
DISCUSSION
In the present study, we verified that there may be a linear association between the amount of weight lost after LRYGB surgery and general self-perceived improvement in QoL. We also found that not only physical function improved, but also mental aspects, especially in the long term and in older patients.
In our study, the impact of WL after MBS on QoL was measured using the SF-36 questionnaire, which is composed of 36 items divided into eight domains^ 14 ^, used in various clinical settings to study the impact of chronic diseases on health-related QoL. Khawali et al.^ 7 ^ compared 41 patients with severe obesity on a waiting list for bariatric surgery with 84 patients undergoing MBS in a public health system. The group that had already undergone the procedure had higher scores in all domains of the SF-36 questionnaire than the preoperative group. Similarly, authors of a study encompassing 65 bariatric patients also used the SF-36 tool to assess QoL, and showed that QoL improved significantly after 1 year of MBS^ 12 ^.
In addition to the SF-36 questionnaire, there are other methods for assessing QoL in bariatric patients. The most popular is probably the Bariatric Analysis and Results Reporting System (BAROS) protocol^ 17 ^. Nonetheless, the BAROS protocol has body weight loss among its scores, namely percentage of excess weight loss (%EWL), making the dissociation of this variable from the others somewhat nebulous^ 16 ^.
Another tool that can also be used is the Moorehead-Ardelt Quality of Life Questionnaire II, which can be used independently or incorporated into the BAROS protocol^ 3,15,17 ^. This instrument assesses several pre- and PO comorbidities, such as hypertension, diabetes mellitus, peripheral vascular disease, dyslipidemia, sleep apnea, and infertility, as well as self-esteem, physical activities, social relationships, labor, and libido. However, it is not able to assess the QoL of patients with extreme obesity properly^ 12,15 ^.
In our study, physical, emotional and mental aspects were the best scored domains in the overall analysis, while pain was the worst. There are a wide variety of causes for pain after LRYGB surgery that may explain this lower score, including behavioral and nutritional disorders, functional motility disorders, marginal ulceration, and internal hernia. Although sometimes not clinically concerning, surgeons should be aware of this self-perception, as it may negatively impact QoL assessment.
Regarding the relationship between WL and self-assessment of QoL, our findings are as expected, considering that WL seems to be the main expectation of patients with obesity when undergoing bariatric procedures. Therefore, patients with greater WL tend to better evaluate their QoL, even minimizing some dysfunctions related to the nature of bariatric surgeries. We corroborate the findings of a systematic review whose authors evaluated the impact of WL on health-related QoL in overweight and obesity adults using the SF-36 and the Impact of Weight on Quality of Life-Lite (IWQOL-Lite) instruments. The authors provided evidence supporting that WL achieved by MBS can significantly improve QoL. Furthermore, sustained WL seems to be associated with maintenance of improvements in QoL, although these improvements were only significant for physical, rather than mental domains^ 10 ^.
As for the time elapsed since surgery, our study demonstrated a positive association with emotional aspects of the patients (D7 — Role Emotional), even in the long term after surgery. We corroborate other studies. Sierżantowicz et al.^ 19 ^ carried out a systematic review to analyze the health-related QoL changes in patients who underwent bariatric surgery with at least 9 years of follow-up. The authors observed that, despite the decrease in the QoL scores from the second year onwards, their values at 9–12 years were still significantly higher than at the baseline, showing that the positive effects of bariatric surgery on QoL can be sustained at the long term. The finding that the improvement in self-perceived QoL is more significant in the first years after bariatric surgery, but that it can also be sustained in the long term, is corroborated by another systematic review whose authors included 40 studies in a qualitative analysis. Interestingly, the researchers showed consistent results regardless of the instrument used to assess QoL^ 18 ^.
Furthermore, we demonstrated that older patients reported better scores in emotional and mental domains after the procedure, explained perhaps by maturity or differences between generations. Similarly, Gerber et al.^ 5 ^ found that older individuals (>60 years old), preoperatively, scored better on mental aspects than the entire cohort, and PO improvements in physical components and obesity problems were sustained in all age groups.
Undoubtedly, physical aspects seem to perform better than the psychological domains after MBS, whatever the QoL assessment tool. In a very long-term prospective cohort (12 years), patients undergoing gastric bypass significantly sustained their improvement in QoL in both weight domains of the IWQOL-Lite instrument and physical domains of the SF-36 instrument when compared with the non-surgical group, but this superiority was not sustained in terms of mental/psychological aspects^ 9 ^. Conversely, in our study, emotional and mental aspects actually improved, especially after 5 years of the procedure and in older patients. Perhaps our commitment to maintaining close psychological and, whenever necessary, psychiatric follow-up for all patients, regardless of mental illness diagnoses, may be the reason for this finding.
We are aware that our study has some limitations that could weaken the findings. First, we had significant missing data, despite our great efforts to contact enrolled patients and try to convince them to participate in the study. Unfortunately, many of them refused to fill out the questionnaire. Second, the cross-sectional design of the study has its inherent downsides preventing an evolutionary assessment. Third, we only included patients undergoing gastric bypass. Obviously, our findings cannot be applied to other types of bariatric procedures. Finally, the assessment of QoL by self-report is highly subjective and not always reliable, although questionnaire designs have already been validated.
Notwithstanding, according to our findings, we clearly verified positive impacts on the QoL of patients undergoing LRYGB surgery, mainly related to the physical and functional domains. Furthermore, we also showed interesting beneficial effects on mental and emotional aspects, sustained in the long term.
CONCLUSIONS
In the present study, we demonstrate that the amount of weight lost provided by LRYGB can have a direct relationship with significant positive impacts on health-related self-perceived QoL, both physical and emotional. Moreover, these effects appear to be sustained in the long term, especially in older individuals.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andrade MRV Vale ARSD Silva MSP Barros JHC Lagares LS Almeida LAB Skin color differences and health-related quality of life perception after gastric bypass Roux-en-Y: a cross-sectional study Arq Bras Cir Dig 202538 e 187210.1590/0102-6720202500003 e 187240052993 PMC 11883800 · doi ↗ · pubmed ↗
- 2Berti LV Campos J Ramos A Rossi M Szego T Cohen R Position of the SBCBM - nomenclature and definition of outcomes of bariatric and metabolic surgery Arq Bras Cir Dig 201528 Suppl. 1210.1590/S 0102-6720201500 S 10000226537262 PMC 4795295 · doi ↗ · pubmed ↗
- 3Castanha CR Tcbc-Pe ÁABF Castanha AR Belo GQMB Lacerda RMR Vilar L Evaluation of quality of life, weight loss and comorbidities of patients undergoing bariatric surgery Rev Col Bras Cir 2018453 e 186410.1590/0100-6991 e-2018186430020323 · doi ↗ · pubmed ↗
- 4Cooiman MI Aarts EO Janssen IMC Hazebroek EJ Berends FJ Weight loss, remission of comorbidities, and quality of life after bariatric surgery in young adult patients Obes Surg 20192961851710.1007/s 11695-019-03781-z 30790164 · doi ↗ · pubmed ↗
- 5Gerber P Gustafsson UO Anderin C Johansson F Thorell A Effect of age on quality of life after gastric bypass: data from the Scandinavian Obesity Surgery Registry Surg Obes Relat Dis 2022181113132210.1016/j.soard.2022.06.01735999164 · doi ↗ · pubmed ↗
- 6Khaitan M Gadani R Pokharel KN Gupta A Good to excellent Quality of Life in patients suffering from severe obesity post bariatric surgery - A single-center retrospective study report using BAROS Questionnaire J Minim Access Surg 2022182284810.4103/jmas.JMAS_268_2033885023 PMC 8973491 · doi ↗ · pubmed ↗
- 7Khawali C Ferraz MB Zanella MT Ferreira SR Evaluation of quality of life in severely obese patients after bariatric surgery carried out in the public healthcare system Arq Bras Endocrinol Metabol 201256133810.1590/s 0004-2730201200010000622460193 · doi ↗ · pubmed ↗
- 8Kolotkin RL Andersen JR A systematic review of reviews: exploring the relationship between obesity, weight loss and health-related quality of life Clin Obes 2017752738910.1111/cob.1220328695722 PMC 5600094 · doi ↗ · pubmed ↗