Clinical decisions in Orthodontics using x-ray-based images and artificial intelligence approaches: a scoping review
Pedro Henrique José de OLIVEIRA, João Roberto GONÇALVES, Luiz Gonzaga GANDINI, Julianna de Oliveira Lima PARIZOTTO, Michelle Sousa OLIVEIRA, Renata Mayumi KATO, Karine EVANGELISTA, Lucia Helena Soares CEVIDANES, Jonas BIANCHI

TL;DR
This scoping review explores how AI using X-ray images can improve orthodontic diagnosis and treatment planning decisions.
Contribution
The study categorizes AI applications in orthodontics and identifies key areas where AI enhances clinical decision-making.
Findings
AI models, especially Deep Learning, are used with X-ray images like lateral radiographs in orthodontics.
AI shows promise in diagnosing TMJ osteoarthritis, skeletal maturation, and obstructive sleep apnea.
Most studies focused on orthognathic surgery and skeletal pattern analysis using AI.
Abstract
Artificial intelligence (AI) in health has increased its applications over the last years. The large amount of data available due to the improvement of data storage and digital exams provided better knowledge in treatment planning and opened new possibilities of applications of AI in Orthodontics’ diagnosis and treatment planning. The aim of this scoping review was to examine when AI models enhance the clinical decision-making process in orthodontic diagnosis and treatment planning, with a focus on the utilization of X-ray-based imaging. Individual eletronic search strategies were developed and conducted on PubMed/Medline, Scopus, Web fo Science, Embase, Lilacs, and Cochrane Library (only English language articles published from January 2000 to October 20, 2021), aiming for relevant studies that met the eligibility criteria. 12 studies were included, categorized in 5 different…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
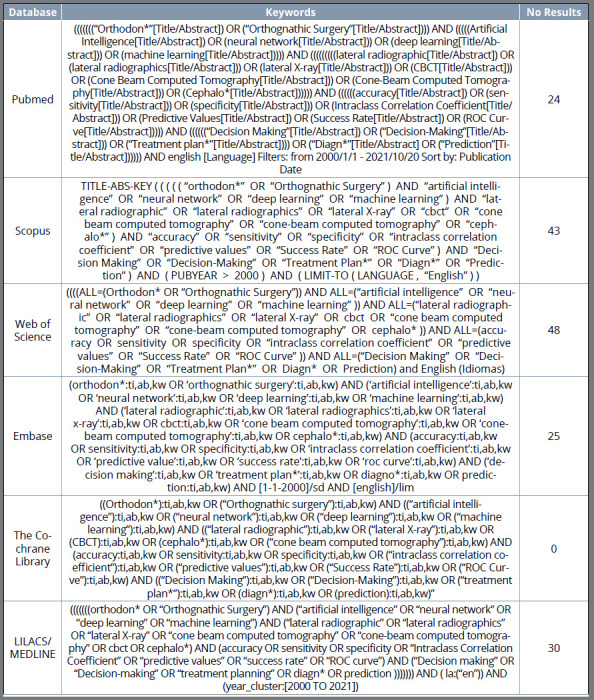 Figure 1
Figure 1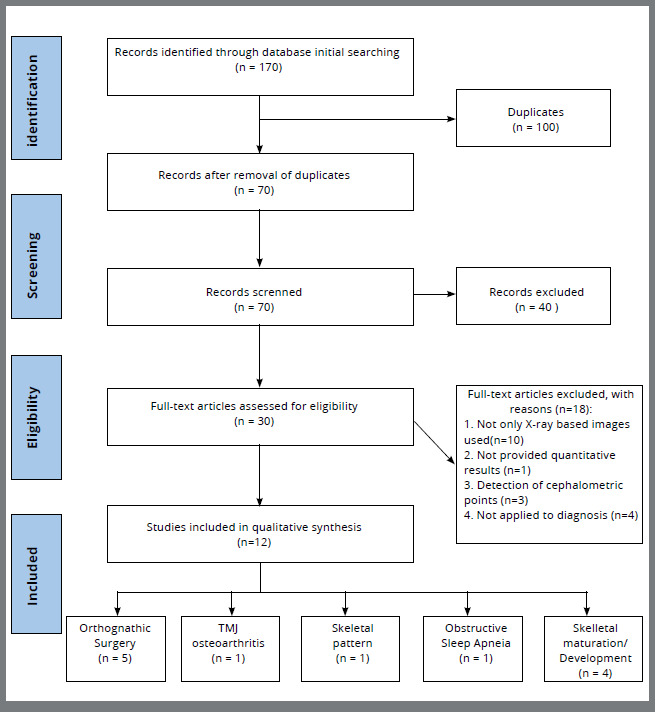 Figure 2
Figure 2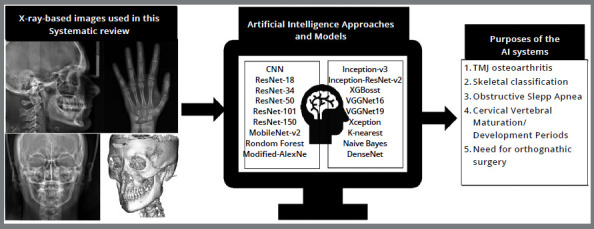 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Radiography and Imaging · Orthodontics and Dentofacial Orthopedics · Temporomandibular Joint Disorders
INTRODUCTION
Artificial intelligence (AI) is a term used to describe the ability that computational models can learn and improve their accuracy based on experience or labeled data, imitating the way that humans can learn. Its application is over streaming services, cellphones, websites, social medial etc.1 ^,^ 2
The inclusion of AI systems in the health area is an emerging topic, that has increased over the last years mainly because clinicians and researchers have more access to different exams generating a large volume of data.1 However, this data may be underused due to the lack of proper decision-making support systems, lack of standardization, and there is still a need for more collaborative data pooling to fuel databases.3 Ideally any data must follow the “4vs” (volume, velocity, variety, and veracity), which could lead to more robust data analysis.1
Several studies with AI have been made in different fields of dentistry,3 ^-^ 5 with different purposes, from detecting teeth and caries,6 ^-^ 9 periapical pathosis,10 ^-^ 12 and tonsils hypertrophy,13 ^,^ 14 to predict treatments, such as the need for extractions15 ^-^ 18 or orthognathic surgery.19 ^-^ 25
One subset of AI that is commonly used in the health area is convolutional (artificial) neural networks (CNN or ANN) that can be used to identify and classify images. They are called neural networks because their structure reminds the human brain networks. It can be used for raw to high-definition specific images, detection of cephalometric landmarks on lateral cephalograms, or cone-beam computed tomography (CBCTs).26 ^-^ 30 AI can also be used to assist and improve the decision-making process. It may happen because these models take large amounts of data and usually are based on expert experience or gold standard patterns.5 ^,^ 18 ^,^ 20 ^,^ 31 ^-^ 34
Dentistry usually provides unstructured data such as clinical data, models, photographs, and X-ray images. This type of data is difficult to analyze than structured because it is usually composed by qualitative data. However, it is’ possible to conduce researches using only unstructured data, like X-ray-based images, by using non-relational databases or by transferring unstructured data (qualitative) to structured data (quantitative).1 ^,^ 35 ^,^ 36
Radiographic image exams, such as CBCTs and lateral radiographs, are widely used because of the standardization and capability to provide quantitative data and images that can be extracted, segmented, and enhanced so imaging deep learning (DL) models can recognize them. In addition, the X-ray images play an essential role in diagnosis and planning.26 ^,^ 27
Still, there is a large amount of information on this field, and the aim of this scoping review was to examine when AI models enhance the clinical decision-making process in orthodontic diagnosis and treatment planning, with a focus on the utilization of X-ray-based imaging.
METHODS
PROTOCOL AND REGISTRATION
The protocol of this scoping review was registered in PROSPERO under the number CRD42021259994 in the NHS (National Institute for Health Research) database at https://www.crd.york.ac.uk/prospero/. The present review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.37
ELIGIBILITY CRITERIA
The PICOS plus inclusion criteria was used as inclusion criteria (Table 1). All included manuscripts were experimental or observation studies focused on AI applied to radiographic imaging exams and its application to Orthodontics diagnosis and treatment planning. Also, they should provide performance metrics or predictive outcomes that could be quantified, such as accuracy, sensibility, ROC curves, and there should be a clear mention regarding the data sets used for assessing the model. The exclusion criteria were articles that were not AI related, used more than just X-ray-based images, were not applied to diagnosis or treatment planning, were written in languages different than English, case reports, expert opinions, and letters to editors.
Table 1:Inclusion criteria.PICOSDescriptionPopulationX-ray based studies focused on diagnostic or planningInterventionUse of AI for diagnostic or planning purposesComparatorExpert opinions, human diagnosis or gold standardOutcomePerformance metrics (accuracy, sensibility, sensitivity...)Study designObservational or experimental studiesQuestionHow does artificial intelligence can be applied to orthodontic diagnosis and planning using x-ray based images?
INFORMATION SOURCES AND SEARCH STRATEGY
Individual electronic search strategies were developed and conducted on PubMed/Medline, Scopus, Web of Science, Embase, Lilacs, and Cochrane Library published from January 2000 to October 20, 2021, and only English publish articles (Fig. 1).
Figure 1:Search strategy.
SELECTION PROCESS
The selection was completed in phases. First, titles, keywords and abstracts were reviewed by two investigators (PHJO and JOLP) separately using the inclusion and exclusion criteria to screen the articles. Duplicated articles were accessed using Mendeley (https://www.mendeley.com)[38](#B38) and double checked using Microsoft Excel^?^. Secondly, full texts of the possible eligible studies were assessed and classified as no, maybe, or yes according to the inclusion and exclusion criteria by the two investigators. The ones marked with no for both investigators were excluded, while the ones marked as maybe were resolved through consensus to decide if they would be included or not based on the PICOS and inclusion criteria.
DATA CHARTING PROCESS AND DATA ITEMS
Data charting was conducted by an independent investigator (PHJO) and checked by a second (JOLP). The following data were collected from each article, as follows: author, year of publication, country, study design, sample, mean/range of age, which X-ray based exam was used, aim, algorithm architecture, performance metrics, author suggestion, recommendations and limitation, results, and conclusions.
STUDY RISK OF BIAS ASSESSMENT AND CRITICAL APPRAISAL OF INDIVIDUAL STUDIES
The risk of bias has not assessed, because the aim of the included manuscripts was to assess statistical machine-learning approaches based on pre-selected imaging exams, rather than the clinical aspects of the sample recruitment, or methodologies during the study’s conduction. In AI systems, the BIAS usually is resulted from the algorithm training itself, which there is no specific standard tool to measure this in scoping reviews. Meta-analysis was not conduced since the risk of bias was not assessed. Also, intervention, metrics or outcomes, and study settings were different in the selected studies.39
SYNTHESIS OF RESULTS
For didactic purposes, the included studies were separated in 5 different categories, according to what was evaluated: (1) Orthognathic surgery, (2) TMJ osteoarthritis, (3) Skeletal pattern, (4) Obstructive Sleep Apnea (OSA), and (5) Skeletal maturation/development.
RESULTS
STUDY SELECTION
A total of 170 studies were retrieved in our search following the previously defined strategy. Duplicate removal and screening were performed, and 30 studies were selected for full-text assessment. After eligibility criteria was carefully applied to the full texts, 18 studies were excluded because they were not based only on x-ray images, did not provide quantitative results, could not be applied directly to diagnosis or treatment planning, or aimed to detect cephalometric landmarks. Finally, 12 studies met the eligibility criteria and were included. The PRISMA flowchart showing the process of selection is presented in Figure 2.
Figure 2:Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) flow diagram of the study selection process.
STUDY CHARACTERISTICS
The studies were divided into groups according to the AI application and what was evaluated (Fig. 3).
Figure 3:The different X-ray-based images that were used in this scoping review such as lateral radiographs (A), hand-wrist radiographs (B), Posterior radiographs (C), and CBCTs (D). Followed by different machine/deep learning methods that are present in the selected studies and the purposes of the use of AI systems in Orthodontics that are shown in this scoping review.
RESULTS OF INDIVIDUAL STUDIES AND SYNTHESIS OF RESULTS
Orthognathic surgery: Five studies were included regarding the application of AI to predict the need for orthognathic surgery or conventional Orthodontics21 ^-^ 25 (Table 2). Shin et al.21 demonstrated that the DL network proposed by them can standardize the decision process for orthognathic surgery and help orthodontists using posterior and lateral radiographs. Their results for accuracy, sensitivity, and specificity were 0.954, 0.844, and 0.993, respectively. Lin et al.22 was the only study that showed results lower than 90% for accuracy or success rate in predicting the need for orthognathic surgery. However, they evaluated that ANB angle, facial convexity angle, and the maxillary plan to Frankfurt plane angle were the main parameters to define the need for surgery. Lin et al.23 used four different CNN models to predict facial symmetry after orthognathic surgery using CBCT images. Xception model was the most suitable for this purpose with 90% accuracy. Kim et al.24 showed that ResNEt-18 and 34 showed better performance than Resnet-50 and 101 to predict the need for orthognathic surgery using lateral radiographs. The results for the four CNN models test were as follows: Area Under the Curve (AUC): 0.979 (ResNet-18), 0.974 (ResNet-34), 0.945 (ResNet-50), 0.944 (ResNet-101). Accuracy: 0.938 (ResNet-18), 0.936 (ResNet-34), 0.911 (ResNet-50), 0.913 (ResNet-101). Sensitivity: 0.882 (ResNet-18), 0.876 (ResNet-34), 0.806 (ResNet-50), 0.824 (ResNet-101). Specificity: 0.966 (ResNet-18), 0.966 (ResNet-34), 0.964 (ResNet-50), 0.958 (ResNet-101). Lee et al.25 showed that Deep Convolutional Neural Networks (DCNN) can be applied to predict orthognathic surgery and show which structure is the most important for diagnosis. Modified-Alexnet showed higher AUC and accuracy (0.969 and 0.919) than MobileNet (0.908 and 0.838) and ResNet-50 (0.923 and 0.838). The algorithm architecture used for all studies in this section was deep learning based.21 ^-^ 25
Table 2:Summary of descriptive characteristics of individual articles.NameAuthor, Year, CountryStudy DesignSample (n) Mean/Range of Age(yr)Imaging AnalysisAimAlgorithm ArchitecturePerformance metricsAuthor suggestions/recommendationsLimitationsWhat was evaluatedResultsConclusionsAUTOMATED DETECTION OF TMJ OSTEOARTHRITIS BASED ON ARTIFICIAL INTELLIGENCELee et al.,2020, Korea44 Retrospective314 (3,514 images)mean ± SD age, 39.5 ± 18.2 y CBCTto develop a diagnostic tool to detect condylar resorption from CBCT images with AI A single-shot detector (SSD)-a deep learning framework designed for object detection Accuracy, precision, recall, and F1 score additional imaging modalities, such as contrast enhanced MRI and bone scintigraphy, could provide more information with higher accuracy over TMJ's inflammation.Only 1 observer classified the TMJ images in the training data set. TMJ osteoarthritis on CBCT on adult patientsThe average accuracy, precision, recall, and F1 score over were 0.86, 0.85, 0.84, and 0.84, respectively. TMJOA from sagittal CBCT images is possible by using a deep neural networks model. AUTOMATED SKELETAL CLASSIFICATION WITH LATERAL CEPHALOMETRY BASED ON ARTIFICIAL INTELLIGENCEYu et al., 2020, Korea43 Retrospective5890 patientsmean 25.4 yLateral radiographsPropose a novel deep learning system that provides the fully automated, 1-step, end- to-end diagnosis for skeletal classification solely from the lateral cephalogram. A multimodal convolutional neural network architecture with a modified DenseNet with pretrained weights for the ImageNet data setSensitivity, Specificity, AUC and AccuracyTo optimize diagnosis, skeletal components and severity of the discrepancy should be evaluated in future studies. Also, further research comparing this system and the original approach with landmark detection and additional studies on enhancing model performance are needed.Data was collected from a single organization which may cause a selection bias Three different models to evaluate sagittal and vertical skeletal pattern of patientsSensitivity, Specificity, AUC and Accuracy for sagittal discrepancies were 93.55%, 96.77%, 0.965 to 0.991 and 95.70%, respectively. Sensitivity, Specificity, AUC and Accuracy for vertical discrepancies were 94.59%, 97.29%, 0.967 to 0.995 and 96.40%Skeletal classification can be made with an AI-aided tool for sagittal and vertical discrepancies MACHINE LEARNING FOR IMAGE-BASED DETECTION OF PATIENTS WITH OBSTRUCTIVE SLEEP APNEA: AN EXPLORATORY STUDYTsuiki et al., 2020, Japan45 Retrospective1389 patients (OSA = 867; control = 522)OSA = 49.7 ± 8.9 Control = 41.2 ± 13.0Lateral radiographstest the hypothesis that a machine learning model could be used to differentiate severe OSA and non-OSA by 2-dimensional images DCNN model called Visual Geometry Group (VGG-19)Sensitivity, Specificity, Positive and negative likelihood ratio, Positive and negative predictive values and AUC area were evaluated for the three different groupsBy the combination of demographic characteristics, anthropometric features and lateral cephalometric images may provide different AI models that could contribute to detect OSAData includes only Asian males from a single centerIf this DCNN model could be used to detect patients with OSA based on 2-D images using three different areas of interest: Original image, main region and head only Sensitivity, Specificity, Positive and negative likelihood ratio, Positive and negative predictive values and AUC area were evaluated for the three different groups: - Full image: 0.90, 0.77, 3.88, 0.14, 0.87, 0.82 and 0.89, respectively. - Main Region: 0.84, 0.81, 4.35, 0.20, 0.88, 0.75 and 0.92, respectively. - Head only: 0.71, 0.63, 1.91, 0.46, 0.85, 0.42 and 0.70, respectivelyThe DCNN accurately identified individuals with severe OSA using lateral cephalometric radiographsCOMPARISON OF DEEP LEARNING MODELS FOR CERVICAL VERTEBRAL MATURATION STAGE CLASSIFICATION ON LATERAL CEPHALOMETRIC RADIOGRAPHSSeo et al, 2021, Korea42 Observational6006-19 yearsLateral radiographsevaluate and compare the performance of six state-of-the-art CNN-based deep learning models for CVM on lateral cephalometric radiographs, and implement visualization of CVM classification for each model using Grad-CAM technology Different CNN models (ResNet-18, MobileNet-v2, ResNet-50, ResNet-101, Inception-v3 and Inception-ResNet-v2)accuracy (1), recall (2), precision (3), F1-score (4), and area under the curve (AUC) values from the ROC curveHigher quality data and development of better CNN architectures may improve the model's performance. It would be easier to evaluate if cervical vertebrae were segmented from surrounding structuresSmall dataIf different CNN models can distinguish the CVM classification on lateral cephalometric radiographsAccuracy was higher than 90% for all models. Inception-ResNet-v2 showed the best results for all metricsDEEP CONVOLUTIONAL NEURAL NETWORKS BASED ANALYSIS OF CEPHALOMETRIC RADIOGRAPHS FOR DIFFERENTIAL DIAGNOSIS OF ORTHOGNATHIC SURGERY INDICATIONSLee et al., 2020, Korea25 Retrospective333 individuals23.1 ± 5.1Lateral radiographsCreate a model for the differential diagnosis of orthognathic surgery and orthodontic treatment with a DL algorithm using cephalometric radiographs.Three DL models were tested: Modified-Alexnet, MobileNet and Resnet50Sensitivity, Specificity, AUC and AccuracyFuture studies can be obtained when assessed with more data. Also, should analyze the impact of better model construction and their comparison with other modelsComparison of the performance was limited due to the lack of dataDifferential diagnosis for orthognathic surgery based on cephalometric radiographs using three different DL models Modified-Alexnet: 0.852 (Sensitivity), 0.973 (Specificity), 0.969 (AUC) and 0.919 (Accuracy). MobileNet: 0.761 (Sensitivity), 0.931 (Specificity), 0.908 (AUC) and 0.838 (Accuracy). Resnet50: 0.750 (Sensitivity), 0.944 (Specificity), 0.923 (AUC) and 0.838 (Accuracy).DCNN can be applied to predict orthognathic surgery. Also it was possible to predict the most important diagnosis structuresDEEP LEARNING BASED PREDICTION OF NECESSITY FOR ORTHOGNATHIC SURGERY OF SKELETAL MALOCCLUSION USING CEPHALOGRAM IN KOREAN INDIVIDUALSShin et al, 2021, Korea21 Observational840 (Class II:244, Class III: 477, Assimetry: 149) (Male: 461, Female: 379) 23.2yPosterior and lateral radiographsDevelop a deep learning network to automatically predict the need for orthodontic surgery using cephalogram. ResNet34, with convolution blocks stacked hierarchically (CNN)accuracy, sensitivity, and specificity.More studies should be encouraged to achieve public confidence.Involves only Korean patients from only one hospital and small number of cases.Exploited a deep learning framework to automatically predict the need for orthognathic surgery based on the cephalogram of the patientsaccuracy, sensitivity, and specificity were 0.954, 0.844, and 0.993, respectivelyDL can standardize the decision process and help orthodontistsDETERMINATION OF GROWTH AND DEVELOPMENT PERIODS IN ORTHODONTICS WITH ARTIFICIAL NEURAL NETWORKKök et al., 2021, Turkey40 Retrospective419 patients (CVM1:70, CVM2:70, CVM3:69, CVM4:70, CVM5:70, CVM6:708 to 17yLateral and hand-wrist radiographsDetermine the growth-development periods and gender from the cervical vertebrae using the artificial neural network (ANN).Twenty-four ANN models were obtained and seven with success level and clinically applicable were selectedAccuracy, Sensitivity, Specificity and F1 scoreUsing all the information from cephalometric radiograph in addition to linear measurements can provide better resultsHand-wrist age determination is more advanced than cephalometry and cervical vertebra.If the ANN models could determinate patient's cervical vertebral stage and gender. The accuracy for the testing set was: 71.4% (ANN-1), 49.2% (ANN-2), 76.1% (ANN-3), 50.7% (ANN-4), 69.8% (ANN-5), 81% (ANN-6), 90.4% (ANN-7), 90.5% (ANN-Gender)The growth-development periods and gender were determined from the cervical vertebrae by using ANN with satisfactory successEARLY PREDICTION OF THE NEED FOR ORTHOGNATHIC SURGERY IN PATIENTS WITH REPAIRED UNILATERAL CLEFT LIP AND PALATE USING MACHINE LEARNING AND LONGITUDINAL LATERAL CEPHALOMETRIC ANALYSIS DATALin et al., 2021, Korea22 Retrospective56 patientsT0: 6.3y and T1: 16.7yLateral radiographsDetermine the cephalo- metric predictors of the future need for orthognathic surgery in patients with repaired unilateral cleft lip and palate (UCLP) using machine learning.Boruta method to identify the most relevant features out of the cephalometric predictors at T0 and XGBoost algorithm to predict the future need for orthognathic surgery10-fold cross-validation accuracy with F1-score Multi-center study to increase the sample.Small sample size.The most important features of the cephalogram and the need for orthognathic surgeryThe prediction model had 87.4% accuracy and when ANB, PP-FH, CF and FCA variables are inserted At age of 6 years, it was possible to predict the future need for orthognathic surgery using cephalometric predictors with a good accuracy INFLUENCE OF THE DEPTH OF THE CONVOLUTIONAL NEURAL NETWORKS ON AN ARTIFICIAL INTELLIGENCE MODEL FOR DIAGNOSIS OF ORTHOGNATHIC SURGERYKim et al., 2021, Korea24 Retrospective960 patients (non-surgical: 640, surgical: 320)24.6 ± 4.9Lateral radiographsinvestigate the relationship between image patterns in cephalometric radiographs and the need for orthognathic surgery, and report on a method for improving the accuracy of predictive models according to the depth of the neural network CNN models (ResNet-18, 34, 50 and 101)AUC, Accuracy, Sensitivity and SpecificityMulti-center data to improve the model's performance. Single center study.Predict the need of orthognathic surgery using cephalometric radiographsAUC: 0.979 (ResNet-18), 0.974 (ResNet-34), 0.945 (ResNet-50), 0.944 (ResNet-101). Accuracy: 0.938 (ResNet-18), 0.936 (ResNet-34), 0.911 (ResNet-50), 0.913 (ResNet-101). Sensitivity: 0.882 (ResNet-18), 0.876 (ResNet-34), 0.806 (ResNet-50), 0.824 (ResNet-101). Specificity: 0.966 (ResNet-18), 0.966 (ResNet-34), 0.964 (ResNet-50), 0.958 (ResNet-101).ResNet-18 and 34 had better performance than ResNet-50 and 101 models.ON CONSTRUCTION OF TRANSFER LEARNING FOR FACIAL SYMMETRY ASSESSMENT BEFORE AND AFTER ORTHOGNATHIC SURGERYLin et al., 2021, Taiwan23 Retrospective71 patients-CBCTA CNN model with a transfer learning approach for facial symmetry assessment based on 3-dimensional (3D) features to assist physicians in enhancing medical treatments. CNN models (VGGNet16, VGGNet19, ResNet50 and Xception)AccuracyLarger number of data and more effective NN architectures can enhance the accuracyThe model can only be used for small data sets and can't be trained by new DL architecture.Predict facial symmetry scores using the trained model.The accuracy for VGG16, VGG19, ResNet50 and Xception was: 80%, 86%, 83% and 90%, respectively.The most suitable model for the transfer learning was Xception modelPREDICTION OF HAND-WRIST MATURATION STAGES BASED ON CERVICAL VERTEBRAE IMAGES USING ARTIFICIAL INTELLIGENCEKim et al., 2021, Korea31 Retrospective499 images from 455 patients9.9 ± 2.6Lateral and hand-wrist radiographs Predict the hand-wrist maturation stages based on the CV images observed in lateral cepha- lograms, and to analyse the accuracy of the proposed algorithms. Various combinations of regression models were usedMean Absolute Error (MAE), round MAE, Root Mean Square of Error (RMSE) and AccuracyFurther studies with a larger sample with na even distribution of sex, chronological age and skeletal maturation. More features can also improve the prediction accuracy.Small sample size and imbalanced data with a great number of patients whose SMI stage was 0.Patients hand-wrist maturation based on CV images and its accuracy.The final ensemble model consisted of eight machine learning models. The MAE, round MAE and RMSE were 0.90, 0.87 and 1.20, respectively.Chronological age and sex increased the accuracy. CV images can be used to predict hand-wrist SMI using machine learning.USAGE AND COMPARISON OF ARTIFICIAL INTELLIGENCE ALGORITHMS FOR DETERMINATION OF GROWTH AND DEVELOPMENT BY CERVICAL VERTEBRAE STAGES IN ORTHODONTICSKök et al., 2019, Turkey41 Retrospective300 patients8 to 17yLateral radiographsdetermine cervical vertebrae stages (CVS) for growth and development periods by the frequently used seven artificial intelligence classifiers, and to compare the performance of these algorithms with each other. Seven algorithms were selected:k-nearest neighbors (k-NN), Naive Bayes (NB), decision tree, ANN, SVM, Random forest and logistic regressionAUC, Accuracy, Precision, F1 score and RecallThere are no author suggestions or recomendations for future studies.The author's did not mentioned any limitations over the studyUse seven different algorithms to determine cervical vertebrae stages from cephalometric radiograph and compare their performanceDecision tree had the highest accuracy for CVS1 to CVS4 (97.1%, 90.5%, 73.2%, 58.5%, respectively) and kNN for CVS5 (60.9%) and CVS6 (78.7%). ANN had the second-highest accuracy, except for CVS5.ANN is the preferred method for determining CVS because it was the most stable algorithm
Skeletal maturation/development: Four studies regarding the application of AI to assess development or skeletal maturation31 ^,^ 40 ^-^ 42 (Table 2). Kim et al.31 showed that cervical vertebrae (CV) images can be used to predict hand-wrist SMI by presenting a model consisted of eight ML models. Also, age and sex can increase the accuracy. Kök et al.40 concluded that growth development periods and gender can be predicted using ANN. The higher accuracy (0.942) was present by ANN-7 (composed by all 32 linear measurements) followed by ANN-Gender (ANN7+gender). Kök et al.41 results showed that ANN was the most stable algorithm to predict CV stages (CVS1-CVS6) with accuracy results of 93%, 89.7%, 68.8%, 55.6%, 47.4% and 78%, respectively. All studies used lateral radiographs and more than one DL model. However, only Seo et al.42 did not use hand-wrist radiographs as a comparison method. They evaluated and compared six different CNN-based DL models to classify Cervical Vertebral Maturation (CVM). All of them had accuracy higher than 90% and also AUC higher than 90% for all CVM stages. All studies showed that AI can be used to predict skeletal maturation.
Skeletal classification: One study was included regarding the application of AI to classify patients’ skeletal patterns (Table 2). Yu et al.43 evaluated sagittal and vertical discrepancies on lateral radiographs using CNN. It showed results higher than 90% for both skeletal classifications and presented heat maps for a better understanding of the region that influences the most to distinguish skeletal patterns.
TMJ osteoarthritis (TMJOA): One study was included regarding the application of AI to detect TMJ osteoarthritis. Lee et al.44 showed that sagittal CBCT images and deep learning are capable to predict TMJOA. The DL used was a single-shot detector. The authors evaluated accuracy, precision, recall, and F1 score. The results were 0.86, 0.85, 0.84, and 0.84, respectively. The authors suggested that additional imaging modalities should improve the performance of the DL and provide more information on the TMJ inflammation (Table 2).
Obstructive Sleep Apnea (OSA): One study was included regarding the application of AI to detect OSA. Tsuiki et al.45 showed that DCNN model (VGG-19) can accurately identify OSA using lateral radiographs (Table 2). The authors divided the sample images into three groups according to the area that was evaluated as follows: full images (original images), main region (facial profile, the upper airway, and craniofacial soft and hard tissues), and head only (occipital region). The main region had the best results for sensitivity, specificity, and AUC (0.84, 0.81, 0.92) followed by full image (0.9, 0.77, and 0.89), and head only (0.71, 0.63, and 0.7). The authors suggested that demographic characteristics and anthropometric features could improve the diagnostic OSA.
DISCUSSION
SUMMARY OF EVIDENCE
To our knowledge, this is the first scoping review to present X-ray imaging-based AI models applied to diagnosis and treatment planning. As a limitation, we have excluded manuscripts that used panoramic images because the studies were not focused on the Orthodontics’ diagnosis or planning. In most reviewed papers, authors divided AI applications in Orthodontics based on radiographic images into two groups: diagnosis and treatment planning.
Diagnosis. Diagnosis is probably the most important aspect of orthodontic treatment. Assessing development and skeletal maturation is needed for patients still growing and present skeletal alterations. With that is possible to provide the best treatment for each developmental period.46 ^-^ 48 The cervical vertebrae method49 is commonly used to identify maturation stages because it can be assessed in lateral radiographs. However, due to its subjectivity and the chance of distortion depending on the patient positioning, clinicians need to have specific training to use this method. That is one of the reasons why hand-wrist radiographs are still the gold standard for assessing the development stage of a patient.50 However, AI can be used to help orthodontists to identify the CVM stages. All the studies assessed here showed that AI had good results assessing the development stage of patients using lateral radiographs when compared to gold standard or to humans’ evaluation. Furthermore, the different studies showed that ANN model had best results when compared to other AI models.31 ^,^ 40 ^-^ 42
Facial analysis and skeletal classification play an important role in Orthodontics’ diagnosis. All the growth deviations that the patient had will produce a skeletal alteration, and the orthodontist must classify the patient properly in all 3 planes.51 ^-^ 53 However, lateral radiographs can only classify vertical and sagittal relationships. Yu et al.43 aimed to used DL to assess skeletal classification and, unlikely previous studies, they did not use CNN models to perform cephalometric landmarks. The authors justified that eliminating this process would improve the classification performance. For assessing vertical relationships, it was used the Bjork’s Sum and Jarabak’s Ratio and the results showed 96.4% accuracy. For sagittal relationships, the ANB angle and Wits’ appraisal were used and a 95.7% accuracy was obtained.
Patients with OSA usually present a retrognathic mandible and/or a lower hyoid position with causes a more crowded oropharynx. Patients with OSA can be diagnosed in lateral radiographs, mainly when it is a severe case. However, 3D images still provide better and more qualified data. Tsuiki et al.45 evaluated 3 types of images: full lateral radiographs images, the main airway region (including facial profile, teeth, cervical bones, maxilla, and mandible), and the occipital region. Best results were obtained for the main region, and the worst were at the occipital region. Also, their results are comparable with the manual cephalometric analysis. It shows that the use of DL models can be applied as an objective additional diagnosis method to OSA patients.
TMJ osteoarthritis is a multi-system disease. CBCTs allow dentists to diagnose the TMJ bone by finding irregular contour, osseous defects, cortical loss or flattening of the condyles.54 Early diagnosis can be the best chance to minimize the damage caused by osteoarthritis, since there is no treatment available yet. Lee et al.44 evaluated if AI could detect TMJOA in CBCT sagittal images. The results showed that using only the CBCT sagittal images had results higher than 80% like Bianchi et al.,55 that used CBCT, clinical and biological data.
Treatment Planning. Once the diagnosis is placed, treatment planning is the next step in orthodontic treatment. It is important to enhance that treatment planning needs radiographic images, facial evaluation, and models to be made, mainly for borderline patients. The proper decision to treat with orthodontic treatment or orthognathic surgery usually requires more experience from the orthodontist.51 ^,^ 56 ^,^ 57 All studies presented here had results higher than 90% when studied adult patients that need surgical treatment. Lin et al.22 was the only study that used young patients with unilateral cleft lip and palate and had 87.4% accuracy and was the only one to use cephalometric measures. The other studies21 ^,^ 23 ^-^ 25 used DCNN to extract features and identify the structures that play an important role in the decision. The authors justify that by saying that the marking and measurement values can be a bias. This model resembles an orthodontist’s subjective or morphological analysis. Previous studies19 ^,^ 58 compared the orthodontists’ impression and cephalometric values and have concluded that there is the correlation between both analyses.
Limitations. The main limitation of this scoping review was that most studies that apply AI to Orthodontics usually needs multi-source data, rather than x-rays-based image alone. For this reason, we retrieve only 12 manuscripts that meet our PICOs criteria. Also, we have not assessed the BIAS of each AI model due to the lack of standardized tools for this purpose. In addition to that, the lack of general applicability is a major limitation in AI models because most of the data are from the same center. We believe that with a greater number of studies conducted using AI to assist in diagnosis and planning, with more data and preferably multicenter studies, we may observe broader clinical applications and improvements in orthodontic software, thereby enhancing the proposed treatment for our patients.
CONCLUSIONS
In fact, AI has already demonstrated its ability to add valuable information and assist in orthodontic treatment planning, diagnostic, and decision-making processes. While AI models are available to enhance the evaluation of specific issues such as TMJ osteoarthritis, skeletal maturation, skeletal classification, OSA, and the need for orthognathic surgery, it is essential to note that these applications are not universally used in orthodontic treatments. Instead, AI’s role is often context-dependent and can be most helpful in particular situations where detailed image analysis and data-driven decision support can provide significant value. Integrating AI into clinical practice will likely continue to evolve, enhancing treatment planning in selective cases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Raghupathi W Raghupathi V Big data analytics in healthcare promise and potential Health Inf Sci Syst 20142332582566710.1186/2047-2501-2-3PMC 4341817 · doi ↗ · pubmed ↗
- 2Park WJ Park JB History and application of artificial neural networks in dentistry Eur J Dent 20181245946013036980910.4103/ejd.ejd_325_18PMC 6178664 · doi ↗ · pubmed ↗
- 3Allareddy V Rengasamy Venugopalan S Nalliah RP Caplin JL Lee MK et al Orthodontics in the era of big data analytics Orthod Craniofac Res 201922181310.1111/ocr.1227931074158 · doi ↗ · pubmed ↗
- 4Machoy ME Szyszka-Sommerfeld L Vegh A Gedrange T Wozniak K The ways of using machine learning in dentistry Adv Clin Exp Med 20202933753843220758610.17219/acem/115083 · doi ↗ · pubmed ↗
- 5Corbella S Srinivas S Cabitza F Applications of deep learning in dentistry Oral Surg Oral Med Oral Pathol Oral Radiol 202113222252383330341910.1016/j.oooo.2020.11.003 · doi ↗ · pubmed ↗
- 6Vinayahalingam S Xi T BergéS Maal T Jong G Automated detection of third molars and mandibular nerve by deep learning Sci Rep 201991900790073122777210.1038/s 41598-019-45487-3PMC 6588560 · doi ↗ · pubmed ↗
- 7Chen H Zhang K Lyu P Li H Zhang L Wu J A deep learning approach to automatic teeth detection and numbering based on object detection in dental periapical films Sci Rep 201991384038403084675810.1038/s 41598-019-40414-y PMC 6405755 · doi ↗ · pubmed ↗
- 8Geetha V Aprameya KS Hinduja DM Dental caries diagnosis in digital radiographs using back-propagation neural network Health Inf Sci Syst 202081883194989510.1007/s 13755-019-0096-y PMC 6942116 · doi ↗ · pubmed ↗