Unilateral Nevoid Hyperkeratosis of the Nipple and Areola: A Case Report of a Rare Entity
Fatema Shamsaldeen, Alsadat Mosbeh, Abeer Albazali

TL;DR
A rare benign skin condition affecting the nipple and areola is reported in a 72-year-old man, highlighting the need to distinguish it from cancerous diseases.
Contribution
This case report documents a rare unilateral male presentation of nevoid hyperkeratosis of the nipple and areola.
Findings
The patient showed unilateral verrucous plaques on the nipple and areola with no signs of malignancy.
Histopathology confirmed the diagnosis of NHNA with features like hyperkeratosis and lymphocytic infiltrate.
Topical corticosteroids led to a good clinical response in the patient.
Abstract
Nevoid hyperkeratosis of the nipple and areola (NHNA) is a rare benign skin disorder that presents as hyperkeratotic, verrucous plaques involving one or both nipples and areola. Although the lesions are asymptomatic, they can raise cosmetic concerns and may clinically mimic serious conditions like Paget’s disease. Histopathology examination is essential for diagnosis and for ruling out malignant conditions. We report a 72-year-old Kuwaiti male with unilateral verrucous plaques persistent over the nipple and areola for six months. Physical examination and mammography revealed no abnormalities, and biopsy showed marked hyperkeratosis, acanthosis, papillomatosis and superficial lymphocytic infiltrate without atypia, consistent with NHNA. The patient was treated with topical corticosteroids with a good response. This case highlights a unilateral male presentation of NHNA, emphasizing the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
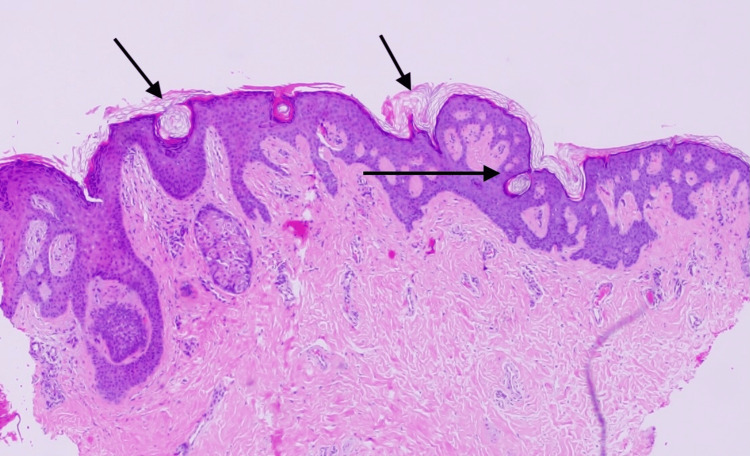 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Skin Diseases and Diabetes · Genetic and rare skin diseases.
Introduction
Nevoid hyperkeratosis of the nipple and areola (NHNA) is a rare skin condition of benign nature, which is characterized by wart-like, hyperkeratotic plaques involving the nipple, areola or both. It can be either unilateral or bilateral. The condition is usually asymptomatic; however, it causes cosmetic concern to the patients. Nevoid hyperkeratosis of the nipple is of unknown etiology; some subtypes are pregnancy-related and suggest a hormonal role. It may resemble in its appearance seborrheic keratosis and navus verrucosis, serious cancerous conditions must be excluded as well. This condition is observed in both males and females, with significantly higher prevalence among females. In this case report, we present a case of Nevoid hyperkeratosis of the nipple in a male patient, highlighting the clinical presentation, diagnosis and management options [1,2].
Case presentation
A 72-year-old Kuwaiti male patient presented to the dermatology clinic with a unilateral nipple lesion that has been causing him discomfort for the past six months. There was no associated history of nipple discharge, itching, bleeding or pain. On examination, the lesion was an erythematous, verrucous plaque with erosions and scaling over the right nipple and areola (Figure 1), no palpable lymph nodes and no similar lesions over the rest of the body. Bilateral breast examination was normal, and the patient has no history of using hormonal therapy. Paget’s disease and Paget's eczema were on the list of differential diagnoses. The patient was referred for a mammogram, which revealed no abnormal findings. Biopsy was done, and histopathology examination revealed marked thickening of the stratum corneum, papillomatous appearance, and minimal superficial dermal perivascular lymphocytic infiltrate, no evidence of cytologic atypia or dysplasia (Figure 2). Thus, a diagnosis of nevoid hyperkeratosis of the nipple and areola was made based on the clinical picture and biopsy findings. The patient was treated with topical steroids with a good response.
Hyperkeratosis, follicular plugging horn and pseudohorn cysts, acanthoses, papillomatosis, and elongated anastomosing rete ridges. Superficial perivascular inflammatory infiltrate forms of lymphohistocytic admixed and melanophages.
Hyperkeratotic, verrucous plaque with erosions and scaling over the right nipple and areola.
Discussion
NHNA is a rare condition that is more common in females. The skin lesion classically manifests as hyperkeratotic plaques described as verrucous lesions. These lesions are typically painless, with no discharge or lymphadenopathy associated with them; however, some patients may experience pruritus, and women may report breastfeeding difficulty [1,2]. In our case, we had a presentation of the lesion that is unilateral lesion in a male patient.
Although the exact cause of NHNA remains unknown, Estrogen levels are thought to contribute to the pathogenesis, as the predominance of cases reported are in women of childbearing age; approximately 80% of cases reported in females of ages between 20-40 years old, and individuals receiving estrogen therapy for certain types of cancer. This supports the hypothesis of hormonal influence [2,3].
The most recent classification of nevoid hyperkeratosis of the nipple broadly classifies it into primary and secondary types. The primary form is idiopathic, usually bilateral and benign. Secondary type is associated with another dermatologic or systemic condition like epidermal nevus or seborrheic keratosis; it can be unilateral or bilateral, and further workup must be done to rule out underlying dermatosis or malignancies [2]. The current case happened to fall under the primary type.
The clinical appearance of the lesion may resemble other dermatological conditions like seborrheic keratosis, acanthosis nigricans, and more serious conditions like Paget’s disease and Paget's eczema. A proper diagnosis through skin biopsy is essential to exclude the potential serious conditions. For diagnosing NHNA, dermatoscopy can show structureless, garish or brown hyperkeratosis. Histopathological examination reveals marked hyperkeratosis, acanthosis and papillomatosis. The basal layer might show hyperpigmentation with a mild lymphocytic infiltrate of the superficial dermis. Most importantly, no atypical cells or pagetoid cells are identified, which helps exclude Paget's disease [4-6]. Our case matches the clinical and histopathological description of nevoid hyperkeratosis of nipple and areola.
When it comes to treating NHNA, both medical and surgical options are available to improve the appearance of the skin. Medical therapies include topical corticosteroids, retinoids and keratolytics like salicylic acid can be used. Multiple case reports showed excellent responses to cryotherapy, reporting complete disappearance of the lesion after six sessions. Other options, like carbon dioxide laser ablation, have a good cosmetic outcome. In some cases, surgical excision is used as an invasive method after all medical treatment fails, with no recurrence reported after two years [7-9]. This case was treated conservatively with topical steroids, with a good response.
Conclusions
NHNA is a rare but benign condition; both males and females can be affected. Early recognition and exclusion of serious dermatological conditions is necessary through clinical evaluation and histopathology confirmation. Management can be conservative with topical steroids and keratolytics or non-conservative, including cryotherapy, laser, and surgical approaches.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nevoid hyperkeratosis of the nipple - A case report and review of literature Clin Dermatol Rev Kumar BS Somaiah SA 16717072023
- 2Unilateral nevoid hyperkeratosis of the nipple: A report of two cases Indian J Dermatol Venereol Leprol Shastry V Betkerur J Kushalappa PA 3033057220061688058010.4103/0378-6323.26730 · doi ↗ · pubmed ↗
- 3Nevoid hyperkeratosis of the areola Int J Dermatol Revert A Bañuls J Montesinos E Jorda E Ramon D Torres V 745746321993 https://doi.org/10.1111/j.1365-4362.1993.tb 02750.x 822572010.1111/j.1365-4362.1993.tb 02750.x · doi ↗ · pubmed ↗
- 4Nevoid hyperkeratosis of the nipple and areola: A distinct entity J Am Acad Dermatol Baykal C Büyükbabani N Kavak A Alper M 4144184620021186217810.1067/mjd.2002.119646 · doi ↗ · pubmed ↗
- 5Hyperkeratosis of the nipple and areola: Report of 3 cases Arch Dermatol Mehanna A Malak JA Kibbi AG 1327132813720011159485710.1001/archderm.137.10.1327 · doi ↗ · pubmed ↗
- 6Dark brown plaques and patches on the breast and areola in a 14-year-old female: Challenge Am J Dermatopathol Succaria F Rosenbaum M Goldberg LJ Mahalingam M 621622372015 https://doi.org/10.1097/dad.00000000000001812619370810.1097/DAD.0000000000000181 · doi ↗ · pubmed ↗
- 7Surgical approach for nevoid hyperkeratosis of the areola J Cutan Aesthet Surg Foustanos A Panagiotopoulos K Ahmad D Konstantopoulos K 4042520122255785610.4103/0974-2077.94343 PMC 3339129 · doi ↗ · pubmed ↗
- 8Naevoid hyperkeratosis of the nipple and areola in a man Br J Dermatol Kubota Y Koga T Nakayama J Kiryu H 38238414220001073078610.1046/j.1365-2133.2000.03320.x · doi ↗ · pubmed ↗