Duration of Folic Acid Supplementation and Adverse Pregnancy Outcomes: A Prospective Multicenter Cohort Study in China
Mingxuan Zhang, Hongzhao Yu, Hongtian Li, Yubo Zhou, Jianmeng Liu

TL;DR
This study in China found that extending folic acid supplementation during pregnancy can reduce risks of certain complications, but may increase gestational diabetes risk in older or overweight women.
Contribution
The study provides new evidence on how the duration of folic acid supplementation affects various pregnancy outcomes, including modifying effects of maternal age and BMI.
Findings
Folic acid supplementation until mid-pregnancy lowers risks of gestational hypertensive disorders and pre-eclampsia.
Supplementation until late pregnancy reduces preterm birth, small for gestational age, and large for gestational age risks.
Advanced maternal age or overweight/obesity is linked to higher gestational diabetes risk with mid-pregnancy supplementation.
Abstract
Background: Folic acid supplementation (FAS) before and in early pregnancy prevents neural tube defects, but the benefits of extending FAS to late pregnancy on pregnancy outcomes remain unclear. We aimed to investigate the associations between duration of FAS and a spectrum of pregnancy outcomes, and to determine whether the associations were modified by maternal age or pre-pregnancy body mass index (BMI). Methods: This prospective multicenter study included 15,694 singleton pregnancies. We used mixed-effects log-binomial regression models to estimate the adjusted risk ratios (aRRs) and 95% confidence intervals (CIs) for gestational diabetes mellitus (GDM), gestational hypertensive disorders (GHDs), pre-eclampsia, preterm birth, macrosomia, small (SGA) and large for gestational age (LGA), and the interaction effects of advanced maternal age and pre-pregnancy BMI. Results: Of 15,694…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
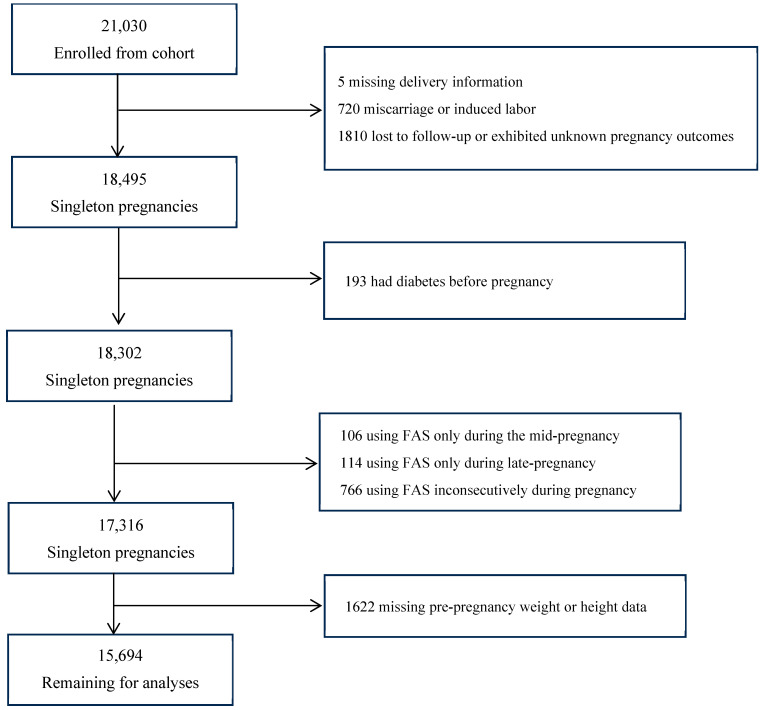 Figure 1
Figure 1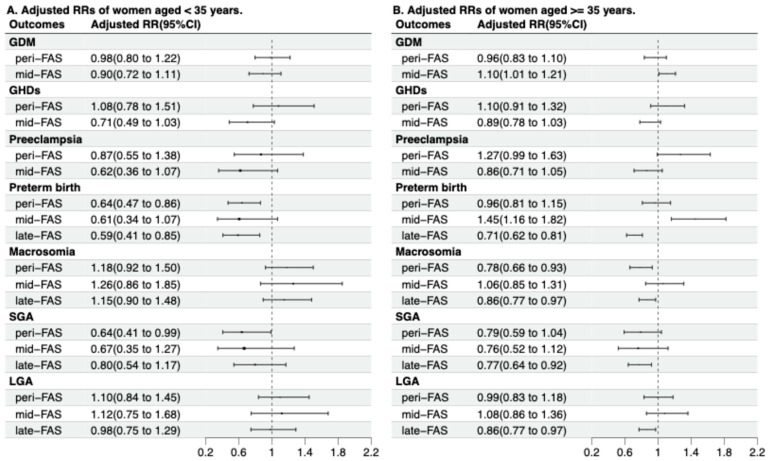 Figure 2
Figure 2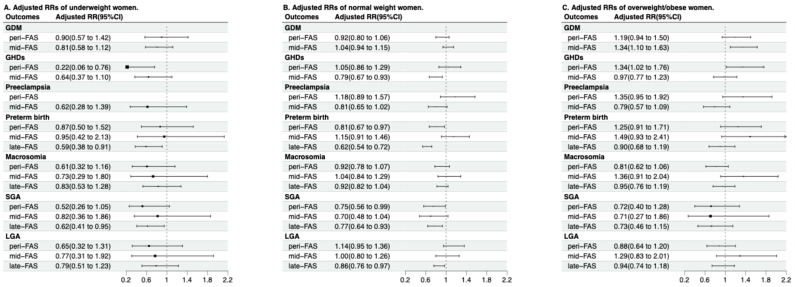 Figure 3
Figure 3- —National Natural Science Foundation of China
- —Clinical Medicine Plus X—Young Scholars Project at Peking University, and the Fundamental Research Funds for the Central Universities
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Gestational Diabetes Research and Management · Vitamin D Research Studies
1. Introduction
Folate is essential for several interconnected one-carbon metabolism pathways, such as nucleotide biosynthesis, amino acid metabolism, and cellular methylation reactions [1]. To reduce the risk of fetal neural tube defects (NTDs), women planning pregnancy are recommended to take folic acid supplementation (FAS), a synthetic and oxidized form of folate [2]. Women should take 400–800 μg of folic acid (FA) as a daily supplement at least one month before anticipated conception and for the first two to three months of pregnancy [3]. However, FAS beyond the first three months has become increasingly prevalent in recent decades. A cohort study conducted in Hunan province, China (2015), reported that 74% of pregnant women who used folic acid supplements continued its use beyond the first three months [4]. Another Chinese cohort study conducted in Tianjin during 2015–2017 showed that approximately 37% of pregnant women used FAS longer than six months [5]. Moreover, extending FAS during pregnancy is more common in the United States and Canada, with 89% of pregnant women taking FAS until late pregnancy [6,7].
Usage of FAS during the periconceptional period for NTD prevention is well established; however, the potential effects of extending FAS to mid- or late-pregnancy stages remain debatable. Prolonged FAS during pregnancy has been linked, in some animal and human studies, to adverse offspring outcomes including metabolic disorders [8,9] and neurobehavioral alterations [10]. Growing evidence suggests that FAS may reduce adverse pregnancy outcomes by modulating placental development and mitigating oxidative stress [11,12,13,14]. However, emerging evidence also suggests that excessive folate might impair insulin resistance [8,15,16,17] and increase the risk of gestational diabetes mellitus (GDM). Some studies reported that longer FAS duration before or at pregnancy was associated with a higher risk of GDM [4,18,19], while the data on the associations between FAS duration and other pregnancy outcomes, such as preeclampsia [20], are sparse. Only one single-center cohort study on 950 participants has focused on the associations between pre-conceptional FAS duration (longer or less than three months) and multiple pregnancy outcomes, including GDM, cesarean delivery, preterm birth, early-term birth, macrosomia, low birth weight, small for gestational age (SGA), and large for gestational age (LGA) [4]. This study found that using FAS for three months before pregnancy was associated with increased risk of GDM and reduced risk of SGA. Nonetheless, the effects of FAS during pregnancy warrant further investigation. To guide FAS during pregnancy, a thorough understanding of the associations of FAS duration across pregnancy with a spectrum of pregnancy complications and birth outcomes is essential. Additionally, it is also unclear whether these associations vary by maternal age and pre-pregnancy body mass index (BMI). These factors might be related to the folate status [21,22] and have changed drastically with the development of society and fertility policy in China [23,24].
Using a multicenter prospective Chinese cohort data, we aimed to examine the associations between the duration of FAS as well as several pregnancy and birth outcomes. We also sought to investigate whether these associations, if any, varied by mother’s age and pre-pregnancy BMI. Furthermore, we sought to determine whether these associations were modified by maternal age or pre-pregnancy BMI.
2. Materials and Methods
2.1. Participants and Study Design
Based on the University Hospital Advanced Age Pregnant (UNIHOPE) cohort (ClinicalTrials No.: NCT03220750), our prospective multicenter cohort study was conducted at eight tertiary hospitals across the southern and northern regions of China from March 2017 to June 2021 [25]. Since we aimed to investigate the risk factors of adverse pregnancy outcomes among women with advanced maternal age, women with an anticipated delivery at age ≥ 35 years were primarily recruited. For potential comparisons, we additionally recruited a small proportion of younger females (<35 years at delivery). To be eligible for the UNIHOPE cohort, participants needed to be in early pregnancy, receiving prenatal healthcare, and planning to deliver at the study hospitals. We excluded those participants who did not provide informed consent or exhibited mental disorders. We recruited both singleton and twin pregnancies and used the sub-cohort data of singleton pregnancies.
The participants provided baseline information at enrollment before 14 gestational weeks and completed follow-ups at 24–28 weeks and 32–34 weeks of gestation, after delivery, and 6–12 postpartum weeks, respectively. Trained nurses or obstetricians collected the baseline information on the mother’s age, height, pre-pregnancy body weight, ethnicity, education level, smoking and alcohol consumption within six months before pregnancy, parity, and conception mode using a structured questionnaire. Information on FAS duration, pregnancy complications, and birth outcomes was collected during follow-ups. Using the WHO criterion, we calculated the pre-pregnancy BMI by dividing the pre-pregnancy weight in kilograms by height in meters squared. It was categorized as underweight (<18.5 kg/m^2^), normal-weight (18.5 to <25.0 kg/m^2^), overweight (25 to <30 kg/m^2^), or obese (≥30 kg/m^2^), respectively.
Among our 21,030 singleton pregnant participants, we excluded those with missing delivery information (n = 5); who had miscarriage or induced labor (n = 720); were lost to follow-up or exhibited unknown pregnancy outcomes (n = 1810); had diabetes before pregnancy (n = 193); or participants using FAS only during the mid-pregnancy stage (n = 106), only during late pregnancy (n = 114), or inconsecutively during pregnancy (n = 766); or those with missing pre-pregnancy weight or height data (n = 1622). Finally, 15,694 participants were analyzed (Figure 1). Maternal and child characteristics were comparable between included (n = 15,694) and excluded participants (n = 5336) (Table A1).
The study was approved by the Institutional Review Board/Human Subjects Committee of the Peking University Health Science Center (IRB00001052-16009; date of approval: 7 April 2016).
2.2. Exposure and Outcomes
Our study’s exposure was FAS duration, which was collected by asking participants whether they were using FAS regularly during the periconceptional period, mid-pregnancy, and late-pregnancy stages, respectively. These supplements included FA tablets, containing 400 μg FA per pill, and multivitamins, which predominantly contain 400 μg or 800 μg FA per pill, depending on the brands [26]. The duration of FAS was classified into no-FAS (no-FAS), FAS only during the periconceptional period (peri-FAS), FAS through the periconceptional period and mid-pregnancy (mid-FAS), and FAS through the periconceptional period, mid-pregnancy, and late-pregnancy (late-FAS) stages, respectively.
Our outcomes of interest included various pregnancy complications (GDM, gestational hypertensive disorders [GHDs], and pre-eclampsia) and birth outcomes (preterm birth, macrosomia, SGA, and LGA). We diagnosed GDM when a 75 g oral glucose tolerance test (OGTT) at 24 to 28 gestational weeks met one of the following three criteria: (1) fasting plasma glucose ≥ 5.1 mmol/L, (2) the 1 h plasma glucose ≥ 10.0 mmol/L, or (3) the 2 h plasma glucose ≥ 8.5 mmol/L [27]. GHDs were defined as new-onset blood pressure ≥ 140/90 mmHg after 20 gestation weeks. Moreover, pre-eclampsia was diagnosed by observing elevated blood pressure and proteinuria after the 20th gestation week [28]. Preterm was defined as delivery occurring before 37 gestational weeks, and macrosomia was interpreted as birth weight ≥ 4000 g. According to the Chinese sex- and gestational week-specific birth weight standards [29], SGA and LGA were defined as birth weight < 10th percentile for gestational age and birth weight > 90th percentile for gestational age, respectively. Since FAS is related to hematological parameters, hemoglobin levels and red blood cell counts at late pregnancy were presented.
2.3. Statistical Analyses
Medians (interquartile range, IQR) were used to present continuous variables, which had skewed distributions according to the Kolmogorov–Smirnov tests (p < 0.05), and frequencies (%) were used to present categorical variables. Their differences across groups of FAS duration were tested by the Kruskal–Wallis test or chi-square test, as appropriate.
Presenting as risk ratios (RRs) and 95% confidence intervals (95% CIs), the associations between FAS duration and pregnancy outcomes were examined using univariable and multivariable two-level mixed-effect log binomial regression models to account for the potential impact of the north and south regions, which had distinct dietary patterns [30]. The multivariable models were adjusted for the mother’s age, pre-pregnancy BMI, parity, ethnicity, conception mode, education level, pre-pregnancy smoking, and alcohol consumption within six months before pregnancy (Table 1). Evidence suggests offspring sex-dependent effects in associations between maternal FAS and offspring development [31]. Thus, offspring sex was additionally adjusted in sensitivity analysis. Since GDM, GHDs, and preeclampsia were diagnosed during mid-pregnancy, FAS after mid-pregnancy cannot logically influence the risk of these outcomes, and thus mid- and late-FAS groups were combined for the relevant analyses.
In order to investigate whether these associations varied by maternal age and pre-pregnancy BMI, the interactions of FAS duration with maternal age and pre-pregnancy BMI for pregnancy outcomes were assessed by introducing their interaction terms in the regression models. Subsequently, subgroup analyses were conducted, stratified by maternal age (≥35 and <35 years) or pre-pregnancy BMI.
Statistical analyses were performed using R software (version 4.0; R Foundation for Statistical Computing, Vienna, Austria) with a two-sided test. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Characteristics of Study Participants
Among 15,694 female participants, 4523 (28.8%), 2854 (18.2%), 921 (5.9%), and 7396 (47.1%) were categorized into no-FAS, peri-FAS, mid-FAS, and late-FAS categories, respectively. Table 1 shows the maternal characteristics for FAS duration groups. Women in the late-FAS group were more likely to be older, multipara, conceive naturally, consume alcohol, and were less likely to be overweight/obese before pregnancy, compared with other participants. Women in the late-FAS group had the highest hemoglobin level at late pregnancy (Table A2).
3.2. Incidence of Pregnancy Outcomes
The incidence of adverse pregnancy outcomes varied significantly by FAS duration (Table 2). The peri-FAS group displayed the lowest incidence of macrosomia (15.2%), while the mid-FAS group exhibited the highest incidence of GDM (28.2%) and the lowest incidences of GHDs (8.9%) and pre-eclampsia (4.0%). Furthermore, the late-FAS group’s participants displayed the lowest incidences of preterm birth (9.4%) and LGA (17.7%), and the no-FAS group reported the highest incidences of SGA (8.1%), compared with the other groups.
3.3. Associations Between FAS Duration and Pregnancy Outcomes
In univariate analyses, FAS during pregnancy displayed lower risks of GHDs, pre-eclampsia, preterm birth, macrosomia, SGA, and LGA; however, mid-FAS was associated with a higher risk of GDM (RR 1.11, 95% CI 1.03, 1.21), compared with the no-FAS group (Table A3). In multivariate analyses with confounder adjustments, the association of mid-FAS with risk of GDM was marginally significant [adjusted risk ratio (aRR) 1.08, 95% CI 0.99, 1.17; p = 0.09], whereas its association with lower risks of GHDs (aRR 0.84, 95% CI 0.74, 0.96) and pre-eclampsia (aRR 0.81, 95% CI 0.67, 0.97) persisted (Table 2). The late-FAS group was significantly associated with lower risks of multiple birth outcomes, including preterm birth (aRR 0.67, 95% CI 0.59, 0.76), SGA (aRR 0.74, 95% CI 0.63, 0.87), and LGA (aRR 0.88, 95% CI 0.79, 0.97) (Table 2). The associations largely remained after additionally adjusting for offspring sex (Table A4).
3.4. Modification Effects of Maternal Age and Pre-Pregnancy BMI
Maternal age modified the associations of FAS duration with preterm birth and macrosomia (Table A5). The protective effects of peri- and late-FAS on preterm birth were more pronounced in women aged < 35 years (p for interaction < 0.01), and on macrosomia were more pronounced in women aged ≥ 35 years (p for interaction = 0.03) [Figure 2, Table A5]. In older participants, mid-FAS was associated with a higher risk of GDM (aRR 1.10, 95% CI 1.01, 1.21), though the interaction effects were insignificant (p for interaction = 0.14) [Figure 2, Table A5].
Among women with pre-pregnancy overweight/obesity, mid-FAS and peri-FAS exhibited an enhanced risk of GDM (aRR 1.34, 95% CI 1.10, 1.63) (Figure 3), as well as higher risks of GHDs (aRR 1.34, 95% CI 1.02, 1.76; p for interaction = 0.01) (Figure 3, Table A5), when compared with the no-FAS group. The associations of FAS duration with GHDs and pre-eclampsia might be modified by pre-pregnancy BMI (Table A5).
4. Discussion
In this prospective multicenter study involving 15,694 Chinese participants, peri-FAS subjects displayed a lower risk of macrosomia, while mid-FAS and late-FAS groups were associated with lower risks of GHDs and pre-eclampsia, as well as preterm birth, macrosomia, SGA, and LGA, compared with the no-FAS group, respectively. Moreover, a few associations were modified by maternal age and pre-pregnancy BMI.
We also found that mid-FAS was associated with lower risks of GHDs and pre-eclampsia. When adjusting for FAS duration, meta-analyses showed that FAS versus no-FAS during pregnancy was associated with reduced risk of pre-eclampsia but not GHDs [32,33]. Similarly, when focusing on FAS duration in pregnancy, two cohort studies from the USA and Canada reported that an extended FAS duration was associated with lower the risks of GHDs and pre-eclampsia [34,35]. Our study’s interaction analysis suggested that peri- or mid-FAS might be associated with lower risks of GHDs and pre-eclampsia among underweight or normal weight women, but not in women with overweight/obesity. Consistently, a previous study also reported the association between peri-FAS and lower risk of pre-eclampsia among women with lower BMI, but not in those with higher BMI [36]. Potentially, the extensive metabolic dysregulation in obese women causes enhanced nutrient requirements compared to lean women [37], thereby attenuating or negating any beneficial effects of increased micronutrient intake [38]. Thus, more research is needed to determine the optimum duration of FAS to counteract the metabolic abnormalities in obese or overweight women.
In our study, mid-FAS was associated with a higher risk of GDM, especially in women with advanced maternal age or with pre-pregnancy overweight/obesity. One Chinese cohort study including 1058 pregnant women collected information on FAS during early pregnancy and reported that FAS was associated with a higher risk of GDM (aOR 1.73) [26]; another Chinese study including 326 pregnancies investigated the association between FAS duration during peri-pregnancy and GDM. FAS duration was classified as no-FAS, 1–60 days, 61–90 days, and 91–365 days. This study reported that women using FAS > 90 days during peri-pregnancy displayed a higher risk of GDM than those using FAS ≤ 60 days (aOR 3.45) [19]. Similarly to our findings, a previous Chinese cohort study that included 1938 pregnancies found that, compared to women with a pre-pregnancy BMI < 25 kg/m^2^ who did not take FAS, women with pre-pregnancy overweight/obesity who took FAS daily in early pregnancy exhibited a higher risk of GDM (aOR 5.63) [39]. Since most significant associations between FAS and increased GDM risk were observed among Chinese populations, the effects of ethnic traits and dietary habits need exploration.
We also assessed the effect of late FAS and found that it exhibited lower risks of multiple interested birth outcomes, including preterm birth, SGA, and LGA. Moreover, two meta-analyses concluded that FAS was associated with lower risks of preterm birth and SGA, if initiated before or after conception [40,41]. However, the data regarding LGA and macrosomia were sparse. One Chinese cohort study found that babies of mothers with peri-FAS were heavier than newborns of mothers with no-FAS; this phenomenon was stronger in newborns with lower birth weight [42]. Consistently, FAS was only positively associated with fetal growth without increasing the risk of LGA [43]. Our late-FAS group exhibited lower risks of preterm birth, SGA, and LGA. The associations between late-FAS and fetal growth-related outcomes could be because of the rapid fetal growth in late pregnancy [44].
Though the underlying mechanisms are ambiguous, multiple, non-mutually exclusive pathways might explain the correlation between FAS and pregnancy outcomes. First, as a key nutrient in the one-carbon metabolism cycle, folate lowers the homocysteine concentration, enriches the placental vascular endothelium [11,12], and reduces the risks of GHDs and pre-eclampsia. Serving as a substrate and cofactor, folate is crucial for multiple biochemical processes, such as nucleic acid and protein synthesis, as well as DNA methylation and repair [1]. Exhibiting indispensable effects on the regulation of placental growth and fetal development [13,14], these processes are intimately linked to birth weight and gestational ages [45,46]. A prolonged FAS duration is associated with an increased risk of GDM, possibly because excessive intake of FA could mask vitamin B12 deficiency [47], which exacerbates insulin resistance and causes GDM [48]. Moreover, elevated circulating unmetabolized folic acid (UMFA) levels might promote natural killer cell dysfunction in humans [49], which might be involved in causing insulin resistance and GDM [50]. Notably, the association between extended FAS and GDM risk was primarily observed in Chinese population [4,18,19], possibly since the MTHFR C677T polymorphism was particularly common in this population [51]. The polymorphism can reduce enzyme activity and alter the metabolic response to high-dose or prolonged FA intake, potentially exacerbating insulin resistance through mechanisms involving altered one-carbon metabolism and UMFA accumulation [8,46,48,52]. In addition, maternal obesity is often linked to elevated levels of hepcidin, an index related to chronic inflammation, which could partly explain the adverse effects of FAS observed among women with higher BMI [53].
Our study extended beyond earlier research by involving multiple pregnancy outcomes, including GDM, GHDs, pre-eclampsia, preterm birth, LGA, SGA, and macrosomia, within a large prospective cohort, and by focusing on FAS duration from periconception to late pregnancy. Additionally, we evaluated the modifying effects of the mother’s advanced age and pre-pregnancy BMI. Our study had a few limitations. First, this study used the data exclusively derived from pregnant women from public referral hospitals. This might have introduced selection bias and affected the data extrapolation. Second, because approximately 75% of our participants were of advanced maternal age and 95% were Han Chinese, the generalizability of our findings to younger pregnant women or other ethnic groups may be limited. Third, our results might be biased because we did not collect the data on the FA dose and multivitamins. This introduces the potential for non-differential exposure misclassification, as individuals within the same FAS duration group may have had varying actual daily intakes. Such misclassification might attenuate the observed associations. Additionally, women with advanced maternal age, adverse pregnancy history, or those under medical supervision may have been advised to continue FAS longer, which could bias the association of extended FAS with risk of GDM. Finally, we lacked data on several potential confounders, such as dietary folate, physical activity, and family medical history. Their absence limits causal interpretation, as residual confounding could bias the associations in either direction.
5. Conclusions
Extending FAS until mid-pregnancy stage was associated with lower risks of GHDs and pre-eclampsia; however, an enhanced risk of GDM was observed in women with advanced maternal age or overweight/obesity. Moreover, FAS until the late-pregnancy stage was associated with lower risks of multiple adverse birth outcomes, including preterm birth, SGA, and LGA. Thus, prolonged FAS during pregnancy might be beneficial; however, women with advanced maternal age or overweight/obesity should be cautious about extending FAS duration. Additional studies focusing on the effects of FA dosage combined with its duration are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Crider K.S. Yang T.P. Berry R.J. Bailey L.B. Folate and DNA methylation: A review of molecular mechanisms and the evidence for folate’s role Adv. Nutr.20123213810.3945/an.111.00099222332098 PMC 3262611 · doi ↗ · pubmed ↗
- 2De-Regil L.M. Peña-Rosas J.P. Fernández-Gaxiola A.C. Rayco-Solon P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects Cochrane Database Syst. Rev.20152015 Cd 00795010.1002/14651858.CD 007950.pub 326662928 PMC 8783750 · doi ↗ · pubmed ↗
- 3Bibbins-Domingo K. Grossman D.C. Curry S.J. Davidson K.W. Epling J.W.Jr. García F.A. Kemper A.R. Krist A.H. Kurth A.E. Landefeld C.S. Folic Acid Supplementation for the Prevention of Neural Tube Defects: US Preventive Services Task Force Recommendation Statement JAMA 201731718318910.1001/jama.2016.1943828097362 · doi ↗ · pubmed ↗
- 4Cheng G. Sha T. Gao X. He Q. Wu X. Tian Q. Yang F. Tang C. Wu X. Xie Q. The Associations between the Duration of Folic Acid Supplementation, Gestational Diabetes Mellitus, and Adverse Birth Outcomes based on a Birth Cohort Int. J. Environ. Res. Public Health 201916451110.3390/ijerph 1622451131731641 PMC 6888242 · doi ↗ · pubmed ↗
- 5Yan J. Liu Y. Cao L. Zheng Y. Li W. Huang G. Association between Duration of Folic Acid Supplementation during Pregnancy and Risk of Postpartum Depression Nutrients 20179120610.3390/nu 911120629099069 PMC 5707678 · doi ↗ · pubmed ↗
- 6Branum A.M. Bailey R. Singer B.J. Dietary supplement use and folate status during pregnancy in the United States J. Nutr.201314348649210.3945/jn.112.16998723365107 PMC 4745881 · doi ↗ · pubmed ↗
- 7Masih S.P. Plumptre L. Ly A. Berger H. Lausman A.Y. Croxford R. Kim Y.I. O’Connor D.L. Pregnant Canadian Women Achieve Recommended Intakes of One-Carbon Nutrients through Prenatal Supplementation but the Supplement Composition, Including Choline, Requires Reconsideration J. Nutr.20151451824183410.3945/jn.115.21130026063067 · doi ↗ · pubmed ↗
- 8Huang Y. He Y. Sun X. He Y. Li Y. Sun C. Maternal high folic acid supplement promotes glucose intolerance and insulin resistance in male mouse offspring fed a high-fat diet Int. J. Mol. Sci.2014156298631310.3390/ijms 1504629824736781 PMC 4013629 · doi ↗ · pubmed ↗