Diet and Mental Health Relationships in Caribbean Populations: A Scoping Review and Evidence Gap Map
Catherine R. Brown, Emily Haynes, Khadija Patel, Christina Howitt, Michael Campbell, Madhuvanti Murphy

TL;DR
This study reviews diet-mental health research in Caribbean populations to identify gaps and guide future studies in culturally diverse contexts.
Contribution
The paper provides the first evidence gap map of diet-mental health relationships in Caribbean populations.
Findings
Most studies focused on food security and depression, with limited use of experimental or qualitative methods.
Few studies used culturally adapted tools, and relationships like seafood intake and autism were frequently explored.
The evidence base is growing but lacks scope, design diversity, and cultural validity.
Abstract
Background/Objectives: Most research linking diet and mental health outcomes is from high-income countries, limiting insight into how these relationships manifest in culturally diverse, vulnerable contexts, such as the Caribbean. This scoping review aims to map existing research on the relationship between aspects of diet and mental health within Caribbean populations, to identify evidence gaps and guide future research. Methods: Eleven databases were searched for studies published between 2000 and 2024 in 33 Caribbean countries which assessed the relationship between diet and mental health outcomes. Duplicate screening and extraction were conducted using Redcap software, and a narrative synthesis and evidence gap map were created. The original protocol was registered with Open Science Framework. Results: Forty-four records were included, nine of which focused on eating disorders…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
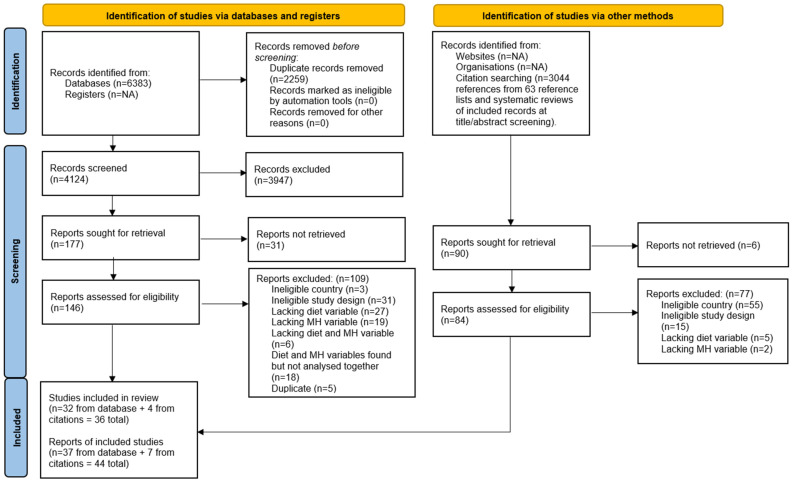 Figure 1
Figure 1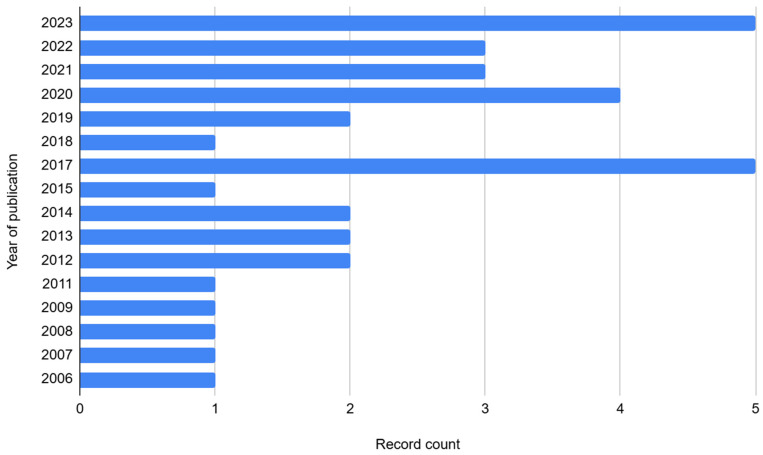 Figure 2
Figure 2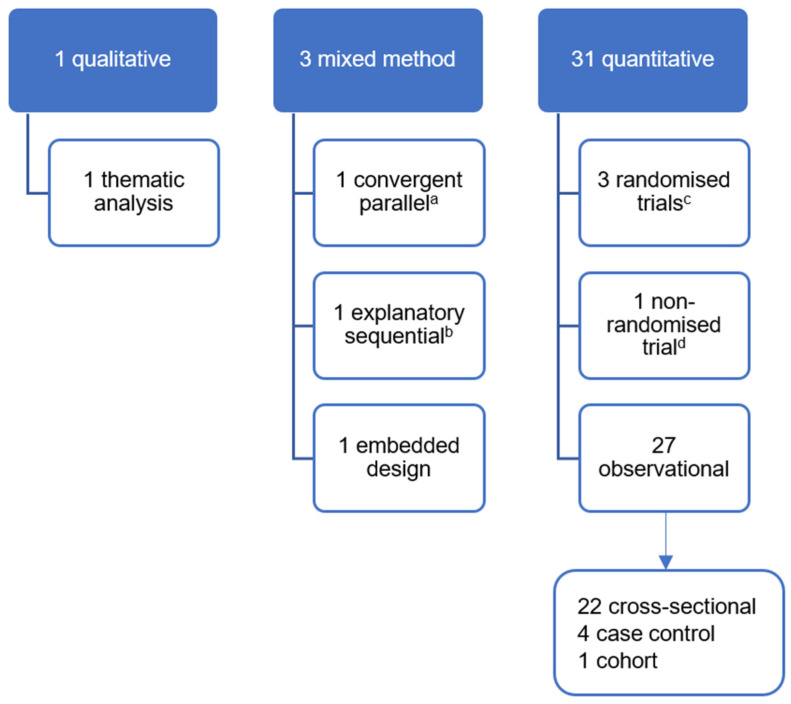 Figure 3
Figure 3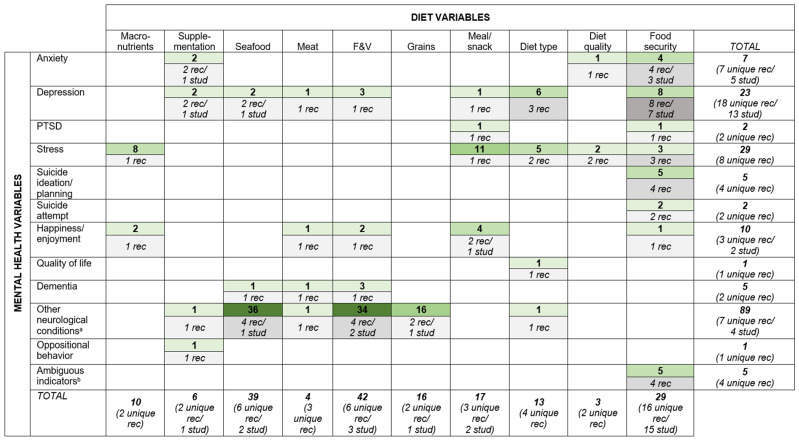 Figure 4
Figure 4| Item | Included | Excluded |
|---|---|---|
| Study design | Experimental or observational studies (qualitative and quantitative), case reports, and conference proceedings (where full-text/data was available). | Editorials. |
| Study setting | Countries/territories in the Caribbean region are included, inclusive of Anguilla, Antigua and Barbuda, Aruba/Bonaire/Curacao, The Bahamas, Barbados, St. Bart’s, Belize, Cayman Islands, Cuba, Dominica, Dominican Republic, St. Eustatius, French Guiana, Grenada, Guadeloupe, Guyana, Haiti, Jamaica, St. Kitts and Nevis, St. Lucia, St. Martin, St. Maarten, Martinique, Montserrat, Puerto Rico, St. Vincent and The Grenadines, Saba, Suriname, Trinidad and Tobago, Turks and Caicos, and the Virgin Islands (US and British). This list is based on that of previous Caribbean-based systematic reviews on social determinants of health [ | Caribbean diaspora. |
| Population | Humans of any age residing in the included study settings. | |
| Intervention | Any intervention; however, studies did not need to implement an intervention to be eligible (i.e., observational designs included). | |
| Diet variable | Any indicator of ‘diet’, including intake of any nutrient, supplement or food, and assessed using any quantitative dietary assessment method (such as food frequency questionnaires, dietary recall, indices of dietary quality, food insecurity scales) or qualitative method (such as interviews or focus groups). | Variables that are not direct measures of food security or diet intake/quality, including: attitudes to/knowledge of diet, water or alcohol intake, and physical/biological proxies of diet/nutritional status (e.g., stunting, wasting, obesity, biological samples of nutrients). |
| Mental health | Any indicator of ‘mental health’ assessed using relevant symptomatic scales or screening tools (e.g., Patient Health Questionnaire-9 Depression scale), diagnostic criteria (e.g., Diagnostic and Statistical Manual of Mental Disorders) or as experienced subjectively by participants (such as in qualitative studies or other means of self-report). This broad inclusion of symptomatology assessment aligns with recommendations to avoid narrowly focusing on diagnostic criteria which could skew potential differing concepts of mental health [ | Proxies for mental health status such as drug or alcohol use. |
| Additional notes: analysis between diet and mental health variables |
Studies reporting on the relationship between at least one diet and one mental health variable. Studies reporting pooled analyses from multiple countries, once at least one Caribbean country is included in the analysis. Eating disorders can be considered a diet indicator and/or a mental health indicator depending on study details. Studies reporting on eating disorders are included but reported separately from diet–mental health relationship records. |
Studies examining diet and mental health variables across generations (i.e., maternal mental health and feeding practices of children and vice versa). With eating disorder studies as the exception, studies that do not report on the relationship between at least one diet variable and one mental health variable. |
| Publication status | Published or unpublished studies released between 1 January 2000 and 11 February 2024 (date of search) in English, Spanish, French, Dutch (i.e., four dominant Caribbean languages). |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Culinary Culture and Tourism · Food Security and Health in Diverse Populations
1. Introduction
Mental health disorders affect over 970 million people worldwide, making them the leading cause of years lived with disability (one in six) and a significant source of societal and economic strain [1]. Reduced economic productivity and direct costs of care due to mental health are expected to cost the world economy USD 6 trillion by 2030 [1].
Determinants of mental health are wide-reaching, yet the impact of diet on mental health outcomes is gaining increased attention [2,3]. Evidence suggests poor diet quality as a modifiable risk factor for mental health conditions, and existing research has investigated its potential impact in two main ways: the impact of specific nutrients (e.g., Vitamin D, omega-3 fatty acids) and the impact of broader dietary patterns (e.g., ultra-processed food consumption, Mediterranean diet) [1,4,5]. For instance, a 2022 review reports the significance of micronutrients and antioxidants in the development of some psychiatric disorders such as Parkinson’s disease, schizophrenia, and depression [6]. Diets high in ultra-processed foods have been associated with systemic (including neural) inflammation and increased risk for depression [7,8]. Research has also highlighted benefits of plant-based diets on symptomatology of depression and dementia [9,10,11]. Likewise, the ketogenic diet has garnered attention for its potential for improving the symptomatology of dementia, bipolar disorder, schizoaffective disorder, and unipolar depression/anxiety [12,13,14]. Further, the ketogenic diet was added to the UK National Institute for Health and Care Excellence Clinical Guidelines for Epilepsies for drug-resistant paediatric epilepsy [15]. A growing number of reviews explore the relationship between diet and mental health—some focusing on specific diets or food groups (e.g., plant-based or ketogenic diets, fruits and vegetables) and/or mental health conditions (e.g., depression, anxiety) [14,16,17,18,19], others taking a broader focus on these variables [20,21,22]. This growing research has led to the conceptualisation of ‘nutritional psychiatry’ as its own field of work [23].
Despite a growing evidence base, gaps remain in examining diverse cultural, dietary, and environmental contexts. Most studies are conducted in high-income, Western countries such as the United States and Europe, limiting generalisability of findings to low-and-middle-income countries (LMIC) and other under-represented countries such as Small Island Developing States (SIDS). Despite most of the world’s population living in LMICs, less than a quarter of the diet–mental health evidence and only 10–20% of experimental studies on the topic are conducted in these populations [24]. SIDS are also underrepresented in research overall, given their smaller populations and capacities [25]. This evidence gap is significant considering that socioeconomic factors, cultural dietary practices, and differing mental health beliefs may play a role in the exploration of diet–mental health relationships [26,27]. This gap is further accentuated by mutual geographic/climatic, environmental, and economic vulnerabilities of these regions, which disproportionately impact their food systems and contribute to high levels of food insecurity [28,29]. Without evidence from a wider range of settings such as these, global dietary recommendations in support of mental health remain limited in their generalisability.
The Caribbean region, comprising a mix of high and LMICs and 16 of the 39 SIDS [30], represents a prime setting for expanding diet–mental health research. Coupled with rising food insecurity levels within its fragile food system [31,32,33], the region has undergone a nutrition transition from traditional, nutrient-dense whole foods to a reliance on imported, low-nutrient, processed foods [34,35]. Further, Caribbean diets consistently fall below recommended targets for key food groups such as fruits, vegetables, legumes, nuts, and whole grains [36]. Increasing reliance on poor quality foods contributes to a rise in metabolic risk factors including elevated blood pressure, blood glucose, blood lipids, and obesity levels and a growing burden of non-communicable diseases (NCDs), such as diabetes, cardiovascular disease, and cancer [37,38]. These conditions not only account for 75% of regional mortality, but also are frequently comorbid with poor mental health [1]. This physical–mental health syndemic is further fuelled by the region’s significant vulnerability to climate change impacts, global economic shifts, and its own unique cultural histories which can shape both food systems and psychosocial stressors [32].
Adding to this backdrop is the growing mental health burden in the Caribbean. While Caribbean-wide data is limited and largely model-based, Global Burden of Disease data indicate that mental health disorders contribute to 5% of DALYs and 16% of YLD in 2019 in the Caribbean [29,39]. This burden is expected to rise at least until 2050, particularly for dementia [40]. Of note, Guyana and Suriname rank 4th and 7th, respectively, among global suicide rates, with 24.8 and 22.3 deaths per 100,000 in 2021 [41]. The World Health Organization’s (WHO) Comprehensive Mental Health Action Plan 2013–2030 stresses the global need for stronger leadership and governance, comprehensive and integrated services, prevention and promotion strategies, and information systems [42]. Given the growing syndemic and comorbidity of physical NCDs and mental health conditions, regional calls to action have been made to include mental health in the heavy NCD focus of countries’ health agendas, and address their underlying causes and impacts [43,44,45,46]. These calls include stronger leadership, policies, and advocacy in support of mental health and strengthening of the region’s limited mental health data and research in the Caribbean.
Understanding the research landscape of the relationship between diet and mental health in the Caribbean is the first step to exploring the role that modifying the population’s diet could have on the region’s mental health burden. Thus, the aim of this review is to map research conducted in the Caribbean that examine the relationship between diet and mental health outcomes to elucidate research gaps and focus future Caribbean-based research on this topic.
2. Methods
This review follows methodological guidance for the conduct of scoping reviews and the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [47,48]. The original protocol was registered with Open Science Framework (https://doi.org/10.17605/OSF.IO/TKJP5).
2.1. Definitions of Variables of Interest
The term ‘diet’ for this review refers to any dietary intake, including nutrient intake, dietary patterns, and dietary quality (inclusive of food security). The term ‘mental health’ is broadly defined by the WHO to include mental disorders, psychosocial disabilities, and other mental states associated with significant distress, impairment in functioning, or risk of self-harm [49]. Further details of these definitions are listed in Table 1. The year 2000 was selected as the starting point for the current study as nutrition research concerning mental health increases substantially after this date [2].
2.2. Eligibility
Eligibility criteria are listed in Table 1 below.
2.3. Search Strategy
Search terms were conceptualised through examination of those used by other reviews on the topic and discussion with colleagues in the field [2,24,52]. The terms were broad to ensure sensitivity, and an example using PubMed syntax is listed in Supplementary Materials Table S1. Eleven databases were searched: Web of Science (via Clarivate), MEDLINE (via PubMed), EMBASE (via Ovid), SciELO, CINAHL (via EBSCO), CUMED (via WHO Virtual Health Library), LILACS (via WHO Virtual Health Library), PAHO and PAHO IRIS (via WHO Virtual Health Library), MedCarib (via WHO Virtual Health Library), PsycINFO (via Ovid), and Global Health (via Ovid). In addition, researchers scanned reference lists of included full-text records and of systematic reviews retrieved during title/abstract screening.
2.4. Record Selection and Data Extraction
Records retrieved from database searching were added to Rayyan reference manager [55]. Authors of inaccessible articles were contacted where contact information was given. Records were reviewed against the eligibility criteria in two steps: (1) Initial screening of titles and abstracts of records → potentially relevant (include) and not relevant (exclude); and (2) Secondary screening of the full-text records identified as potentially relevant in Step 1 → relevant (include) and not relevant (exclude). Key details of eligible records were extracted into REDCap data management software version 15.9.3 [56], including publication information, intervention details (if applicable) and indicators/outcome measures and data collection tools. Screening and data extraction were performed in duplicate by two independent reviewers, and any disagreement or uncertainty was resolved by a third reviewer.
2.5. Data Synthesis
The findings are reported narratively as a descriptive summary of publication details and study characteristics including design, settings, intervention, variables, tools applied, and relationships assessed. An evidence gap map was constructed summarising the distribution of existing evidence. Following scoping review methodology, effect measures and study risk of bias were not assessed.
3. Results
3.1. Summary of Included Records
Of the 6318 database search results and 3044 references screened, 44 records from 36 studies were included (See Figure 1). The references for these 44 records are listed (in the same order as the table) in Supplementary Materials Table S2.
Of the 44 records, 35 examined diet and mental health relationships and 9 were classified as ‘eating disorder’ records. Eating disorders are not an aspect of diet but are considered a behavioural condition that affects dietary intake [58]. Although these studies did not fit the primary aim of this scoping review, their relevance to the topic is acknowledged and so they are briefly and separately presented at the end of this Results section.
The 35 included diet–mental health relationship records were published in 33 peer-reviewed journals, one e-book of studies, and one thesis. Only half were open access. The scope of publications included public health, medical science (broadly), and nutrition (n = 26), with relatively few mental health journals (n = 5). The remaining publications were one unpublished thesis and three environmental journals. Publications spanned from 2006 to 2023, with a gradual increase from one article published per year to five articles per year (See Figure 2).
Studies were conducted in 20 of the 33 Caribbean countries, with most records from Jamaica (n = 12 records), Barbados (n = 7), Dominican Republic, Puerto Rico, and Trinidad (n = 6 each). Others included Cuba and Haiti (n = 4 each); Grenada (n = 3); US Virgin Islands and Bahamas (n = 2 each); and Antigua, Anguilla, Belize, Curacao, Guadeloupe, Martinique, St. Kitts and Nevis, St. Lucia, St. Vincent and the Grenadines, and Suriname (n = 1 each). Overall, 9 of the 35 records reported analyses of pooled data from multiple countries—3 with pooled data from Caribbean countries only [59,60,61] and 6 which also pooled international data [62,63,64,65,66,67].
3.2. Study Details
Study details of the 35 diet–mental health relationship records are listed in Table 2. The sampling frame for most records was the general population/communities (n = 18 records), while others sampled from schools (n = 10), clinics (n = 6), and prison (n = 1). Ten records used child-only samples [67,68,69,70,71,72,73,74,75,76], and some sampled specifically from low-income communities or intentionally recruited participants who were pregnant or reported health issues (e.g., cancer, Parkinson’s disease). Nearly all records used quantitative, observational designs (n = 31) (See Figure 3).
Five records reported on experimental studies [69,79,81,92,93]. One used urban gardens, nutrition, and cooking education to improve food security and subsequently mental and emotional wellbeing among persons living with human immunodeficiency virus in Dominican Republic [81]. Two records from The Jamaican Supplementation and Stimulation Study used milk-based formula supplementation of infants to improve future psychosocial functioning later in life (depression, anxiety, attention deficit, and oppositional behaviour) [92,93]. The final two records implemented a ketogenic diet for (a) adults in Trinidad with various types of cancer to improve their depression and quality of life [79], and (b) a boy in Cuba diagnosed with medication-resistant epilepsy to reduce the frequency and severity of seizure events [69].
Notably, only 10 of 35 records aimed primarily to assess the relationship between diet and mental health, versus 20 records for which this was a secondary aim and 5 where it was not an aim at all. Of these 10 studies, 2 sought to examine the impact of a ketogenic diet intervention (mentioned above) [69,79]; 2 sought to examine the association of dietary patterns and perceived stress among students in Puerto Rico [84,88]; 4 examined the association between food insecurity and (a) suicide ideation/plans/attempt among adolescents across the Caribbean [67,75] and (b) mental health status (including anxiety and depression) in vulnerable communities in Haiti [86] and across several Caribbean countries [59]. One record investigated the association between skipping meals and depression and post-traumatic stress disorder symptomatology among students [66], and another sought to examine the association of annonaceae (e.g., sour soup, sugar apple) consumption and cognitive manifestations in atypical forms of parkinsonism and Parkinson’s disease in Guadeloupe and Martinique [82].
Studies from five records examined diet–mental health relationships during or in response to hazards or disasters—two during the COVID pandemic assessing participants in Barbados, Cuba, Dominican Republic, Haiti, and Puerto Rico [64,65] and three during or after hurricanes affecting the Dominican Republic, Puerto Rico, and US Virgin Islands [85,89,91].
3.3. Variables and Tools
3.3.1. Indicators of Diet
Of the 35 diet–mental health relationship records, 16 examined food security as the ‘diet’ variable and 19 examined diet intake, quality, or type. Diet intake variables included the intake of macronutrients (e.g., fats, protein) (n = 3 records); supplementation (infant formula) (n = 2); seafood (n = 6); meat (n = 2); fruit and/or vegetable (n = 6); grains (n = 1); meals (n = 2); and snacks (n = 2). Overall diet quality (i.e., diet diversity or food group adequacy) (n = 2) and diet type (i.e., ketogenic diet (n = 2); ‘diabetes mellitus specific’ diet (n = 1); and ‘Western’ diet (n = 1)) (n = 4) were also examined. Most records used food frequency questionnaires to collect dietary data (n = 14); one used 24 h recall and food diary, and another used qualitative interviews. The three remaining experimental records did not explicitly explain their diet assessment procedure [81,92,93].
Food security was most commonly measured using surveys, while two records used qualitative interviews. However, only four records used standardised food security surveys, namely the Household Hunger Scale, Household Food Insecurity Access Scale, Latin American and Caribbean Food Security Scale, and the Food Insecurity Experience Scale Survey Module for Individuals. Others used generalised multi-component surveys, often with only one question assessing food security (n = 10).
Few records explicitly examined processed foods (e.g., cakes, dumplings, soft drinks, Vienna sausages, added sugars) within their diet variables [72,74,84,88,90], and nine records specifically mentioned the production or consumption of local foods. These local foods included annonaceae in Guadeloupe and Martinique [82] and various local fruits and vegetables (e.g., ackee, avocado) in Jamaica [71,72,73,74]. Two examined local food production (a food security intervention) [81] and local food consumption [89] in Dominican Republic. Two others examined individual agricultural assets (a measure of food security) in Haiti [80,86]. All other records assessed diet without specification of local/traditional foods.
3.3.2. Indicators of Mental Health
Depression diagnosis or symptomatology was the most frequently (and widely) examined variable (n = 17 records), followed by perceived stress (n = 8) and anxiety diagnosis/symptomatology (n = 7). Others included suicide ideation/planning (n = 5 records), suicide attempt (n = 2), dementia diagnosis/symptomatology (n = 2), post-traumatic stress disorder symptomatology (n = 2), happiness/enjoyment (n = 2), overall quality of life (includes mental health components) (n = 1), and oppositional behaviour symptomatology (n = 1). Seven records reported on indicators of neurological conditions other than dementia: parkinsonism severity (n = 1), epileptic seizures (n = 1), autism diagnosis (n = 4), and attention deficit behaviours (n = 1). The remaining five records used ambiguous indicators: scores for ‘mental and emotional wellbeing’ (n = 1), ‘mental health symptoms’ (n = 1), ‘negative experience index’ (n = 1), ‘positive experience index’ (n = 2), and having a child at home with a mental disability (n = 1).
A wider variety of tools were used to measure mental health variables than to measure diet variables; 46 unique tools were used for measuring the 16 mental health variables, as shown in Table 3. Among all mental health variables, depression was measured by the widest variety of tools—14 different tools (1 diagnostic test and 13 measures designed to assess symptomatology) across 17 records. On the other hand, the WHO Global School-Based Student Health Survey was used in all five records examining suicidal thoughts and behaviours [67,68,70,75,76]. Some data collection tools assessed multiple different mental health variables in their studies: Geriatric Mental State Exam [94]; Child Vulnerability Survey [60]; WHO Global School-Based Student Health Survey [95]; Behaviour and Activities Checklist [92]; Negative Experience Index [59]; researchers’ own survey; and qualitative interview.
3.3.3. Cultural Adaptation of Tools
Although an array of tools was used to collect data on diet and mental health outcomes, only 10 explicitly noted that the data collection tool was culturally adapted to their Caribbean setting. Three of these were qualitative interview guides are assumed to be designed for defined populations of the studies. Five records culturally adapted their tool for dietary intake data collection by adding culturally relevant food groups or questions and piloting [60,79,88], or researchers used a tool previously created for or adapted to the Caribbean setting (e.g., Latin American and Caribbean Food Security Scale) [61,82]. Regarding mental health tools, four records culturally adapted their tool by adding questions and piloting [60,79] or used a tool previously created for or adapted to the Caribbean setting [80,86].
3.4. Relationships Examined
Below, Table 4 details the relationships examined and tools used in each of the 35 included records. Figure 4 further illustrates the distribution across variables of these 179diet–mental health relationships.
Fruit and vegetable intake (n = 42 relationships), seafood intake (n = 39), and food security (n = 29) were the most frequently examined diet variables. However, the majority of the seafood intake variables are from the Jamaican Autism Study examining autism diagnosis [71,72,73,74]. ‘Other neurological conditions’ was the most frequently examined mental health variable (n = 89 relationships). However, nearly all are also from the Jamaican Autism Study examining the association between autism diagnosis and the intake of fruits and vegetables, seafood, grains, and meat [71,72,73,74]. Perceived stress (n = 29 relationships) and depression (n = 23) were also frequently reported yet spread across a larger number of unique records/studies (i.e., more widely examined). Food security was the most widely examined diet variable (n = 29 relationships examined in 16 records from 15 studies), and depression was the most widely examined mental health variable (n = 23 relationships examined in 18 records from 13 studies).
With respect to relationships, the most frequently examined relationships were seafood intake and other neurological conditions (n = 36 relationships in four records from one study); fruit and vegetable intake and other neurological conditions (n = 34 relationships in four records from two studies); and grain intake and other neurological conditions (n = 16 relationships in two records from one study)—all from the same Jamaican Autism Study. Apart from these, meal/snack intake and perceived stress (n = 11 relationships in one record); macronutrient intake and perceived stress (n = 8 relationships in one record); and food security and depression (n = 8 relationships in eight records from seven studies) were the most frequently examined relationships, the latter also being the most widely examined relationship of all relationships found.
3.5. Eating Disorders
Nine peer-reviewed, mostly cross-sectional records (2002–2011) examined eating disorders; five were open access. They included one pooled regional analysis on dieting behaviours and their correlates across nine countries [96]; five reports of school-based surveys on bulimic disorders, eating attitudes, and body image perceptions in Barbados, Trinidad, and Puerto Rico [97,98,99,100,101]; two medical-record reviews of anorexia and other eating disorder diagnoses in Curacao and Jamaica [102,103]; and one mixed-methods study exploring cultural influences on anorexia diagnoses in Curacao [104]. Together, they assessed incidence, prevalence, correlates, and contextual factors related to eating disorders in adolescents and adults across 12 Caribbean countries.
Except the Jamaica and Curacao studies which were secondary data analyses, the data collection tools included the following:
- To screen for anorexia and/or bulimia: Researchers own short surveys (n = 4 records); Eating Attitudes Test-26 [105] (n = 5); Bulimia Investigatory Test Edinburgh (BITE) [106] (n = 2); Bulimia Test-Revised (BULIT-R) [107] (n = 2); Eating Disorders Inventory (EDI) [108] (n = 1); and the Questionnaire for Eating and Weight problems-revised [109] (n = 1);
- To diagnose bulimia: Diagnostic and Statistical Manual of Mental Disorders, 3rd edition, revised Bulimia Diagnostic Interview [110] (n = 1);
- To screen for any eating disorder: Drive-for-Thinness subscale of the Eating Disorder Inventory-2 [111] (n = 1).
Except for three studies of university students [97,100,101], authors reported a relatively low prevalence of potential eating disorders in the context of the protective factors of a “still traditional” culture [98] of healthy body size preferences and eating habits. Authors referred to the growing influence of Western ideals of thinness/beauty as a contributing factor to eating disorders, while one hypothesised that the influence may not be Western-specific per se but rather related to the process of any society’s complex socio-cultural development [104].
4. Discussion
4.1. Summary Findings and Evidence Gaps
Thirty-five records examined relationships between diet and mental health in the Caribbean between 2000 and 2024. Despite relatively limited human and infrastructural capacities, an increasing number of studies were conducted in a wide range of Caribbean countries (20 of 33 searched). While this might seem to reflect growing regional interest in the field, the low number of studies that examine this relationship as a primary research aim suggests the Caribbean to be at an early, exploratory stage of examination.
With respect to study design, the common use of cross-sectional design limits speculation on the direction of reported associations. Though five interventions were found, the collective strength of evidence is limited due to relatively small sample sizes and lack of control groups or randomisation. The low number of qualitative studies indicates a weak understanding of sociocultural beliefs about the diet–mental health relationship, including what might shape the relationship or its focus in academic research. Overall, studies were mostly epidemiological; there were no biological studies of mechanisms of action (for example, gut or neural inflammation, gut microbiome, or hypothalamic–pituitary–adrenal axis) which could also deepen the regional evidence base on nutritional psychiatry. Finally, with respect to eating disorders, the evidence spans only up to 2011, deeming their findings possibly less relevant considering that Caribbean countries are vulnerable to rapid globalisation and it is argued that prevalence of eating attitudes and disorders may change over time [98].
Although a variety of diet and mental health variables were examined, the Jamaican Autism Study [71,72,73,74] skews the image of a strong Caribbean focus on autism when in fact its high count of relationships comes from this single study. It is unsurprising that perceived stress and depression were the most frequently and widely examined mental health variables, given the ubiquity of stress and its implications for both physical and mental health, and that depression is among the most common mental health disorders globally [112]. Yet two major mental health disorders were not reported - bipolar and schizoaffective disorders. While less prevalent than anxiety or depression, this is a significant evidence gap given their severity of symptoms, comparative difficulty in achieving remission, and the emerging evidence of effective nutritional interventions that may reduce their symptoms and burden of disease [17,113].
The most frequently and widely reported diet variables (fruits and vegetables, seafood and food security) are also unsurprising given the commonly purported protective role of fruits and vegetables in promoting adequate health [18,114], the cultural significance and abundance of seafood in Caribbean diets, and the rise in food insecurity in the region [31]. However, the low number of records examining processed foods and local foods specifically is important considering the Caribbean’s heavy reliance on processed food imports, and the vital role local foods could play in improving food sovereignty, food security and NCD risk profiles in the Caribbean [32,34,35,115]. Indigenous foods of the region have declined in availability since colonialism, but traditional plant-based foods, such as the West Indian cherry, mango, avocado, aloe, cassava, and breadfruit, not only have nutritional benefits, but also their production could improve food sovereignty and climate resilience of small island food systems [116,117].
Though not problematic to see diversity in variables examined across studies, the variation in data collection tools used limits both the comparability between settings and, in some cases, the validity of findings. Variation could obscure observed associations when comparing diverse contexts [59]. For example, the variability of tools used to assess food security is relevant considering that its impact on mental health is not only from biological effects of poor nutrition but also because of the stress caused by being food insecure, with accompanying emotions and behaviours which can be culturally bound [21,118]. Suicide was the only variable examined by the same standardised tool, namely the WHO Global School Based Survey. However, validity of findings is questionable as the survey often used a single yes/no question for assessment (e.g., “During the past 12 months, did you ever seriously consider attempting suicide?”) [68]. This inconsistency in tools is perhaps driven by the relative lack of measures (particularly mental health measures) validated for use in the Caribbean, which raises risk for error in interpretation of both research and clinical findings [119,120]. The emerging field of global mental health emphasises the significance of cultural variation in conceptualisations of mental health, which can influence both the interpretation and measurement of mental health constructs and questions the applicability of standardised assessment tools across diverse settings [26,121]. The same can be said for diet; measuring dietary intake with standard tools such as food frequency questionnaires is challenged by cultural differences in food preferences and varying access to foods, which may not be fully captured. The omission of culturally specific foods can limit the accuracy of dietary assessment, particularly amongst underrepresented groups, potentially contributing to gaps in understanding diet-related health outcomes [27].
4.2. Future Research Focus
A more targeted systematic review to follow this scoping exercise is recommended to examine this existing data. Potential areas of focus can include the most widely reported relationships—‘food security and depression’, and ‘food security and suicide ideation/planning/attempt’. Additionally, risk of bias assessments of systematic reviews will elucidate the strength of existing evidence.
Secondly, conducting studies with the primary aim of examining the relationship between diet and mental health could deepen understanding of nutritional psychiatry in the region. Study designs that promote enquiry beyond the cross-sectional observational study are warranted. Qualitative and mixed-methods studies can provide insight into why research in this area might be lacking and what cultural beliefs and understandings exist about the relationship. Hoek et al., for example, found sociocultural factors to be associated with the incidence of anorexia nervosa in Curacao, and they call for a deeper understanding to support their explanatory hypotheses on how settings influence the development of eating disorders [102]. Intervention studies would also benefit the regional evidence base of nutritional psychiatry, perhaps focusing on plant-based and ketogenic diets and including more severe mental health conditions given the growing amount of evidence in support of these in other settings [9,12,14]. Interventions promoting fruit and vegetable intake might be particularly relevant for Caribbean populations given existing low intake and potential benefit for both physical and mental health [36]. Further, understanding contextual factors such as cultural food preferences and local food availability and accessibility could complement intervention work. Researchers should also consider examining processed food and local food consumption and use dietary diversity as a proxy for nutrient adequacy, given their evidenced impact on mental health in other countries and considering the Caribbean’s narrowing local foodscape and dependency on (often processed) food imports [117,122]. Likewise, researchers should facilitate ethical inclusion of people with severe mental illness, such as those with bipolar disorder and schizophrenia, to increase their representation in needed research [123]. Though, researchers must acknowledge the threat of Neyman bias arising from the potential of persons with severe mental health disproportionately refusing to participate in or withdrawing from studies, and also the difficulty in recruiting from other hard-to-reach groups (i.e., low-income or rural dwellers). Finally, social desirability bias is also at play in any self-report of diet, where participants might erroneously report healthier foods than those that are truly consumed.
With respect to tools, researchers are encouraged to use culturally appropriate data collection tools or conduct validation studies in Caribbean settings to prevent the misappropriation of WEIRD-developed tools (‘Western, Educated, Industrialised, Rich and Democratic’ contexts) [124]. For instance, the Beck Depression Inventory II has been validated in Jamaican university students [125]; Perceived Stress Scale and Brief Resilient Coping Scale were validated in health professional students across four Caribbean countries [124]; and EQ-5D-5L for self-reported health was validated in adults in Barbados and Jamaicas [126]. Yet caution must be taken in applying these tools across all ages and countries given the specificity of study samples. Also, any cultural adaptation to standardised tools must also appreciate the ‘tailor locally, retain globally’ principle in measurement tool adaptation. While culturally adapting standardised tools is essential, the process must be balanced to preserve enough of the original structure to allow for meaningful cross-country comparisons [127]. A recent example is the adaptation and pilot of the INTAKE24 dietary intake data collection tool, which was originally developed for the United Kingdom context. Researchers from the Global Community Food and Health Project adapted the diet recall tool for application in St. Vincent and the Grenadines, adding Caribbean dishes and local foods to ensure cultural applicability and validity (ongoing study; manuscript in review) [128]. Food frequency questionnaires can also be adapted to include context-specific foods and use more branching logic with open-answered questions to capture these foods in a systematic way [27].
Finally, researchers are encouraged to publish in more open-source platforms and mental health-focused publications to promote further awareness and advocacy in mental health arenas where, perhaps, knowledge on the potential impact of diet on mental health may be less acknowledged.
4.3. Strengths and Limitations
To our knowledge, this scoping review is the first to attempt to map research on diet and mental health relationships in the Caribbean. It provides a broad snapshot of existing research to guide focused systematic reviews and primary studies on the topic. Its broad search strategy encompassing eleven databases and the inclusion of review articles during screening maximised sensitivity to capture as many relevant studies as possible. However, as expected within scoping review work, researchers were challenged by deciding on eligibility criteria for the two variables. While definitions of mental health were kept broad, researchers were forced to draw a line between what constitutes ‘mental health’ versus ‘overall brain health’, especially considering the physiological connection between physical and mental health and the shared purported pathophysiology of diet’s impact on both, through oxidative stress and systemic inflammation, for example [3]. It is acknowledged that broader definitions of variables might identify further studies.
5. Conclusions
Research examining diet and mental health relationships is steadily increasing in Caribbean contexts. However, research is limited in study design (mostly cross-sectional); is thinly spread across most variables; and often uses data collection tools that may not be culturally appropriate. Targeted systematic reviews of the identified diet and mental health variables are required to better understand the extent of existing evidence in the region. Experimental and qualitative studies that primarily aim to explore the impact of diet on mental health outcomes and related beliefs of such, using culturally appropriate, data collection tools, are warranted. Diet and mental health are cultural phenomena of populations and future examinations should be performed with a cultural lens to elucidate more on if and how culture interacts with findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization World Mental Health Report: Transforming Mental Health for All World Health Organization Geneva, Switzerland 2022
- 2Sparling T.M. Cheng B. Deeney M. Santoso M.V. Pfeiffer E. Emerson J.A. Amadi F.M. Mitu K. Corvalan C. Verdeli H. Global Mental Health and Nutrition: Moving Toward a Convergent Research Agenda Front. Public Health 2021972229010.3389/fpubh.2021.72229034722437 PMC 8548935 · doi ↗ · pubmed ↗
- 3Kaplan B.J. Rucklidge J.J. Romijn A. Mc Leod K. The Emerging Field of Nutritional Mental Health: Inflammation, the Microbiome, Oxidative Stress, and Mitochondrial Function Clin. Psychol. Sci.2015396498010.1177/2167702614555413 · doi ↗
- 4Eliby D. Simpson C.A. Lawrence A.S. Schwartz O.S. Haslam N. Simmons J.G. Associations between Diet Quality and Anxiety and Depressive Disorders: A Systematic Review J. Affect. Disord. Rep.20231410062910.1016/j.jadr.2023.100629 · doi ↗
- 5Devranis P. VassilopoulouΕ. Tsironis V. Sotiriadis P.M. Chourdakis M. Aivaliotis M. Tsolaki M. Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review Life 20231317310.3390/life 1301017336676122 PMC 9866105 · doi ↗ · pubmed ↗
- 6Grajek M. Krupa-Kotara K. Białek-Dratwa A. Sobczyk K. Grot M. Kowalski O. Staśkiewicz W. Nutrition and Mental Health: A Review of Current Knowledge about the Impact of Diet on Mental Health Front. Nutr.2022994399810.3389/fnut.2022.94399836071944 PMC 9441951 · doi ↗ · pubmed ↗
- 7Lane M.M. Davis J.A. Beattie S. Gómez-Donoso C. Loughman A. O’Neil A. Jacka F. Berk M. Page R. Marx W. Ultraprocessed Food and Chronic Noncommunicable Diseases: A Systematic Review and Meta-Analysis of 43 Observational Studies Obes. Rev.202122 e 1314610.1111/obr.1314633167080 · doi ↗ · pubmed ↗
- 8Ejtahed H.-S. Mardi P. Hejrani B. Mahdavi F.S. Ghoreshi B. Gohari K. Heidari-Beni M. Qorbani M. Association between Junk Food Consumption and Mental Health Problems in Adults: A Systematic Review and Meta-Analysis BMC Psychiatry 20242443810.1186/s 12888-024-05889-838867156 PMC 11167869 · doi ↗ · pubmed ↗