Nutritional Status, Body Composition and Growth in Paediatric-Onset Ulcerative Colitis: A Systematic Review
Chen Sarbagili-Shabat, Floor Timmer, Konstantina Morogianni, Ralph de Vries, Tim de Meij, Nikki van der Kruk, Lana Verstoep, Nicolette Wierdsma, Johan Van Limbergen

TL;DR
This review explores how ulcerative colitis affects growth and nutrition in children and adolescents, highlighting the need for better research.
Contribution
The study systematically reviews UC-specific data on growth, nutrition, and body composition in pediatric patients, identifying gaps in current research.
Findings
Growth failure prevalence in UC patients ranged from 7% to 36%, with weight deficits more common than height deficits.
Undernutrition affected up to 25% of UC patients, but findings were variable across studies.
Only five small studies assessed body composition, reporting inconsistent results on lean body mass.
Abstract
Background: Growth impairment and poor nutritional status are recognized complications of pediatric inflammatory bowel disease (IBD), yet data specific to ulcerative colitis (UC) are limited. This systematic review aims to provide an overview of current knowledge on growth, nutritional status, and body composition in children and adolescents with UC. Methods: A systematic literature search was performed up to August 2025. Studies including patients aged 5–22 years with confirmed UC were reviewed. Results related to growth, nutritional status, and body composition were narratively synthesized to summarize findings. Results: Fifteen studies with 1575 patients with UC met inclusion criteria, comprising 5 prospective, 5 cross-sectional, and 5 retrospective designs. Although the included studies were conducted in broader IBD cohorts, only UC-specific outcomes were reported. The data were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
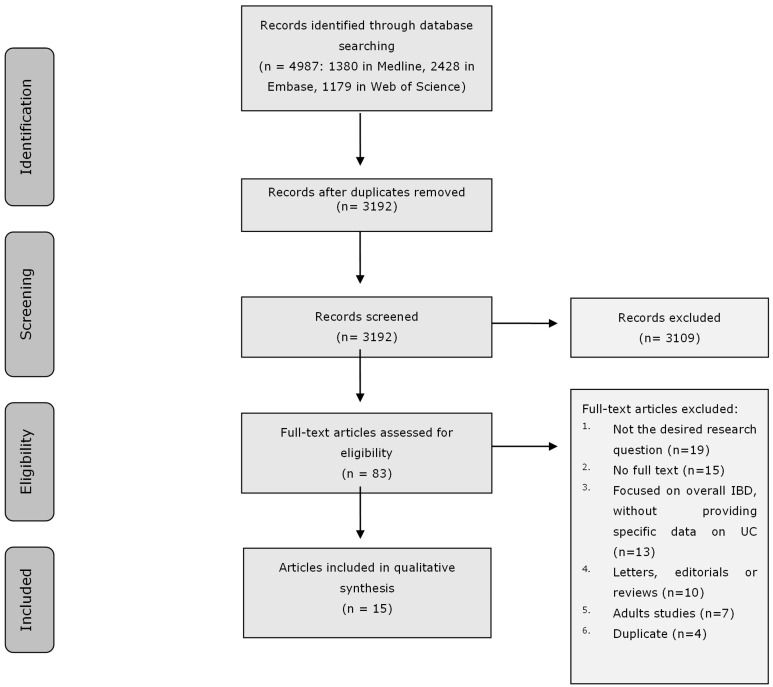 Figure 1
Figure 1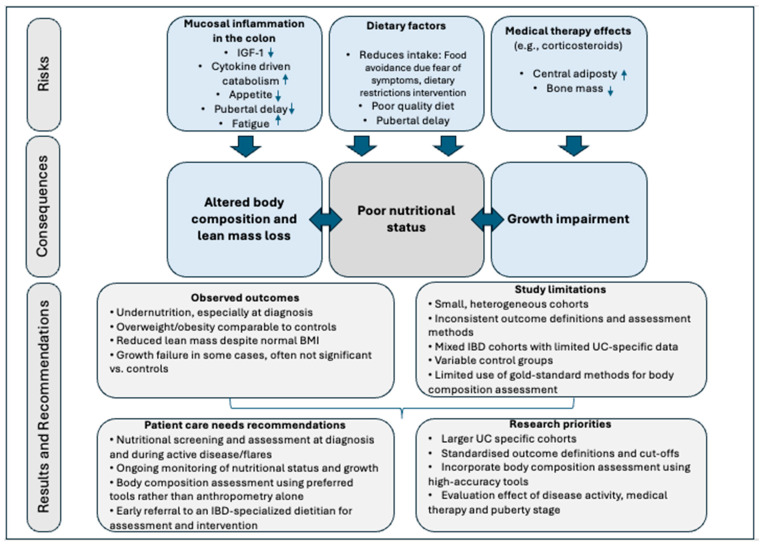 Figure 2
Figure 2- —Nestlé Health Sciences for an investigator-initiated study into nutritional status in colonic IBD
- —Health Holland TKI grant in partnership with Nestlé Health Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Infant Nutrition and Health · Pregnancy and Medication Impact
1. Introduction
Growth impairment and poor nutritional status are prevalent in children with inflammatory bowel diseases (IBD), particularly at diagnosis and during active phases, but can also exist during remission phase [1]. Poor nutritional status reflects an underlying nutritional imbalance and can result in growth impairment, undernutrition, overnutrition, obesity, and altered body composition [2]. Studies have indicated that poor nutritional status reduces quality of life, including a decline in physical performance and social functioning, and is associated with impaired clinical outcomes and an increased need for surgery in patients with IBD [3,4,5]. Although Crohn’s disease (CD) and ulcerative colitis (UC) share some overlapping clinical characteristics, key differences in pathophysiology lead to distinct approaches in disease management [6,7]. These differences are likely to influence nutritional status and growth patterns in distinct ways across conditions. Despite this, many studies group CD and UC together under the umbrella of IBD, which may mask UC-specific variations. Therefore, focusing exclusively on UC allows for a more precise understanding of growth impairment and nutritional features and challenges unique to this population. Two systematic reviews have examined body composition in children with IBD. In one review, reduced lean mass was reported in children with IBD; however, UC represented a minority of participants [8]. A more recent systematic review across chronic inflammatory diseases in children predominantly reported findings in CD, with scarce data for ulcerative colitis [9].
The pathogenesis of UC is thought to result from a dysregulated immune response toward microbial antigens in genetically susceptible individuals exposed to environmental triggers, including dietary factors [10]. UC is characterised by gut microbial dysbiosis, with reduced short-chain fatty acid–producing taxa [11,12] and, in some studies, an increased abundance of potential pathobionts such as hydrogen sulfide–reducing bacteria [12]. Paediatric UC is typically more extensive and severe than adult-onset disease [13]. Assessment of UC in children requires a multidisciplinary approach, incorporating clinical evaluation, endoscopy, imaging, and histological assessment, with disease severity guiding therapeutic decision-making ranging from aminosalicylates and corticosteroids to biologic and immunomodulatory therapies [6,14]. Multiple factors, such as the inflammatory burden, clinical symptoms, changes in dietary habits, physical activity levels, and medical treatments, can influence growth and nutritional status in children and adolescents with UC [15]. Recent nutritional consensus guidelines for IBD emphasize the importance of a thorough nutritional assessment using various tools, including body composition analysis, to accurately evaluate nutritional status. Although linear growth is routinely monitored in clinical practice for patients with IBD, comprehensive evaluation of nutritional status remains challenging due to budget constraints, the need for specialized expertise, and the time required [16]. Relying solely on anthropometric measurements such as body mass index (BMI) may lead to misclassification: overweight or obese patients may appear well-nourished despite being malnourished [4,5]. Furthermore, these measurements alone cannot accurately reflect body composition [17,18,19]. Therefore, the aim of this study is to perform a systematic review to provide an overview of current knowledge on growth, nutritional status, and body composition in children and adolescents with UC.
2. Materials and Methods
2.1. Systematic Literature Review
The conduct and reporting of this review were in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [20]. This study was submitted to the International Prospective Register of Systematic Review—PROSPERO (CRD420251072395) [21].
2.2. Search Strategy
To identify the relevant publications, we conducted systematic searches in the bibliographic databases Ovid Medline, Embase.com and Web of Science (Core Collection) covering all records indexed in each database from their start dates up to 12 August 2025. The following terms were used (including synonyms and closely related words) as index terms or free-text words: “Ulcerative Colitis”, “Growth”, “Nutritional Status”, “Malnutrition”, “Body composition”, “Adolescents”, “Children”. The references of the identified articles were searched for relevant publications. Duplicate articles were excluded by a medical information specialist using Endnote X21.0.1 (Clarivate^TM^, London, UK), following the Amsterdam Efficient Deduplication (AED) method, a stepwise approach based on combinations of bibliographic fields to efficiently identify and remove duplicates [22], and the Bramer method, which applies systematic multi-field matching to remove duplicates [23]. The full search strategies for all databases can be found in Supplementary Material (Supplementary Table S1). The main outcomes were related to growth, nutritional status, and body composition, as defined in Table 1.
2.3. Selection Process
Two reviewers (CSS and FT) independently screened all potentially relevant titles and abstracts for eligibility. Differences in judgement were resolved through discussion. Studies were included if they met the following criteria: involved children or adolescents aged 5–22 years with an established diagnosis of UC. Although paediatric care typically ends earlier, studies reporting outcomes beyond adolescence were included when disease onset occurred during childhood or adolescence, in order to capture longitudinal growth and nutritional outcomes. Studies were excluded if they included patients with IBD without separate UC data, involved animal models or in vitro research, or were of certain publication types such as editorials, letters, legal cases, interviews, commentaries, or conference abstracts lacking full data. If necessary, the full-text article was checked for the eligibility criteria.
2.4. Data Assessment
The full text of the selected articles was obtained for further review. Two reviewers (CSS and FT) independently evaluated the methodological quality of the full-text papers using used the JBI appraisal tools [27]. Any differences between the reviewers were resolved by discussion.
2.5. Data Synthesis
Given the anticipated heterogeneity in outcomes (including indicators of overall nutritional status, body composition, and growth), as well as the variability in assessment methods and the relatively small number of studies available for each, we used a qualitative synthesis to present the results. Study characteristics, relevant outcomes, and main results were extracted from the included studies and narratively synthesised to provide broader insights into growth, nutritional status, and body composition in children and adolescents with UC.
3. Results
3.1. Search Results
The literature search generated a total of 4987 references. After removing duplicates of references that were selected from more than one database, 3192 references remained. The flow chart of the search and selection process is presented in Figure 1. A total of fifteen studies were included: twelve provided data on growth impairment, eight on malnutrition, and five on body composition.
3.2. Study and Patient Characteristics
The studies were equally distributed across designs, with 5 prospective, 5 cross-sectional, and 5 retrospective studies (Table 2). The majority of the prospective studies had follow-up periods extending up to one year. The included studies focused on patients with IBD or other gastrointestinal disorders, analyzing UC patients as a subgroup. In total, the included studies reported on 1575 children and adolescents with UC. Sample sizes varied from 12 to 676 participants/patients. The mean or median age across studies varied between 9 and 14 years, with one study reporting a mean age of 21.4 years representing the final measurement [28]. When specified/where reported, the disease duration ranged from less than one year to 6.3 years [28,29,30,31]. Among the six studies that reported disease duration, 63–66% of the UC patients were in remission or had mild active disease [30,31,32,33,34,35]. While most studies did not provide detailed data on medical treatment, three studies reported that patients were treatment-naïve at baseline [33,34,36]. Additionally, in four other studies, aminosalicylates were the most frequently used therapy [29,30,35,37]. Table 2 summarizes only the results reported for patients with UC. Most of the included studies (12/15) did not perform separate analyses for each study outcome or assess statistical significance specifically for patients with UC.
3.3. Methodology Assessment of the Outcomes
The included studies in this systematic review employed a variety of standardized methods and criteria to assess growth, nutritional status, and body composition in pediatric UC populations. Growth was predominantly assessed using height and weight converted to z-scores or percentiles according to established reference populations, most commonly the WHO growth standards or national growth references. Definitions of growth impairment varied across studies but typically included height or weight z-scores below specific thresholds (e.g., <−1 or <−1.64) [29,33,34,36,39,42], while several studies used a threshold of −2 standard deviations (SD) to classify growth failure as stunting or short stature [28,30,31,32,33,34,36,37,38,40]. The use of a −2 SD cutoff likely led to an underestimation of growth impairment. Although assessing changes over time is crucial, only a minority of studies incorporated dynamic measures such as height or weight velocity to capture growth patterns over time [28,29]. Nutritional status was primarily evaluated through BMI z-scores to categorize underweight, overweight, or obesity, with cutoffs generally aligned with WHO or national standards [30,31,33,34,37,40].
Body composition was assessed exclusively using indirect, non-invasive methods, mainly bioelectrical impedance analysis (BIA) and anthropometric measures such as mid-upper arm circumference (MUAC), triceps and subscapular skinfold thickness, and handgrip strength [30,31,34,35,41]. Reported parameters included fat mass, fat-free mass, lean body mass, body fat percentage, and phase angle. None of the included studies used dual-energy X-ray absorptiometry (DXA), which is considered the gold-standard method [1], thereby reducing accuracy and sensitivity in detecting subtle changes in muscle and fat mass.
3.4. Systematic Evaluation of Growth and Nutritional Status
Across included studies assessing growth, growth failure among pediatric UC patients exhibited variability, with prevalence estimates ranging from 7 to 36%, depending on the definition applied [33,36,39,42]. Zhou et al. reported significantly lower weight percentiles at diagnosis, with growth failure in 30% of boys and 36% of girls, although height did not differ compared with controls. Rates of stunting ranged from 0 to 19% [28,32,36,37,39,40]. The highest prevalence of stunting was reported in a small cohort in Bahrain (19% of 41 UC patients), but no statistical comparison to controls was provided. Weight deficits at diagnosis were commonly reported, with several cohorts identifying a substantial proportion of patients exhibiting weight z-scores below normal thresholds [34,36,38]. In contrast, height impairments were less consistently observed; multiple studies [30,31,35,36,37,38,39] reported no significant differences in height percentiles or height z-scores between patients with UC and healthy controls. Final adult height outcomes were generally comparable to healthy populations, although some evidence suggested that males diagnosed prior to puberty may experience reduced adult stature [28,39].
Malnutrition, including undernutrition, was evaluated with prevalence ranging from 0% to 25%. Two studies, one in Poland and one in the United Kingdom (UK), reported significantly lower BMI z-scores than in the control/reference group despite relatively low rates of growth failure [33]. A study in Saudi Arabia demonstrated a significantly greater prevalence of undernutrition versus the national growth reference, although the difference in growth failure specifically was not significant [40]. A Croatian cohort of newly diagnosed children reported the highest prevalence of undernutrition in UC (25%) [34]. Information on disease severity was lacking in 3 out of 8 studies, while in the other studies, most patients were in remission. In the remaining studies, although most patients were in remission, data comparing active versus inactive disease were not provided, which may partly explain the variability in the results. Overnutrition and obesity were also reported across four cohorts, with three studies showing no significant differences in prevalence compared with controls [31,33,34]. However, overweight prevalence in patients with UC was significantly higher than expected in the Saudi cohort versus reference standards [40].
3.5. Systematic Evaluation of Body Composition
Body composition was evaluated in small pediatric or adolescent UC cohorts, with sample sizes ranging from 12 to 40 patients per study [30,31,34,35,41]. Results demonstrated heterogeneity in body composition outcomes, including lean and fat mass parameters among patients with UC. Two studies identified significantly reduced lean mass or phase angle in patients with UC compared with healthy controls [34,35], even in the presence of normal height and weight. Sila et al. specifically reported significantly lower lean body mass. In contrast, Pawłowska-Seredyńska et al. [33] found lean body mass deficiency only in 3% of patients with UC and another study reported no significant difference in lean body mass z-scores versus controls [31].
3.6. Quality Assessment
A summary of the methodological quality assessment across included studies is presented in Table 3, with detailed study-level assessments provided in Supplementary Tables S2 and S3. All five cross-sectional studies were found to have a moderate risk of bias. These studies generally provided clear inclusion criteria and used valid and reliable measures for both exposure and condition [31,33,34,35,40]. However, none of the studies identified and addressed cofounding factors, representing the most frequent limitation in this group. In addition, Mouzan et al. and Tsiountsiouria et al. [31,40] failed to describe the subjects in detail.
Among the ten cohort studies, three studies were rated as low risk of bias [36,37,38], six as moderate [28,30,32,39,41,42], and only one as high risk of bias [29]. Most cohort studies adequately measured exposures and outcomes. Again, most studies, except for the studies of Ashton et al. and Jakobsen et al. [37,38] failed to identify cofounding factors. While follow-up duration was often reported as sufficient, incomplete follow-up and lack of strategies to cope with incomplete follow-up contributed to elevated risk of bias in some studies [29,37]. Control groups typically consisted of age and sex matched healthy children from local populations or reference datasets, allowing for comparative analysis. Seven studies compared the UC patients with healthy controls [28,30,31,34,35,39,41], of which five studies used controls matched for age and gender [28,30,35,39,41]. The remaining eight studies used national [29,33,36,37,40,42] or WHO reference populations as comparators [32,38].
3.7. Results of Syntheses
All included studies were observational in design and involved relatively small UC subgroups within broader IBD cohorts. Substantial heterogeneity was observed across patient characteristics, outcome definitions, and assessment methods. The included studies indicated higher rates of poor nutritional status and growth impairment at diagnosis [32,34,36,37,39]. However, when disease activity was reported, the majority of included patients were in remission or had mild disease activity, yet still demonstrated a signal of poor nutritional status and growth impairment [30,33,34]. The overall risk of bias was low to moderate, with the most common limitations being inadequate control for confounding factors and incomplete reporting of UC-specific analyses.
4. Discussion
In this systematic review, we provide an overview of current knowledge in paediatric-onset UC on growth, nutritional status, and body composition in children and adolescents. Unlike previous related reviews, which primarily evaluated IBD as a whole group, our analysis focused specifically on patients with UC. Our findings showed that most studies assessing growth and nutritional parameters have reported findings in mixed IBD cohorts, often without presenting UC-specific data. Consequently, these results cannot be directly applied to the UC population, limiting disease-specific interpretation. Even among studies that did provide separate UC data, outcome definitions were frequently incomplete, sample sizes were small, and statistical power was rarely addressed. These limitations reduce confidence in the precision of reported associations and highlight the need for larger, UC-focused studies using standardized methods.
Across the included studies, there was substantial heterogeneity in the findings related to the assessment of growth, nutritional status and body composition. These differences can be explained by several factors. First, methodological diversity was evident, including variation in the definitions of growth failure and considerable diversity in the methods used to assess nutritional outcomes. Second, patient and disease characteristics varied across studies. The timing of outcome assessment differed (at diagnosis versus during prolonged disease), and although a higher proportion of patients in most studies were in remission or had mild disease activity, this likely influenced the results, leading to an underestimation of nutritional impairment. Third, differences in control group selection further contributed to heterogeneity, with some studies using matched healthy peers, others relying on general population datasets, and several using WHO or national reference populations.
When considering growth outcomes, most studies reported some degree of impairment among children with UC, with prevalence estimates ranging from 7% to 36%, depending on the criteria applied, with higher rates observed at diagnosis. Weight deficits were more frequently significant than height deficits, suggesting that linear growth impairment is less pronounced in UC. Several longitudinal studies demonstrated that height outcomes often normalized in adolescence or adulthood, particularly with adequate disease control. However, males diagnosed before puberty appeared more vulnerable to reduced final height, suggesting a critical window of risk during early growth. Multiple factors may contribute to impaired growth in UC. Persistent intestinal inflammation can disrupt the growth hormone–IGF-1 pathway, while corticosteroid exposure and reduced nutritional intake during active disease may further impair growth velocity [15]. Growth impairment is generally more severe and prevalent in CD than in UC, largely due to small intestinal involvement, malabsorption, and prolonged inflammation before diagnosis [24]. This difference may, in part, be explained by differences in diagnostic delay and clinical presentation. A large cross-sectional, multicenter Canadian cohort study of 1092 newly diagnosed IBD patients reported a significantly shorter diagnostic delay in those with UC or IBD-unclassified (n = 394) compared with CD [4.7 months, IQR 2.2–10.6 months, vs. 2.9 months, IQR: 1.3–6.5 months, respectively; p < 0.001] [43]. This shorter diagnostic delay may partly explain the lower prevalence of linear growth failure observed in UC. The study also found that patients with UC or IBD-unclassified more frequently presented with bloody diarrhea (87%) and experienced a high rate of weight loss (62%), indicating that nutritional deficits can still occur despite relatively preserved height. These findings underscore the importance of comprehensive nutritional monitoring in all patients with IBD. Notably, the study reported a low rate of linear growth failure, with results presented by combining UC and IBD-unclassified cases rather than analysing UC separately. Moreover, the definition of growth failure and the reference standards used were not specified [43].
Our review identified a dual burden of undernutrition and overnutrition in paediatric UC. Undernutrition at diagnosis was common, with prevalence rates of up to 25%, despite the fact that the majority of patients were in remission. Studies from Poland and the UK demonstrated significantly lower BMI z-scores than in controls, despite low stunting rates, suggesting early depletion of body weight relative to height [33,38]. Conversely, overweight and obesity were also reported in several cohorts. While most studies found no significant differences from controls, a study from Saudi Arabia identified a significantly higher prevalence of overweight [40]. This may partly reflect the global rise in obesity, but could also indicate that in certain populations, such as the Saudi cohort, the prevalence of overweight among UC patients is disproportionately higher, potentially influenced by regional dietary or lifestyle factors [44]. Overall, BMI alone may not adequately capture nutritional status in UC, as it can obscure both muscle deficits and excess adiposity, particularly during remission.
Altered body composition represents another important dimension of poor nutritional status in paediatric UC. The studies assessing body composition were limited to small cohorts (n = 12–40) and relied primarily on indirect methods such as BIA and anthropometry, with no studies using the gold-standard DXA [30,31,34,35,41]. Although DXA provides the highest accuracy, its use is limited by low feasibility and the need for specialised equipment. BIA is more practical and accessible for routine care, but its accuracy may be influenced by hydration status and high BMI. Anthropometric and functional measures may complement assessment but cannot reliably diagnose low muscle mass [16]. The wide range of assessment tools and cut-offs used across studies limits comparability and hampers synthesis of the evidence. Despite these limitations, two studies identified significantly reduced lean mass [34,35], even when height and BMI were within normal ranges, suggesting subclinical muscle depletion. In contrast, other studies reported no significant differences in fat mass, fat-free mass, or functional strength compared with healthy controls [31,33]. Longitudinal findings showed improvement in lean tissue indices following disease control [30,41]; however, the magnitude and clinical relevance of these changes remain uncertain. These mixed results and the study limitations emphasize the need for more quality studies to assess body composition in paediatric UC.
This systematic review has limitations related to the review process. Due to substantial heterogeneity in study design, outcome definitions, and assessment methods, a quantitative synthesis or meta-analysis was not feasible and results were therefore summarised narratively. In addition, the review is limited the ability to perform stratified analyses by disease severity, disease duration, or treatment exposure. Finally, the lack of access to individual patient data precluded more granular analyses. The multifactorial pathways contributing to poor nutritional status, altered body composition, and growth impairment in paediatric UC are summarised in Figure 2, which serves as a conceptual framework to contextualise both the findings and the limitations of this review.
In conclusion, the limited available evidence suggests that children and adolescents with UC may experience poor nutritional status, manifesting as both undernutrition and overnutrition, as well as growth impairment. Although the available data are heterogeneous and largely observational, and the reported prevalence ranges vary widely and statistical significance was not consistently assessed, the findings across studies suggest a signal of growth impairment and poor nutritional status that may have important implications for patient health. As nutritional status influences both disease outcomes and quality of life, accurate and early detection of these impairments is essential. From a clinical perspective, regular screening for growth impairment and undernutrition at diagnosis is recommended, with continued monitoring of weight, height, and pubertal progression throughout the disease course. Nutritional evaluation should also include body composition and functional strength assessments, with early referral to specialised dietitians for individualised guidance, ensuring adequate macro- and micronutrient intake and promoting overall high-quality dietary patterns. Nutritional management is a key component in the care of paediatric UC, supporting both the prevention of malnutrition and the promotion of optimal growth and development. Based on the findings of this systematic review, future studies should prioritize larger, UC-exclusive cohorts with well-defined control groups, standardized outcome measures, and high-accuracy body composition methodologies. These priorities reflect key methodological gaps consistently identified across the included studies. Moreover, research should consider the influence of disease activity, corticosteroid exposure, biologic therapy, pubertal stage, and ethnicity to better clarify the interplay between disease and nutritional status.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hill R.J. Update on nutritional status, body composition and growth in paediatric inflammatory bowel disease World J. Gastroenterol.2014203191319710.3748/wjg.v 20.i 12.319124696604 PMC 3964391 · doi ↗ · pubmed ↗
- 2Bischoff S.C. Bager P. Escher J. Forbes A. Hebuterne X. Hvas C.L. Joly F. Klek S. Krznaric Z. Ockenga J. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease Clin. Nutr.20234235237910.1016/j.clnu.2022.12.00436739756 · doi ↗ · pubmed ↗
- 3Liu S. Ding X. Maggiore G. Pietrobattista A. Satapathy S.K. Tian Z. Jing X. Sarcopenia is associated with poor clinical outcomes in patients with inflammatory bowel disease: A prospective cohort study Ann. Transl. Med.20221036710.21037/atm-22-112635433981 PMC 9011317 · doi ↗ · pubmed ↗
- 4Norman K. Kirchner H. Lochs H. Pirlich M. Malnutrition affects quality of life in gastroenterology patients World J. Gastroenterol.2006123380338510.3748/wjg.v 12.i 21.338016733855 PMC 4087869 · doi ↗ · pubmed ↗
- 5Prince A.C. Moosa A. Lomer M.C. Reidlinger D.P. Whelan K. Variable access to quality nutrition information regarding inflammatory bowel disease: A survey of patients and health professionals and objective examination of written information Health Expect.2015182501251210.1111/hex.1221924934409 PMC 5810632 · doi ↗ · pubmed ↗
- 6Assa A. Aloi M. Van Biervliet S. Bronsky J. di Carpi J.M. Gasparetto M. Gianolio L. Gordon H. Hojsak I. Hudson A.S. Management of paediatric ulcerative colitis, part 2: Acute severe colitis-An updated evidence-based consensus guideline from the European Society of Paediatric Gastroenterology, Hepatology and Nutrition and the European Crohn’s and Colitis Organization J. Pediatr. Gastroenterol. Nutr.20258181685110.1002/jpn 3.7009640528309 · doi ↗ · pubmed ↗
- 7van Rheenen P.F. Aloi M. Assa A. Bronsky J. Escher J.C. Fagerberg U.L. Gasparetto M. Gerasimidis K. Griffiths A. Henderson P. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update J. Crohns. Colitis 20211517119410.1093/ecco-jcc/jjaa 16133026087 · doi ↗ · pubmed ↗
- 8Thangarajah D. Hyde M.J. Konteti V.K. Santhakumaran S. Frost G. Fell J.M. Systematic review: Body composition in children with inflammatory bowel disease Aliment. Pharmacol. Ther.20154214215710.1111/apt.1321826043941 · doi ↗ · pubmed ↗