Psychological and Psychiatric Consequences of Prolonged Fasting: Neurobiological, Clinical, and Therapeutic Perspectives
Vincenzo Bonaccorsi, Vincenzo Maria Romeo

TL;DR
Prolonged fasting can reduce stress and depressive symptoms in healthy people but may worsen mental health in vulnerable individuals, with cultural and religious practices also influencing outcomes.
Contribution
This review provides a comprehensive analysis of the psychological and psychiatric effects of prolonged and intermittent fasting, including insights from religious practices.
Findings
Short-term fasting was linked to modest reductions in depressive symptoms and perceived stress in healthy adults.
Religious fasting showed similar neuropsychological effects, with cultural context playing a moderating role.
Vulnerable individuals, such as those with eating disorders, faced risks of mood destabilization and behavioral relapse.
Abstract
Background/Objectives: Prolonged fasting—defined as voluntary abstinence from caloric intake for periods exceeding 24 h—is increasingly recognized not only as a metabolic intervention but also as a psycho-behavioral modulator. According to the 2024 international consensus, intermittent fasting encompasses diverse temporal patterns including time-restricted feeding, alternate-day fasting, and periodic fasting of multi-day duration. While metabolic benefits are well documented, the psychoneurobiological and psychiatric consequences remain incompletely characterized. This review critically appraises current evidence on the psychological and psychiatric effects of prolonged and intermittent fasting, including both secular and religious practices. Methods: A narrative synthesis was conducted on clinical trials, observational studies, and translational research published between January 2010…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
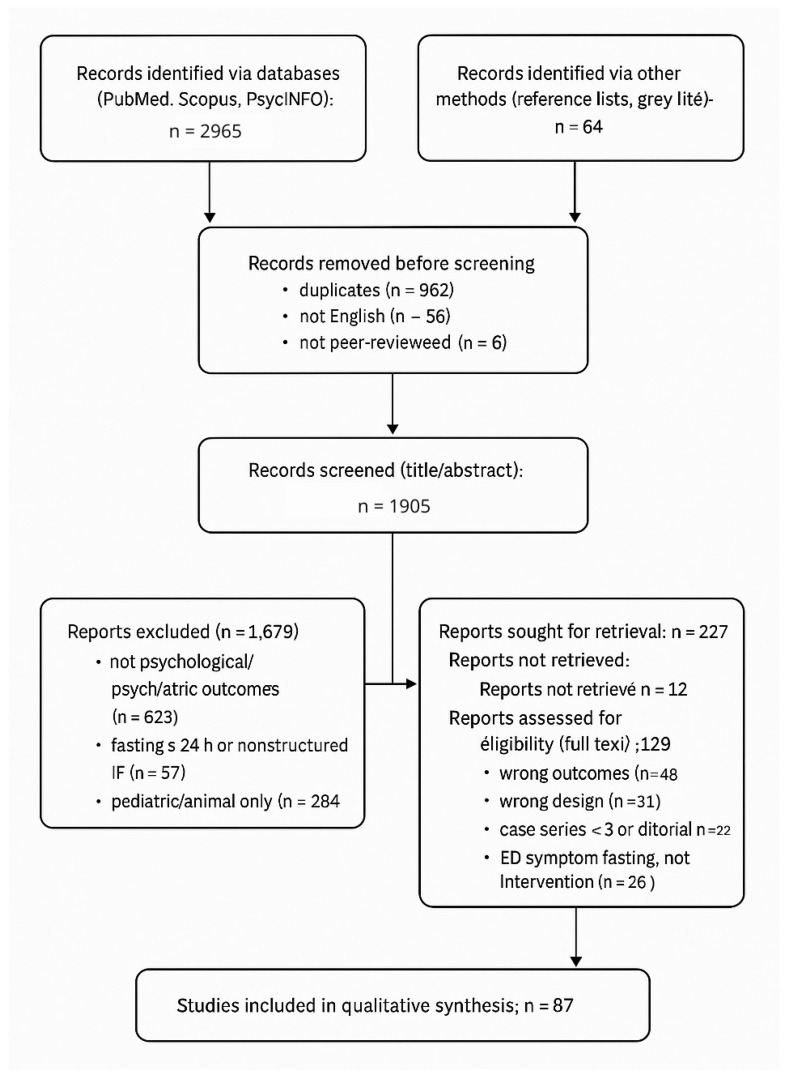 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDietary Effects on Health · Genetics, Aging, and Longevity in Model Organisms · Diet and metabolism studies
1. Introduction
Intermittent fasting (IF) encompasses four macro-categories recently codified by the International Consensus on Fasting Terminology—time-restricted eating (TRE), alternate-day fasting (ADF), periodic prolonged fasting (PPF ≥ 48 h) and religious/ritual fasting (RRF) [1]. Over the past decade IF—whether practiced as ≥24 h water-only fasts, 5:2 schedules, or multiday interventions—has moved from niche to mainstream, driven by its documented metabolic benefits [2,3,4]. Public and scientific interest in fasting has increased over the past decade, as reflected by the growing number of registered trials and peer-reviewed publications examining metabolic and mental-health endpoints. Yet weight-centered endpoints dominate these studies, leaving the neuropsychiatric dimension underexplored.
At the mechanistic level, metabolic switching from hepatic glycogenolysis to ketogenesis elevates circulating β-hydroxybutyrate (BHB), which crosses the blood–brain barrier and serves as an efficient neuronal substrate [5]. BHB functions as a class-I histone-deacetylase inhibitor, modulating transcription programs linked to synaptic plasticity and oxidative-stress resilience [6]. Pre-clinical work shows that intermittent or prolonged fasting boosts hippocampal brain-derived neurotrophic factor (BDNF), promotes mitochondrial biogenesis, dampens microglial activation, and recalibrates hypothalamic–pituitary–adrenal (HPA)-axis signaling—pathways tightly linked to mood and stress disorders [7,8].
Human evidence is heterogeneous. A 2023 systematic review of 15 RCTs reported that IF produced small-to-moderate reductions in depressive symptoms (Hedges g = 0.32) without major adverse events [9]; a 12-month TRE trial documented sustained improvements in Patient Health Questionnaire-9 scores alongside 8 % weight loss [10]. Conversely, a 2024 scoping review highlighted that prolonged fasts (>7 days) can heighten neuro-inflammatory markers such as IL-6 and TNF-α, raising concerns for at-risk psychiatric cohorts. Case reports still describe affective lability, anxiety spikes and, in vulnerable persons, fasting-related psychosis or mania.
Public adoption via wellness culture further blurs the boundary between therapeutic practice and disordered-eating behavior, especially among adolescents and perfectionistic young adults [11]. Thus, fasting emerges as a bidirectional tool: neuroplastic, anti-inflammatory, and potentially resilience-enhancing on one side; psychopathology-triggering when misapplied.
Objectives. This narrative review aggregates literature from 2010 to June 2025 on the psychological and psychiatric sequelae of prolonged fasting. Specifically, (i) integrating mechanistic insights connecting fasting to neural and endocrine pathways; (ii) appraising clinical data on mood, cognition, and psychiatric symptoms; (iii) delineating risk profiles and adverse events—including those linked to religious practices such as Ramadan and Orthodox fasting; and (iv) proposing evidence-based clinical guidelines and research priorities. By clarifying these domains, we aim to help clinicians harness fasting’s therapeutic potential while safeguarding vulnerable populations. This review integrates mechanistic, preclinical, and clinical perspectives to bridge biological and behavioral evidence on fasting and mental health, with emphasis on operational guidance for safe clinical translation.
2. Materials and Methods
2.1. Literature Search Strategy
A narrative search was carried out in PubMed/MEDLINE, Scopus, and PsycINFO for articles published from 1 January 2010 to 30 June 2025. The string (“prolonged fasting” OR “intermittent fasting” OR “alternate-day fasting” OR “time-restricted feeding”) AND (“psychology” OR “psychiatry” OR “mood” OR “cognition” OR “stress”) was applied to titles, abstracts, and keywords. Reference lists of retrieved papers and recent systematic reviews were screened manually to capture additional studies.
2.2. Eligibility Criteria (Pre-Specified)
We included studies meeting the following a priori criteria. Population (humans): Adults (≥18 years); adolescent samples were considered only when psychological/psychiatric outcomes were explicitly assessed. Interventions/exposures: Fasting paradigms, namely, time-restricted eating (TRE), alternate-day fasting (ADF), periodic/prolonged fasting, and religious/ritual fasting. Comparators: Any (active control, usual diet, parallel control, or within-subject pre–post). Human outcomes: Validated psychological/psychiatric endpoints (e.g., HDRS-17, PHQ-9, GAD-7, STAI-S, BAI; clinician-assessed relapse/recurrence) and/or stress-physiology/autonomic markers with a clear mental-health relevance (e.g., morning salivary cortisol, high-frequency heart-rate variability [HF-HRV]). Preclinical inclusion: In vivo studies directly pertinent to neurobiological pathways of mood, anxiety, or psychosis (e.g., BHB→NLRP3, BDNF/PGC-1α signaling, hypothalamic–pituitary–adrenal axis recalibration). Designs: Randomized controlled trials (RCTs), non-randomized trials, cohorts, case–control, pre–post studies, and case series (humans); in vivo experiments (preclinical). In vitro studies were excluded unless tightly anchored to converging in vivo evidence. Language/time window: English; January 2010–June 2025.
Exclusion codes (mapped to PRISMA boxes in Figure 1) were defined as follows: wrong outcomes—absence of validated psychological/psychiatric measures or mental-health-relevant physiological markers (studies reporting only metabolic/weight outcomes without mental-health endpoints); wrong population—purely pediatric samples; severe medical cohorts without mental-health outcomes; animal/in vitro work not mechanistically relevant; wrong intervention—calorie restriction without a fasting component or diet/supplement interventions unrelated to fasting; wrong design—editorials, narrative opinions without primary data, conference abstracts without a retrievable full text; reports not retrieved—full texts unobtainable after institutional access attempts and author contact; duplicates—multiple reports from the same cohort, in which case the most complete version was retained.
2.3. Information Sources and Search Strategy
We searched PubMed/MEDLINE, Scopus, and PsycINFO for records published from January 2010 through June 2025. The search combined controlled vocabulary and free-text terms for fasting paradigms and mental-health outcomes (e.g., “prolonged fasting” OR “intermittent fasting” OR “time-restricted eating” OR “alternate-day fasting” OR “religious fasting”) AND (psycholog* OR psychiatr* OR mood OR anxiety OR stress OR depression). Core MeSH/keywords included fasting; intermittent fasting; time-restricted eating/feeding; alternate-day fasting; religious fasting (Ramadan, Eastern Orthodox); and mental-health terms (psychology, psychiatry, mood, depression, anxiety, stress, cognition, HPA axis, BDNF). Full Boolean strings and database-specific filters are reported in Table S1 (Supplementary Materials). We performed backward and forward citation chasing of included records. “Gray literature” was limited to reference-list screening and trial-registry checks; non-peer-reviewed materials (preprints, theses, abstracts without retrievable full texts) were excluded. Duplicates were removed using reference-manager de-duplication and manual verification.
2.4. Study Selection and Data Extraction
Titles/abstracts and then full texts were screened in duplicate by two reviewers working independently; disagreements were resolved by a third reviewer. For each eligible study we extracted, on pilot-tested forms, the design, population/sample, clinical status/diagnosis, fasting protocol (type, timing, duration), comparator, psychometric instruments, follow-up window, key psychological/psychiatric outcomes, and a brief design-level risk-of-bias note. These fields are summarized for human studies in Table 1 (Summary of human evidence linking prolonged fasting to key psychological outcomes) and correspond to the columns reported in Table 2. Preclinical data items included species/strain, fasting paradigm, mechanistic readouts, and behavioral endpoints when applicable. Data integrity and consistency checks were performed prior to synthesis, and reasons for exclusion at the full-text stage were recorded and are summarized in Figure 1 and detailed in Table S1.
2.5. Quality Assessment
Randomized controlled trials were appraised with the Cochrane RoB-2 tool, observational studies with the Newcastle–Ottawa Scale, and animal studies with the SYRCLE risk-of-bias tool. Narrative grades (low, moderate, or high risk of bias) were assigned to each study. Overall, randomized trials exhibited low-to-moderate risk of bias, mainly due to incomplete blinding and selective reporting; observational studies were moderate, with residual confounding and measurement variability; animal studies showed variable risks related to randomization and outcome assessment. These considerations informed the narrative grading of evidence strength.
2.6. Data Synthesis
Given heterogeneity in fasting regimens, psychiatric assessments, and endpoints—most relying on self-report instruments rather than clinician-administered interviews [23,24], a quantitative meta-analysis was not feasible. Results were therefore synthesized qualitatively, with particular attention to protocol duration, psychiatric stratification, and outcome directionality.
3. Results
3.1. Study Selection
The database and manual search identified 3029 records. After removal of duplicates (n = 962), non-English (n = 96), and non–peer-reviewed items (n = 6), 1905 records were screened. Of these, 227 reports were sought for full-text retrieval, 129 were assessed for eligibility, and 87 studies (39 human; 48 preclinical) were included in the qualitative synthesis (Figure 1; Table S1).
3.2. Characteristics of Included Human Studies
The human evidence base comprised randomized controlled trials, non-randomized trials, cohort studies, pre–post investigations, and observational studies spanning time-restricted eating (TRE), supervised prolonged fasting programs (e.g., Buchinger regimens), and religious fasting. For each study, design, sample characteristics, fasting protocol (type, timing, duration), comparator, psychometric instruments, follow-up, and outcomes are summarized in Table 2. Across human trials, intervention durations typically ranged from 4 to 12 weeks for TRE and 4–21 days for supervised prolonged fasting programs. Sample sizes were predominantly small-to-moderate (≈20–100). Primary assessment tools included PHQ-9/BDI-II (depression), GAD-7/STAI-S (anxiety), PSS (perceived stress), and selected cognitive tests (executive/working-memory tasks).
3.3. Synthesis of Human Outcomes
Across metabolically healthy adults, TRE and supervised prolonged fasting were associated with small improvements in depressive symptomatology and perceived stress; effect magnitudes varied by baseline symptom burden and the degree of supervision. Supervised Buchinger-type programs consistently reported reductions in State-Trait Anxiety Inventory-State (STAI-S) scores, lower morning salivary cortisol, and increases in high-frequency heart-rate variability (HF-HRV). Religious fasting yielded mixed findings: Eastern Orthodox Great Lent was associated with modest reductions in Perceived Stress Scale and Beck Anxiety Inventory scores [25], whereas during Ramadan, a higher relapse risk in bipolar disorder was observed under specific clinical conditions. Severe adverse events were uncommon but documented: isolated psychotic or manic decompensations occurred in vulnerable individuals, and restrictive-eating phenotypes tended to worsen in the absence of clinical supervision.
Overall, most human studies reported favorable changes in mood and/or perceived stress under circadian-aligned TRE or supervised prolonged fasting, whereas neutral findings were more common in longer, unsupervised, or less structured regimens.
3.4. Synthesis of Preclinical Mechanisms
In vivo studies converged on several pathways plausibly linking fasting to affective and stress-related outcomes: ketone-mediated signaling (e.g., β-hydroxybutyrate effects on the NLRP3 inflammasome), neurotrophic modulation (brain-derived neurotrophic factor and PGC-1α-related mitochondrial programs), hypothalamic–pituitary–adrenal axis recalibration, gut–brain interactions influencing barrier integrity and microglial activation, and immuno-oxidative attenuation. Most preclinical evidence derives from rodent models (mice/rats) employing 24–72 h fasting or TRF paradigms. While these data elucidate plausible mechanisms (e.g., BHB→NLRP3, BDNF/PGC-1α), species differences, protocol heterogeneity, and behavioral readouts limit direct clinical extrapolation.
4. Neurobiological and Neurochemical Effects of Prolonged Fasting
Prolonged fasting precipitates a rapid metabolic switch from hepatic glycogenolysis to ketogenesis, elevating circulating β-hydroxybutyrate (BHB), acetoacetate, and acetone within 24–48 h. During prolonged fasting or ketogenic states, circulating β-hydroxybutyrate (BHB) crosses the blood–brain barrier via monocarboxylate transporters and can supply a substantial fraction of cerebral ATP demand, in addition to its signaling functions [26]. Importantly, BHB is not merely a fuel; it operates as a pleiotropic signaling metabolite that engages host receptors and epigenetic machinery.
4.1. Ketone Signaling and Neurotransmission
BHB binds to hydroxycarboxylic acid receptor-2 (HCA2) on microglia, inhibiting NLRP3-inflammasome activation and downstream IL-1β release—an anti-inflammatory action germane to affective disorders [27]. As a class I histone-deacetylase inhibitor, BHB increases histone H3 acetylation at promoters of neuronal resilience genes such as BDNF and Peroxisome proliferator-activated receptor gamma coactivator 1-alpha (PGC1α) (Figure S1), thereby enhancing synaptic plasticity [28,29]. Rodent hippocampal slices exposed to physiological ketone concentrations exhibit augmented GABAergic tone and reduced glutamatergic excitability, effects reproduced in vivo by 48 h fasting [30]. These shifts underpin the anticonvulsant and anxiolytic profile of ketogenic interventions. In humans, supervised 4–21-day Buchinger fasting programs have been associated with significant reductions in perceived tension/anxiety and morning salivary cortisol, alongside increases in high-frequency heart-rate variability, indicating strengthened parasympathetic control [31].
4.2. Mitochondrial Biogenesis and Autophagy
Energy scarcity activates AMP-activated protein kinase (AMPK) and sirtuin-1, leading to PGC-1α-driven mitochondrial biogenesis, enhanced mitophagy, and up-regulation of antioxidant enzymes including superoxide-dismutase-2 [32]. Fasting-induced autophagic flux clears dysfunctional organelles and misfolded proteins; in neuronal cultures, a single 24 h nutrient deprivation period reduces α-synuclein aggregates via ULK1 activation [33].
4.3. Neuroendocrine and Autonomic Recalibration
Acute fasts elevate cortisol and catecholamines, yet repeated cycles dampen basal ACTH and enhance vagal tone, suggesting a recalibrated hypothalamic–pituitary–adrenal axis (Figure 1) conducive to stress resilience [34]. Concomitantly, adiponectin—a metabolic hormone with AdipoR1-AMPK-mediated antidepressant effects—increases both peripherally and centrally, correlating with improvements in mood scores [35].
4.4. Gut–Brain Axis Modulation
Time-restricted feeding paradigms remodel gut microbial communities, enriching butyrate-producing taxa such as Roseburia and Faecalibacterium. These metabolites fortify blood–brain barrier integrity and dampen microglial activation, thereby influencing anxiety-like behavior in mice [36,37,38]. A pilot crossover study reported parallel shifts in microbial α-diversity and reductions in perceived stress after two weeks of 16:8 fasting in healthy adults [39].
4.5. Immuno-Oxidative Landscape
Meta-analytical evidence indicates that fasting interventions ≥4 weeks reduce high-sensitivity C-reactive protein, Tumor Necrosis Factor alpha (TNF-α), and Interleukin-6 (IL-6) by 10–30%, with concomitant down-regulation of NF-κB-responsive transcripts [40]. These changes mirror clinical improvements in depressive symptomatology and may constitute a mechanistic bridge linking metabolic and mood benefits.
Taken together, ketone-mediated signaling, mitochondrial rejuvenation, endocrine recalibration, microbiota reshaping, and immuno-oxidative dampening converge to form a neurobiological substrate through which prolonged fasting can influence cognition, emotion, and psychiatric vulnerability. Inter-individual variability in these cascades—driven by genetics, sex, circadian alignment, and psychiatric history—highlights the need for personalized protocols and mechanistic endpoints in future trials.
5. Psychological Outcomes
5.1. Mood
Emerging evidence positions prolonged or intermittent fasting (IF) as a double-edged sword in the affective domain. On one side, metabolic switching and the attendant rise in β-hydroxybutyrate (BHB) trigger neurotrophic, anti-inflammatory, and monoaminergic cascades that may convey antidepressant and anxiolytic benefits; on the other, caloric deprivation can destabilize mood in susceptible individuals, particularly when fasting is unsupervised or prolonged. Below, we synthesize data across preclinical models, mechanistic biomarker studies, and clinical trials, highlighting moderators that tilt the fasting–mood relationship toward resilience or risk.
Rodent models demonstrate that 24–48 h water-only fasts increase hippocampal BDNF and activate the CREB–PGC-1α axis, yielding behavioral antidepressant-like phenotypes in forced-swim and tail-suspension tests [41]. Translationally, association between circulating BHB and proBDNF mRNA in human peripheral mononuclear cells, correlating with mood elevation [42]. A 2022 randomized controlled trial (RCT) in 93 adults with mild-to-moderate major depressive disorder (MDD) reported that a 4-week 16:8 IF protocol reduced Hamilton Depression Rating Scale (HDRS-17) scores by −4.8 ± 1.3 points versus −1.9 ± 1.1 in an isocaloric three-meal control, accompanied by increased serum BDNF and lower high-sensitivity C-reactive protein [43]. These findings align with a recent network meta-analysis [44] showing small-to-moderate effect sizes (Hedges g = 0.29) for depressive symptom reduction across six IF randomized controlled trials (Figure 1). Representative randomized trials reported small-to-moderate symptom reductions on clinician-rated (e.g., HDRS-17) and self-report measures (e.g., STAI-S, PHQ-9), sometimes accompanied by BDNF shifts. Conversely, null effects on BDI-II/POMS at 12 months under less intensive TRE underscore heterogeneity by protocol duration, baseline symptoms, and assessment modality.
5.2. Anxiety
Fasting modulates hypothalamic GABA/glutamate ratios and attenuates NLRP3-inflammasome activity, mechanisms implicated in anxiolysis (Figure 1). In mice, a 24 h fast reduces anxiety-like behavior and improves memory via brain-wide reductions in caspase-1 activity (a key regulator of IL-1β maturation) [45]. Clinically, healthy adults undergoing a 10-day Buchinger water fast exhibited significant reductions in State-Trait Anxiety Inventory-State (STAI-S) scores [46]. However, anxiety outcomes across trials are heterogeneous, partly due to differing baseline anxiety levels and assessment tools.
Psychological responses to fasting vary markedly by sex, psychiatric history, and hormonal milieu. Women with pre-existing MDD or bipolar II disorder appear particularly vulnerable to mood destabilization during calorie restriction [47]. Fasting-induced hypoglycaemia, cortisol surges, and sleep fragmentation may jointly precipitate irritability, anergia, or mixed affective states. In an observational cohort of 1 214 Ramadan fasters, 7.4% of participants with a prior mood-disorder diagnosis experienced clinically significant symptom exacerbation [48].
Sleep disruption is a salient mediator: in a randomized pilot trial, early time-restricted eating shifted sleep timing in late sleepers; independently, selective REM-sleep suppression increases next-day negative affect [49]. Moreover, fasting can cue maladaptive cognitive–emotional schemas in individuals with dieting history, potentiating rumination and guilt, which are transdiagnostic risk factors for depression [50].
Collectively, data suggest a U-shaped relationship wherein moderate, circadian-aligned fasting confers modest affective benefits in metabolically healthy adults, while aggressive or prolonged restriction heightens risk in vulnerable groups. Screening for mood-disorder history, sleep quality, and stress load is therefore essential before prescribing fasting interventions. We recommend (i) starting with ≤14 h fasting windows, (ii) maintaining consistent bedtime to preserve REM sleep, (iii) monitoring glucose and cortisol in patients with affective disorders, and (iv) integrating cognitive–behavioral strategies to mitigate guilt-based cognitions. Large-scale, stratified RCTs with clinician-rated endpoints and ≥6-month follow-up are urgently needed to define safety boundaries.
5.3. Stress Correlations
Fasting elicits a biphasic stress response. Acutely (<24 h), glycogen depletion activates the hypothalamic–pituitary–adrenal (HPA) axis, elevating ACTH and cortisol to mobilize glucose and free fatty acids (Figure 1), whereas with repeated cycles, homeostatic recalibration emerges, characterized by blunted basal cortisol, enhanced vagal tone, and lower heart-rate-variability indices of sympathetic drive [51]. In middle-aged mice, eight weeks of alternate-day fasting normalized diurnal corticosterone, up-regulated hippocampal glucocorticoid-receptor phosphorylation, and improved stress-coping in forced-swim and tail-suspension tests [52]. Translationally, in adults completing a 10-day Buchinger water fast, morning salivary cortisol decreased (≈18%) and high-frequency HRV increased, consistent with strengthened parasympathetic control and stress-system recalibration [53].
5.4. Religious Fasting
Structured religious fasts (e.g., those aligning feeding to circadian windows or imposing abstention from specific macronutrients) plausibly recruit similar stress-system adaptations, while differing in intent, oversight, and social context. At the immune–neuroendocrine interface, fasting paradigms comparable to religious regimens have been associated with 10–30% reductions in circulating IL-6 and TNF-α and with down-regulation of NF-κB–responsive transcripts, changes that track improvements in perceived stress and mood [54]. Mechanistically, ketosis emerging in longer fasts can exert ketone-mediated anti-inflammatory effects—β-hydroxybutyrate directly inhibits the NLRP3 inflammasome—thereby attenuating innate-immune activation relevant to stress responsivity and affective outcomes [55]. Human fasting programs with supervised protocols further illustrate feasibility and safety signals (cortisol reduction, HRV shifts), offering a translational bridge to religious contexts where adherence, sleep timing, and communal practices may modulate stress-related benefits [56]. Analyses of Ramadan studies should account for confounders such as altered sleep timing, caffeine intake, medication dosing schedules (e.g., lithium), and daily routine changes, which can independently influence mood or relapse risk.
5.5. Severe Adverse Events
5.5.1. Eating Disorders
Structured fasting overlaps phenomenologically with restrictive-eating pathology. Individuals with anorexia nervosa, atypical anorexia, or high-functioning orthorexia often employ extended fasts as compulsive rituals, reinforcing dopaminergic reward dysregulation, interoceptive mistrust, and perfectionism-driven hyper-control [57]. Epidemiological surveys indicate that up to 38% of female college students practicing intermittent fasting meet threshold or sub-threshold criteria for an eating disorder [58]. Wellness-culture promotion of IF may thus mask prodromal ED behaviors. Pre-intervention screening for dietary rigidity, body-image concern, and obsessive–compulsive traits is imperative; where such red flags surface, fasting should be deferred or implemented only within a specialized ED framework.
5.5.2. Psychosis
Although uncommon, psychotic decompensations during prolonged fasting have been reported—for example, recurrent paranoid-hallucinatory episodes immediately following week-long fasts in a patient with anorexia nervosa—and Ramadan fasting has been associated with higher relapse risk in bipolar disorder in observational data. Mitigation strategies include maintaining antipsychotic dosing schedules, encouraging nocturnal caloric intake to stabilize glycaemia, and providing close psychiatric follow-up during the fasting period (see Table S1 in the Supplementary Materials for discontinuation criteria).
In support of the synthesis above, Table 2 provides a detailed, study-level overview of human investigations (2010–2025) across fasting paradigms (Buchinger fasting, TRE/eTRE, FMD, Ramadan), including sample characteristics, protocols, psychometric measures, follow-up, outcomes, and design-level risk of bias.
6. Clinical Integration and Ethical Considerations
6.1. Therapeutic Fasting in Psychiatric Populations
Early-phase studies have begun testing fasting-mimicking diets (FMDs), alternate-day fasting, and 16:8 time-restricted eating (TRE) as adjuncts to standard care in major depressive disorder, post-traumatic stress disorder, and mild cognitive impairment. A randomized controlled pilot trial in adults with major depression (n = 20) showed that adding three monthly cycles of a fasting-mimicking diet to structured psychotherapy improved self-esteem and psychological quality of life versus psychotherapy alone, with comparable depressive-symptom reduction across groups [59]. An ongoing randomized controlled trial is comparing time-restricted eating with a Mediterranean-diet control for symptom reduction and quality of life in bipolar disorder, with rater-blinded assessments across 8–15 months. Despite these encouraging signals, fasting remains contraindicated or high-risk in patients with active psychosis, severe impulse-control disorders, borderline personality disorder with suicidality, and uncontrolled substance use.
Clinical checklist (monitoring and safety):
- Initial assessment (week 0): Psychiatric history; current diagnoses; ED screening; suicidality; medications; metabolic panel (electrolytes, glucose/ketones if applicable); BMI and weight trajectory; sleep and caffeine use.
- Protocol start: For at-risk patients, prefer ≤14 h fasting windows; maintain consistent sleep timing; avoid abrupt medication schedule changes.
- Follow-up (every 2 weeks): Clinician-rated scales (e.g., HDRS-17, CGI-S/CGI-I), self-report (PHQ-9/GAD-7/PSS), adverse-event checklist (psychiatric and somatic), weight/BMI, basic labs if indicated.
- Discontinuation criteria (“STOP”): ≥5% weight loss in <4 weeks, emergent suicidality, psychotic or manic symptoms, severe anxiety/agitation, electrolyte derangements, or clinically significant sleep disruption non-responsive to adjustments.
- Coordination: Multidisciplinary oversight (psychiatry, nutrition/dietetics, internal medicine/endocrinology), with shared decision-making and informed consent emphasizing uncertain long-term efficacy.
6.2. Ethical and Clinical Governance
Implementing fasting interventions in psychiatric settings raises distinct ethical imperatives. Informed consent must articulate (i) uncertain long-term efficacy, (ii) potential for mood destabilization or metabolic derangement, and (iii) the right to withdraw without prejudice. High-risk conditions include active eating disorders (anorexia nervosa, bulimia nervosa, severe ARFID), unstable mood or psychotic disorders, and patients under active psychopharmacological treatment with narrow therapeutic windows or dosing-time sensitivity (e.g., lithium, sedative-hypnotics); in such cases, fasting should be avoided or undertaken only with close medical supervision. Contraindication screening should encompass active eating disorders, BMI < 18.5 kg m^−2^, pregnancy, insulin-treated diabetes, cognitive impairment affecting decision-making capacity, and unstable cardiovascular or renal disease. A multidisciplinary team—psychiatrist, dietitian, internist/endocrinologist, and where available, clinical psychologist—should co-design the protocol and oversee monitoring.
Risk–benefit assessment ought to be continuous: laboratory review at baseline and week 4, structured mood and suicidality scales every fortnight, and caregiver check-ins for patients with limited insight. Ethics-committee oversight is advised for research applications, with rapid-response plans for adverse psychiatric events. Finally, fasting must remain a reversible, individualized adjunct rather than a one-size-fits-all replacement for evidence-based pharmacotherapy or psychotherapy.
7. Research Gaps and Future Directions
Despite burgeoning interest, the evidence base for prolonged fasting in psychiatric contexts remains nascent. Priority areas include the following:
- (1)Protocol standardization. Heterogeneous fasting windows (12–72 h), feeding macronutrient composition, and cycle duration hinder comparability; consensus statements mirroring exercise prescription guidelines are needed.
- (2)Psychiatric stratification. Forthcoming trials should stratify by diagnostic category, illness phase, and psychotropic medication to delineate differential risk–benefit profiles.
- (3)Long-term safety and efficacy. Most studies last ≤12 weeks; prospective cohorts ≥12 months are crucial to detect delayed metabolic, endocrine, or affective sequelae.
- (4)Mechanistic biomarkers. Integrative omics (metabolomics, epigenomics), inflammatory panels, and digital phenotyping of mood/sleep could clarify mediators and moderators of response.
- (5)Gut–brain axis. Controlled feeding studies isolating fiber and prebiotic intake will determine how microbiota shifts contribute to affective and cognitive outcomes.
- (6)Sex and age effects. Given hormonal modulation of HPA and reward circuitry, sex-specific and developmental-stage analyses are imperative.
- (7)Digital-assisted monitoring. Wearable glucose/ketone sensors and app-based mood tracking may enhance safety and adherence, yet require validation in psychiatric samples.
- (8)Expectancy bias mitigation. Employ blinded outcome assessors, neutral framing, and objective biomarkers (e.g., inflammatory panels, HRV, digital sleep metrics) to reduce expectancy and measurement biases.
- (9)Standardized adverse-event reporting. Adopt validated psychiatric terminology and structured AE taxonomies with severity/relatedness grading, enabling cross-study comparability and safety-signal detection.
Addressing these gaps will enable evidence-based, personalized fasting protocols and inform clinical guidelines.
8. Conclusions
Prolonged fasting represents a potent metabolic intervention whose neurobiological ripple effects extend to mood, cognition, stress physiology, and—under specific conditions—psychiatric risk. The balance between benefit and harm pivots on protocol design, individual vulnerability, and clinical oversight. Current data support cautious, short-duration, nutrient-replete fasting as an adjunct in select psychiatric populations, provided rigorous screening and monitoring frameworks are in place. Future research should adopt standardized protocols, stratify by diagnosis, sex, and developmental stage, and incorporate mechanistic biomarkers to establish causal pathways.
Large, multisite randomized controlled trials with ≥12-month follow-up—integrating digital phenotyping, wearable biosensors, and health-economic analyses—are now needed to verify efficacy, durability, and scalability. In parallel, real-world implementation studies should evaluate clinician training, patient acceptability, and equity of access across diverse healthcare settings. Future trials should prioritize clinician-rated endpoints, standardized psychiatric adverse-event reporting, and longer follow-up (≥6–12 months) to substantiate durability of mental-health benefits and refine safety boundaries across diagnostic strata.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Koppold D.A. Breinlinger C. Hanslian E. Kessler C. Cramer H. Khokhar A.R. Peterson C.M. Tinsley G. Vernieri C. Bloomer R.J. International consensus on fasting terminology Cell Metab.20243617791794.e 410.1016/j.cmet.2024.06.01339059384 PMC 11504329 · doi ↗ · pubmed ↗
- 2Longo V.D. Panda S. Fasting, circadian rhythms, and time-restricted feeding in healthy lifespan Cell Metab.2016231048105910.1016/j.cmet.2016.06.00127304506 PMC 5388543 · doi ↗ · pubmed ↗
- 3de Cabo R. Mattson M.P. Effects of intermittent fasting on health, aging, and disease N. Engl. J. Med.20193812541255110.1056/NEJ Mra 190513631881139 · doi ↗ · pubmed ↗
- 4Mattson M.P. Longo V.D. Harvie M. Impact of intermittent fasting on health and disease processes Ageing Res. Rev.201739465810.1016/j.arr.2016.10.00527810402 PMC 5411330 · doi ↗ · pubmed ↗
- 5Cervenka M.C. Wood S. Bagary M. Balabanov A. Bercovici E. Brown M.-G. Devinsky O. Di Lorenzo C. Doherty C.P. Felton E. International recommendations for the management of adults treated with ketogenic diet therapies Neurol. Clin. Pract.20211138539710.1212/CPJ.000000000000100734840865 PMC 8610544 · doi ↗ · pubmed ↗
- 6Shimazu T. Hirschey M.D. Newman J. He W. Shirakawa K. Le Moan N. Grueter C.A. Lim H. Saunders L.R. Stevens R.D. Suppression of oxidative stress by β-hydroxybutyrate, an endogenous histone deacetylase inhibitor Science 201333921121410.1126/science.122716623223453 PMC 3735349 · doi ↗ · pubmed ↗
- 7Anson R.M. Guo Z. de Cabo R. Iyun T. Rios M. Hagepanos A. Ingram D.K. Lane M.A. Mattson M.P. Intermittent fasting dissociates beneficial effects of dietary restriction on glucose metabolism and neuronal resistance to injury from calorie intake Proc. Natl. Acad. Sci. USA 20031006216622010.1073/pnas.103572010012724520 PMC 156352 · doi ↗ · pubmed ↗
- 8Chung H.Y. Kim H.J. Kim J.W. Yu B.P. The inflammation hypothesis of aging: Molecular modulation by calorie restriction Ann. N. Y. Acad. Sci.200192832733510.1111/j.1749-6632.2001.tb 05662.x 11795524 · doi ↗ · pubmed ↗