Participants’ Perspectives on Health Impact, Barriers and Facilitators to Adherence in a Mediterranean Diet Lifestyle Trial
Paloma Massó Guijarro, María Durán-Luque, Claudia Rojas-Medina, Naomi Cano-Ibáñez

TL;DR
This study explores what helped or hindered older Spanish adults in sticking to a Mediterranean diet and lifestyle program aimed at preventing chronic diseases.
Contribution
The study provides gender-sensitive insights into adherence facilitators and barriers in Mediterranean diet interventions.
Findings
Perceived health improvements and confidence in managing diet were key facilitators of adherence.
Low motivation, mobility issues, and lack of partner support were major barriers to adherence.
A strong relationship with the research team helped sustain long-term commitment.
Abstract
Background/Objectives: Interventions promoting the Mediterranean Diet (MedDiet) and healthy lifestyle behaviours are effective and cost-efficient in preventing non-communicable diseases (NCDs), yet sustaining adherence remains challenging. This study explored perceived health impacts on, barriers to, and facilitators of adherence among older Spanish adults participating in a randomised clinical trial (RCT) based on the MedDiet and lifestyle interventions. Methods: A qualitative study was conducted with 17 Spanish participants (aged 60–81 years) with overweight/obesity and metabolic syndrome (MetS). In-depth, semi-structured interviews were audio-recorded, transcribed verbatim, and analysed through inductive thematic analysis with a gender-sensitive approach. Results: Participants identified several facilitators, including perceived improvements in vitality, psychological well-being, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
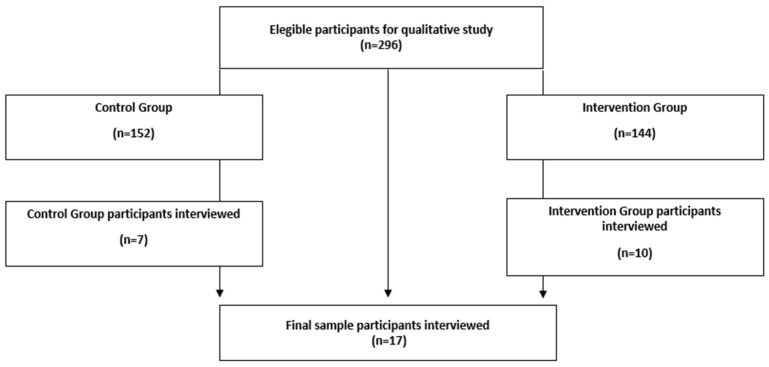 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Obesity and Health Practices · Diabetes Management and Education
1. Introduction
Non-communicable diseases (NCDs), the leading cause of mortality worldwide, represent a major challenge for public health [1]. Among the NCDs, metabolic syndrome (MetS) has a global prevalence of 31.4% [2,3]. The main causes and comorbidities associated with MetS are largely related to modifiable lifestyle factors, including unhealthy dietary habits and physical inactivity [4,5]. Consequently, public health agencies emphasise the need for preventive, cost-effective strategies to reduce the growing burden of NCDs on healthcare systems [6].
Research efforts have increasingly focused on interventions promoting healthy dietary patterns and lifestyle modifications [7,8,9]. Evidence from randomised clinical trials (RCTs) demonstrates that adherence to the Mediterranean Diet (MedDiet) is among the most effective approaches for preventing and managing MetS and its associated risk factors [10]. In most MedDiet RCTs, higher adherence to dietary recommendations has been strongly associated with improved health outcomes [11,12]. However, a key limitation of such trials lies in the high level of participant motivation required to sustain adherence and complete long-term follow-up [13]. Non-adherence rates of up to 50% have been reported, posing a significant barrier to achieving the anticipated health benefits [14].
Enhancing adherence to dietary and lifestyle interventions requires engaging participants to better understand the enablers and obstacles they face in changing established habits [15]. Despite the robust quantitative evidence supporting the benefits of MedDiet interventions, limited attention has been given to the behavioural, psychosocial, and gender-specific factors that influence adherence over time. Understanding these subjective experiences is essential to bridge the gap between efficacy under controlled trial conditions and real-world effectiveness. Identifying perceived barriers and facilitators within the target population allows researchers and practitioners to adapt intervention protocols, personalise support strategies, and improve long-term adherence and outcomes [16,17].
While quantitative studies have primarily examined the clinical outcomes of MedDiet RCTs [18], qualitative research offers valuable insights into the personal and contextual factors shaping adherence behaviours. This methodological approach provides a deeper understanding of how participants interpret and integrate dietary knowledge acquired during intervention programmes to their daily lives. This study explored perceived barriers and facilitators to adherence among older Spanish adults participating in an RCT based on MedDiet and lifestyle interventions.
2. Materials and Methods
2.1. Study Design
A qualitative content analysis study based on in-depth semi-structured interviews, ancillary to an ongoing 6-year randomised clinical trial (RCT) on the Mediterranean lifestyle, was conducted (Registration Number 89898870; http://www.isrctn.com/ISRCTN89898870, accessed on 6 November 2025). The RCT aimed to evaluate an intensive lifestyle intervention programme promoting traditional MedDiet, physical activity, and behavioural support for cardiovascular disease prevention, compared with usual care and general dietary counselling. The protocol and main results of the trial have been reported elsewhere [5,19]. This qualitative study followed the Standards for Reporting Qualitative Research (SRQR) [20] to ensure methodological rigour and transparency. In addition, the study adhered to the Sex and Gender Equity in Research (SAGER) guidelines to guarantee the systematic integration of a gender perspective throughout the study design, methodology, and data analysis [21,22] (Supplement S1).
2.2. Sample Selection
Participants were selected from the larger randomised clinical trial cohort (n = 296) at the Granada research site, following a maximum variation purposive strategy to capture a broad range of experiences [23]. The target population of the trial comprised community-dwelling older adults (men aged 55–75 years, and women aged 60–75 years) with overweight or obesity (BMI between 27 and 40 kg/m^2^), free from cardiovascular disease at enrollment, and diagnosed with MetS.
To achieve diversity within the qualitative sample, participants were chosen to represent differences in sociodemographic factors such as age, gender, marital (widowed, married, divorced, and never married) and occupational status (active, retired, and never working), educational level (primary, secondary, and university), number of cohabitants, and place of residence (urban or rural). Additional inclusion considerations were related to participants’ engagement in the trial, including allocation group, degree of weight change during the first six months, improvement in adherence to MedDiet, motivation to remain in the study, and attendance at follow-up visits. The inclusion of participants from both the intervention and control groups was intentional and consistent with the qualitative aim of capturing a wide range of experiences related to perceived health impact and adherence, rather than assessing intervention effects.
Eligible participants were contacted by telephone and invited to take part in the interviews. The recruitment process was carried out by P.M.-G. (PhD, MD, Anthropologist and Medical Specialist in Preventive Medicine, University of Granada), N.C.-I. (PhD, Nurse, Nutritionist and Lecturer, University of Granada), M.D.-L (Nursing phD student, University of Granada) and C.R.-M. (Nursing student, University of Granada).
2.3. Data Collection
Data were gathered between March and May 2023 through 17 individual semi-structured interviews. Each session was conducted in person and lasted approximately 30 to 60 min. The research team comprised two female investigators: N.C.-I., P.M.-G., and one research assistant: C.R.-M. All interviews were conducted at the University of Granada’s Faculty of Medicine (Spain), where participants’ visits during the RCT follow-up were held. The interviewers made a presentation introducing the other researchers to each participant, explaining selection reasons, purpose of the interview, and advising that conversation would be audio-recorded for later transcription ensuring confidentiality. All interviews were audio-recorded, occasionally, recording was stopped at the participants’ request when they felt that some comment was particularly private, or that could be politically incorrect. Records yielded a total of 12.5 h of material for analysis.
A semi-structured interview guide (Supplement S2) with open-ended questions was used to explore participants’ health impact, barriers, and facilitators related to adherence to the Mediterranean lifestyle intervention. This approach facilitated the ‘emic’ perspective [24], minimised researcher bias, and encouraged the emergence of new categories. Interviewers stimulated participants to reflect freely on their participation in the clinical trial and on how they had managed to incorporate dietary and lifestyle recommendations into their everyday routines.
To ensure an open and comfortable atmosphere, participants were informed that there were no right or wrong answers and that their views and experiences were highly valued. During the sessions, one researcher led the discussion, another took field notes documenting non-verbal cues and contextual observations, and the assistant transcribed relevant statements in real time. Immediately after each interview, the team held a brief debriefing meeting to review impressions, discuss data quality, and adjust the interview guide when necessary. Saturation principle was applied to achieve maximum discursive heterogeneity and representativeness. Data collection continued until no new topics of interest emerged, and the information started to become redundant [25].
From a reflexivity standpoint, all the researchers were young women, and N.C.-I., P.M.-G. and M.D.-L. had professional and academic training related to patient care, as well as experience in recruiting and monitoring in multiple studies. In addition, many participants were already familiar with the researchers, as all of them—except C.R.-M.—worked in the setting where the RCT visits and group sessions were carried out. These facts were expected to facilitate rapport and to foster open communication during the interviews. An anthropological perspective was provided by P.M.-G., which contributed to avoiding biomedical bias, and to sustaining more in-depth analytical discussions during the interpretation of the interviews, guided by the gender sensitivity shared among the researchers.
2.4. Theoretical and Analytical Framework
In this qualitative study, sociocultural dimension [26,27], and gender perspectives [28,29,30,31,32,33] were applied across the study design, methodology and analysis for addressing processes influencing participants’ lifestyles and adherence to study recommendations. The conceptual framework of thematic analysis was based on the updated MedDiet pyramid, which offers a more holistic view beyond nutritional recommendations, and emphasised social environment, relationships, and physical activity within a Mediterranean lifestyle [34].
2.5. Data Analysis
The audio records of 17 interviews were transcribed within two days by P.M.-G. and C.R.-M. A thematic analysis was performed collaboratively by the research team (P.M-G., N.C.-I., and C.R.-M.) [35]. Inductive orientation was used to identify themes and categories related to the research topics on participants’ experiences shaping their adherence to the RCT intervention protocol. Data analysis started simultaneously with data collection, using quotes from fieldnotes and researchers’ insights after each interview with a debrief of main topics, comments, and impressions during the conversations. Audio-records of interviews were transcribed within two days using oTranscribe software (https://otranscribe.com/). To ensure truthfulness and data accuracy, transcriptions were carefully checked against the original recording and field notes taken during interviews.
Constant comparison method was used to code collected data, to segment by themes, and to group information into relational category trees [36], as well as to triangulate data analysis among researchers [37]. After an in-depth reading of each transcription, researchers identified categories and subcategories, which were grouped into main themes according to topic guide and key points in the fieldnotes. All themes, categories, subcategories, and illustrative verbatims were shared among researchers to add, modify, and regroup them, and to include or relocate quotes after each transcription analysis. Disagreements were solved though discussion among these three researchers to choose the categories that best suited the purpose and framework of the study. The emergence of each theme and category was interpreted according to sociodemographic characteristics of participants (i.e., gender, age, civil status, occupation, etc.) to observe differences in their health perceptions and facilitators or barriers to adherence.
2.6. Ethical Statement
The study protocol complied with the principles of the Declaration of Helsinki and was approved by the Provincial Ethics Committee of Granada, Spain (Registration number: S1045, 0936_N-22, approval date: 28 April 2023). All participants provided written informed consent. Data protection was ensured in accordance with Organic Law 3/2018 on Personal Data Protection and Regulation (EU) 2016/679 of the European Parliament and of the Council.
3. Results
3.1. Sociodemographic Characteristics of Participants
Among 296 subjects contacted, 17 agreed to participate (10 men and 7 women) (Figure 1). The mean age was 67.4 ± 5.7 years (range 60–81). Most participants were married (n = 15, 88.2%), retired (n = 16, 94.1%), and resided in urban areas (n = 13, 76.5%), sharing their homes with an average of 2.4 cohabitants. Educational attainment was mainly medium (n = 6, 35.3%) or low (n = 7, 41.2%). Regarding their allocation in the clinical trial, 10 participants (58.9%) belonged to the intervention group and 7 (41.2%) to the control group. Concerning outcomes achieved during participation in the randomised trial, 6 participants (35.3%) reported a weight reduction greater than 5%, while two-thirds (64.7%) showed an improvement in MedDiet adherence after six months of follow-up. Most participants (n = 13, 76.5%) attended at least 75% of scheduled follow-up visits. Individuals with higher visit attendance generally achieved greater dietary adherence and weight loss, particularly those assigned to the intervention arm (Table 1).
3.2. Thematic Analysis of Interviews
Main themes identified were: (1) experiences of enrollment in MedDiet lifestyle trial study; (2) perceived health impact; (3) Facilitators to adherence with the MedDiet and lifestyle recommendations; (4) Barriers to adherence with the MedDiet and lifestyle recommendations; and (5) opinions and suggestions for improving the intervention.
4. Experiences of Enrollment in a MedDiet Lifestyle Trial Study
4.1. Motivations for Participation
Participants expressed multiple reasons for joining the study, mainly related to health improvement and interest in learning healthier eating habits (Table S1). A recurring motivation was the desire to increase nutritional knowledge: “Being taught to eat well, because we don’t know how to eat well.” (08399, Woman, 60 years). This intention was closely linked to a sense of self-control and personal growth: “…improving one’s conscience in terms of diet, exercise and leading a healthy life.” (08382, Man, 61 year). A sense of social responsibility and commitment to scientific research was also mentioned: “…if this is a valuable study, first for some people who might fry their eggs with butter, so that they learn not to do so.” (08341, Woman, 63 years). Some women expressed a protective, almost maternal attitude toward the research team, as reflected in: “The first point is collaboration with young people,…so that girls can get scholarships and…have a future.” (08341, Woman, 63 years). Expectations of receiving advice for age-related health concerns were also raised: “We need help…to cope with…all the problems that arise at our age and we…don’t know how to solve them.” (08181, Woman, 70 years). For some men, participation also carried cultural meaning and pride in promoting Mediterranean traditions: “…if we’re going to promote olive oil and the Mediterranean diet, then let’s export the way of life as well.” (08382 Man, 61 years). However, not all participants were initially aware of the study’s scope or aims, as noted by one woman: “I had no idea what it was.” (08093, Woman, 67 years). In a few cases, the long duration of the programme discouraged participation, although satisfaction increased over time (Table S1).
4.2. Challenges and Personal Goals
At enrollment, many participants reported having no clear personal objectives, often delegating responsibility for outcomes to the research team (Table S1). Still, some viewed participation as a challenge in discipline and perseverance: “Personally, to carry it out…I’m working on it.” (08200, Woman, 67 years). For others, particularly women, the main goal was maintaining health and autonomy to avoid depending on relatives: “I just want to be healthy and be able to…take care of myself…I don’t want to burden my daughters.” (08381, Woman, 76 years). A few participants expressed frustration after previous unsuccessful weight-loss attempts: “I saw this as a dream…because I was about twenty-something kilos overweight.” (08200, Woman, 67 years). Conversely, others acknowledged abandoning their initial weight-loss objectives during follow-up: “At first, I set myself some goals, but then I didn’t set myself anymore.” (08212, Man, 70 years).
5. Perceived Health Impact
5.1. High Quality of Life
Many women described their well-being holistically, emphasising autonomy, social activity, and self-fulfilment: “Psychologically, I also feel good, fulfilled with what I am doing with my grandchildren, with the activity. I do not feel like a useless woman…, I help as much as I can.” (08200, Woman, 67 years) (Table 2). Participants frequently attributed improved health and vitality to their involvement in the study: “Thanks to [study], I am alive.” (08032, Man, 81 years); “Coming here has been the best thing that has ever happened to me.” (08093, Woman, 67 years). They also emphasised enhanced self-esteem and autonomy: “The self-esteem of being myself, of preparing my own food…Teaching me to take care of myself…” (08093, Woman, 67 years). Several women valued improvements in physical appearance and self-image: “I feel young, I feel better, lighter, I am not flabby, I can wear clothes that I like, and I feel good.” (08200, Woman, 67 years). Some reported notable physical recovery: “I was on a waiting list for a prosthesis, and I did not have surgery because…I lost weight.” (08032, Man, 81 years). Reduced medication use and closer medical monitoring contributed to their sense of security: “The healthy diet…has balanced my blood pressure and weight very well, and I don’t take pills for cholesterol.” (08200, Woman, 67 years).
5.2. Moderate Quality of Life
Participants with stable chronic conditions aimed to preserve health and functionality: “I feel fine, I have my ailments, but as long as you keep moving with light physical activity and keep yourself under control, that’s it.” (08382, Man, 61 years). Others prioritised independence over aesthetics: “…I have perhaps paid more attention to ensuring that…I do not become useless in being able to walk…[rather] than what figure I had.” (08381, Woman, 76 years) (Table 2).
5.3. Low Quality of Life
A few participants described worsening health and well-being, often associated with disease progression or adverse family circumstances. New cardiovascular diagnoses generated uncertainty and discouragement: “But this year life changed. I have a cardio issue … you start to see yourself as worse off than you really are.” (08212, Man, 70 years). Feelings of loss and depression were also present: “And now I feel useless, I feel depressed because [blindness] has come on almost suddenly.” (08032, Man, 81 years). Social and relational problems further affected their well-being: “[I] was no longer any good for anything, married life [he meant sexual impotence]. I couldn’t do anything.” (08032, Man, 81 years). Several participants also reported sleep problems, family stress, or social isolation affecting adherence and mood (Table 2).
5.4. Health Impact on Relatives and Social Networks
Participants often described themselves as agents of change, transferring acquired health habits to family members and neighbours: “I have tried… to pass on the good that I have received.” (08200, Woman, 67 years) and even reported vicarious benefits: “My daughter has taken advantage of that, my son too, and my neighbors.” (08200, Woman 67 years) (Table 2).
6. Facilitators to Adherence with the Mediterranean Diet and Lifestyle Recommendations
6.1. Nutritional Learning and Behavioural Reinforcement
Participants emphasised that repeated nutritional guidance and individualised feedback strengthened their dietary awareness and confidence to maintain healthy habits (Table 3). Continuous reinforcement through group sessions and follow-up visits facilitated internalisation of key messages: “…you get used to it … because you keep telling us things very repeatedly.” (08212, Man, 70 years). Perceived health improvements, such as weight loss, better mobility, and disease control, acted as strong motivators for sustained adherence: “I did everything exactly as instructed [and]…I noticed the improvement.” (08032, Man, 81 years).
6.2. Supportive Relationship with the Research Team
A close, trust-based relationship with the research team emerged as a key facilitator of adherence. Participants valued the team’s empathy, availability, and personalised attention, which fostered commitment and a sense of belonging: “Everything was attentive, delicate, personal encounters…they helped me so much.” (08200, Woman, 67 years). Group sessions also contributed to emotional well-being and empowerment: “They have taught me to go out and … communicate, move forward…and learn self-esteem, enthusiasm.” (08093, Woman, 67 years). Some participants expressed their intention to maintain healthy habits beyond the study: “Everything you have taught me; I will continue to do. I am not going to say, ‘I have finished studying and I am stopping.’” (08347, Man, 69 years) (Table 3).
6.3. Sense of Responsibility and Social Meaning
Engagement was often reinforced by a sense of moral duty and gratitude for being part of a meaningful scientific initiative: “If I’m here, it’s to participate seriously…I’m doing serious work [in such relevant study].” (08382, Man, 61 years). The perception of contributing to broader social benefit enhanced participants’ motivation to adhere to and complete the programme. As well, meals and daily activities were often ritualised around their closer social network, as partners, friends, or family members, that reinforced adherence to healthy lifestyles: “I usually get together with a group of…friends…” (08027 Woman, 67 years) (Table 3).
7. Barriers to Adherence with the Mediterranean Diet and Lifestyle Recommendations
7.1. Loss of Motivation and Difficulty Sustaining Discipline
Several participants acknowledged inconsistency in maintaining healthy habits. Fatigue, low willpower, and entrenched routines were frequently cited as obstacles: “…my fault is that I don’t follow a strict diet like … my brother [also a participant] did.” (08212, Man, 70 years). The challenge of sustaining dietary effort over time was apparent: “[Losing 4 kg] is very difficult…because that would require an additional effort …, the habits I have incorporated are not enough.” (08241, Man, 60 years) (Table 4).
7.2. Cultural and Emotional Resistance to Change Eating Habits
Men described difficulty abandoning lifelong eating customs and “food addictions”: “It takes a lot of effort, because we’re already addicted … You can’t cut things out immediately … At my age, it’s very difficult to break old habits.” (08212, Man, 70 years). The “carpe diem” mentality associated with aging often weakened motivation: “There comes a time when I’m not going to stop doing what I like.” (08212, Man, 70 years) (Table 4).
7.3. Physical Limitations
Health problems often limited engagement in physical activity and healthy routines (Table 4). Chronic conditions, joint pain, frailty, and apprehension after receiving a diagnosis of severe disease restricted mobility: “I … have a total knee prosthesis, … I can’t walk as fast as I used to walk.” (08212, Man, 70 years). Low public availability of senior-oriented exercise programmes was also mentioned as constraints.
7.4. Gendered Challenges and Relational Barriers
For women, caregiving obligations were a recurrent barrier: “I signed up to do sport…, and I had to cancel [because]… I must look after my grandson.” (08093, Woman, 66 years). Many reported frustration with their partners’ non-compliance, which undermined household adherence: “I call it a problem, gluttony…In fact, he’s put on 20 kilos lately … Now I let it go because it’s his freedom and I’m not going to be like a police officer.” (08200, Woman, 67 years). Lack of partner involvement in sharing physical activity was also reported: “I say [to him]: ‘Let’s go out, let’s join a gym…’ [He answered]: ‘No, because you walk too slowly.” (08181 Woman, 70 years). For some widows, adherence was sustained largely through the research team’s support, suggesting external rather than intrinsic motivation: “Once this research is over, I may not be able to lose weight on my own. (…) I’ll have to prepare myself mentally for … and resign myself to them calling me from time to time.” (08027, Woman, 67 years) (Table 4).
8. Participants’ Opinions and Suggestions for Improving the Intervention
8.1. Overall Satisfaction and Trust in the Research Design
Most participants expressed a high level of satisfaction with the study, describing the experience as positive and well-organized. No substantial changes were suggested, and many perceived the study as exemplary in its planning and implementation: “I can’t find any faults. For me, everything I’ve seen is very, very, very positive…that it’s a real gift, how it’s been planned … very well studied and with experience.” (08200, Woman, 67 years). A generalized attitude of conformity and deference toward researchers emerged, reflecting participants’ confidence in scientific authority and self-perceived lack of expertise to critique methodological aspects: “No, I don’t consider myself competent for that.” (08241, Man, 60 years). The delegation of responsibility to the research team was recurrent: “You will know why it is planned and why certain things are done and so on.” (08200, Woman, 67 years). Conversely, participants often attributed potential shortcomings to themselves rather than to the study: “The only flaw here is that we have it ourselves, that we are very greedy.” (08212, Man, 70 years) (Table S2).
8.2. Unmet Expectations and Perceived Gaps in the Intervention
Despite the overall satisfaction, several participants expressed unmet needs, primarily regarding psychological and communicative dimensions of the intervention. Some expected broader support to address aging-related issues: “I thought we were going to get some help with…age-related problems…, a psychologist… But…this [intervention] has only been about nutrition.” (08181, Woman, 70 years). Others found the technical language used in group sessions difficult to follow: “I find it very technical, which might make it difficult for many people to understand.” (08212, Man, 70 years). Logistical difficulties were also cited, particularly balancing study attendance with family caregiving responsibilities: “What has been difficult for me … has been … when … we had to look after our grandchildren and couldn’t attend some meetings … it made me a little angry (…) But it was something personal.” (08200, Woman, 67 years) (Table S2).
A few participants mentioned limited social interaction among participants: “We see each other at meetings, but that’s all.” (08399, Woman, 60 years). Others requested clearer communication of test results and study findings: “I would prefer that, well, since we’ve been there undergoing so many tests, that they at least tell us something about results … if something serious comes up.” (08181, Woman, 70 years); “What is the basis of this study?” (08181, Woman, 70 years) (Table S2).
9. Discussion
This qualitative study explored older adults’ perceptions of health impacts, barriers, and facilitators to adherence within a long-term MedDiet and lifestyle randomised clinical trial. Semi-structured interviews provided in-depth insights into participants’ experiences after six years of follow-up, allowing for a nuanced interpretation of how behavioural, social, and contextual factors influenced sustained engagement with the intervention. The analysis revealed that adherence was not merely determined by individual willpower or knowledge, but rather by a complex interplay between health perceptions, psychosocial resources, and relational dynamics.
Most participants reported meaningful improvements in health, vitality, and self-esteem, attributing these gains to enhanced adherence to the MedDiet and increased awareness of healthy living. These perceived benefits, mainly highlighted by women, acted as strong motivators for continued engagement, consistent with prior studies linking perceived health improvements to adherence in lifestyle interventions [38,39]. For women, in particular, participation was associated with a sense of empowerment, autonomy, and self-worth, reflecting gendered patterns of health motivation documented in Mediterranean and aging populations [40]. Moreover, the emergence of participants as informal health promoters within their families and communities underscores the social diffusion potential of such interventions [41,42,43]. However, a gradient in perceived health benefits was observed, conditioned by chronic disease burden, physical limitations, and emotional well-being. Participants experiencing illness exacerbation or frailty often reported decreased motivation and a reduced sense of control over their health, which in turn hindered adherence. This aligns with evidence indicating that multimorbidity and psychological distress negatively influence sustained engagement in dietary and physical activity programmes [44].
Adherence facilitators included increased nutritional literacy, internalized behavioural reinforcement, strong social network, and the supportive relationship developed with the research team. Participants frequently cited empathy, individualized attention, and the continuity of professional contact as key enablers of motivation, reflecting the importance of therapeutic alliance and trust-building in long-term behavioural change interventions [45]. The sustained reinforcement of messages during follow-up visits promoted both accountability and a sense of belonging to the study, particularly among women who valued emotional connection as part of their adherence experience. This was consistent with a systematic review on gender differences to engage in clinical trials, which showed that women’s motivation increased when they perceived rapport from research team, and a conductive atmosphere to express themselves and to feel heard [46]. Moreover, the female gender of the research team was specifically valued by women participants in our study, similarly to recent studies that confirm that there were more female participants in cardiovascular disease clinical trials led by female investigators [47,48].
Additionally, participants highlighted the moral significance of contributing to a meaningful scientific endeavour. In turn, meaningful daily activities ritualized around closer social network [49,50] encouraged them to maintain adherence and to achieve weight goals [51]. This sense of collective purpose and social responsibility reinforced their engagement and may represent a culturally embedded dimension of Mediterranean social identity, where participation in research was perceived as a civic and intergenerational contribution.
Despite these positive factors, several barriers to adherence emerged. Fatigue, low motivation, and difficulties sustaining dietary discipline over time were frequent, mirroring findings from other long-term interventions where initial enthusiasm diminishes without ongoing reinforcement [52]. For many men, resistance to changing long-standing eating patterns or adopting restrictive diets reflected cultural attachment to traditional food practices and a “carpe diem” mindset associated with ageing. Women, conversely, emphasised relational and household barriers, particularly the lack of partner support or shared commitment to dietary change, which often undermined adherence efforts within couples. These findings echo previous research showing that spousal dynamics and gender roles significantly shape lifestyle behaviours in older adults with chronic diseases [53,54,55]. Physical limitations due to chronic conditions or injuries, as well as caregiving responsibilities, further constrained both dietary and physical activity adherence. In Mediterranean cultures, where intergenerational caregiving is common, competing family duties, especially among grandmothers, constitute a recognised challenge to health self-management [56].
Strengths and Limitations
This study provides novel qualitative insights into the long-term adherence to a Mediterranean Diet and lifestyle intervention among older adults with metabolic syndrome. Strengths include the in-depth exploration through semi-structured interviews, the use of a gender-sensitive and socio-contextual analytical approach, and the triangulation among multidisciplinary researchers, which enhanced credibility and rigor. The inclusion of participants with diverse backgrounds enriched the findings and reflected real-world variability in adherence behaviours. Nevertheless, the study’s qualitative nature and small sample limit generalizability. Selection bias toward more motivated participants and the post-pandemic context may also have influenced reported behaviours. Despite these limitations, the findings yield valuable implications for designing more sustainable, person-centred Mediterranean lifestyle interventions.
10. Conclusions
This qualitative study elucidated the perceived mechanisms underpinning adherence to a MedDiet-based lifestyle intervention among older adults with MetS. Perceived health improvements, self-efficacy, social engagement, and the relational support of the research team acted as key facilitators, whereas declining motivation, illness burden, and limited partner engagement hindered sustained adherence. These results highlight that adherence extends beyond nutritional compliance, encompassing psychosocial, gendered, and contextual dynamics that shape participants’ capacity for behavioural change.
Future intervention studies should employ tailored, gender-sensitive motivational strategies involving participants’ relatives and social networks to enhance adherence and maximize the impact of lifestyle programmes in aging populations. Moreover, translating these programmes into healthcare settings remains a challenge despite prior implementations in other regions. This process could benefit from training primary care personnel to lead group sessions using a systemic, gender-sensitive approach that actively engages patients and their families, while ensuring job stability to maintain continuity of care and a strong therapeutic alliance. Finally, practical guides and educational materials could be strengthened by including vignettes or scenarios designed from a gender-sensitive perspective to illustrate everyday challenges and opportunities for improving lifestyles.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization World Health Statistics 2025: Monitoring Health for the SD Gs, Sustainable Development Goals WHO Geneva, Switzerland 2025
- 2Noubiap J.J. Nansseu J.R. Lontchi-Yimagou E. Nkeck J.R. Nyaga U.F. Ngouo A.T. Tounouga D.N. Tianyi F.L. Foka A.J. Ndoadoumgue A.L. Geographic Distribution of Metabolic Syndrome and Its Components in the General Adult Population: A Meta-Analysis of Global Data from 28 Million Individuals Diabetes Res. Clin. Pract.202218810992410.1016/j.diabres.2022.10992435584716 · doi ↗ · pubmed ↗
- 3Alberti K.G.M.M. Eckel R.H. Grundy S.M. Zimmet P.Z. Cleeman J.I. Donato K.A. Fruchart J.C. James W.P.T. Loria C.M. Smith S.C. Harmonizing the Metabolic Syndrome: A Joint Interim Statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; And International Association for the Study of Obesity Circulation 2009120164016451980565410.1161/CIRCULAT · doi ↗ · pubmed ↗
- 4Hernández Ruiz de Eguilaz M. Batlle M.A. Martínez de Morentin B. San-Cristóbal R. Pérez-Díez S. Navas-Carretero S. Martínez J.A. Cambios Alimentarios y de Estilo de Vida Como Estrategia En La Prevención Del Síndrome Metabólico y La Diabetes Mellitus Tipo 2: Hitos y Perspectivas An. Sist. Sanit. Navar.2016392692892759995410.23938/ASSN.0267 · doi ↗ · pubmed ↗
- 5Fernandez-Lazaro C.I. Toledo E. Buil-Cosiales P. Salas-SalvadóJ. Corella D. FitóM. Martínez J.A. Alonso-GómezÁ.M. Wärnberg J. Vioque J. Factors Associated with Successful Dietary Changes in an Energy-Reduced Mediterranean Diet Intervention: A Longitudinal Analysis in the PREDIMED-Plus Trial Eur. J. Nutr.2022611457147510.1007/s 00394-021-02697-834846603 PMC 8921156 · doi ↗ · pubmed ↗
- 6Nugent R. Bertram M.Y. Jan S. Niessen L.W. Sassi F. Jamison D.T. Pier E.G. Beaglehole R. Investing in Non-Communicable Disease Prevention and Management to Advance the Sustainable Development Goals Lancet 20183912029203510.1016/S 0140-6736(18)30667-629627167 · doi ↗ · pubmed ↗
- 7Lichtenstein A.H. Appel L.J. Vadiveloo M. Hu F.B. Kris-Etherton P.M. Rebholz C.M. Sacks F.M. Thorndike A.N. Van Horn L. Wylie-Rosett J. 2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement from the American Heart Association Circulation 2021144 E 472E 48710.1161/CIR.000000000000103134724806 · doi ↗ · pubmed ↗
- 8Godos J. ZappalàG. Bernardini S. Giambini I. Bes-Rastrollo M. Martinez-Gonzalez M. Adherence to the Mediterranean Diet Is Inversely Associated with Metabolic Syndrome Occurrence: A Meta-Analysis of Observational Studies Int. J. Food Sci. Nutr.20176813814810.1080/09637486.2016.122190027557591 · doi ↗ · pubmed ↗