“Lost in Transition”: Informational Needs of Sepsis Survivors and Their Relatives Across the Care Trajectory—A Qualitative Study
Frank Vahl, Susanne Ullmann, Lea Draeger, Lena Kannengießer, Mathias W. Pletz, Claudia T. Matthaeus-Kraemer, Carolin Fleischmann-Struzek

TL;DR
Sepsis survivors and their relatives face information gaps across the care journey, needing better communication and resources to manage recovery and long-term effects.
Contribution
This study identifies phase-specific informational needs and preferred formats for sepsis survivors and relatives, offering actionable insights for healthcare providers.
Findings
Relatives need timely, clear, and empathetic communication during the ICU phase.
Survivors and relatives experience an 'information vacuum' after discharge, lacking guidance on long-term effects and rehabilitation.
Participants desired peer support and repeated conversations with healthcare professionals, alongside trusted online and printed resources.
Abstract
Background/Objectives: Sepsis survivors frequently experience long-term complications known as Post-Sepsis Syndrome. Many survivors and their relatives express ongoing dissatisfaction with the quality and accessibility of health information. Yet the specific informational needs and preferred formats remain insufficiently defined. To identify the informational needs of sepsis survivors and their relatives across different stages of illness and recovery. Methods: This qualitative study, conducted within the AVENIR project, included semi-structured telephone interviews with 12 survivors and 6 relatives in Germany. Interviews were transcribed verbatim and analyzed using qualitative content analysis according to Mayring. Results: Eighteen interviews highlighted phase-specific gaps in information. Relatives reported urgent needs for timely, comprehensible and empathetic communication during…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
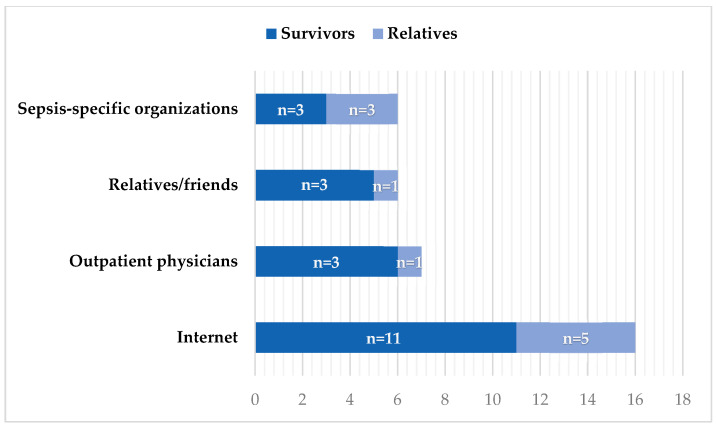 Figure 1
Figure 1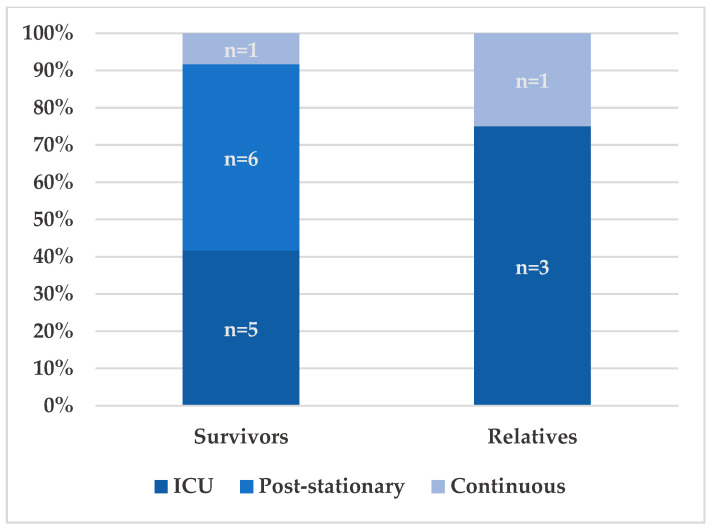 Figure 2
Figure 2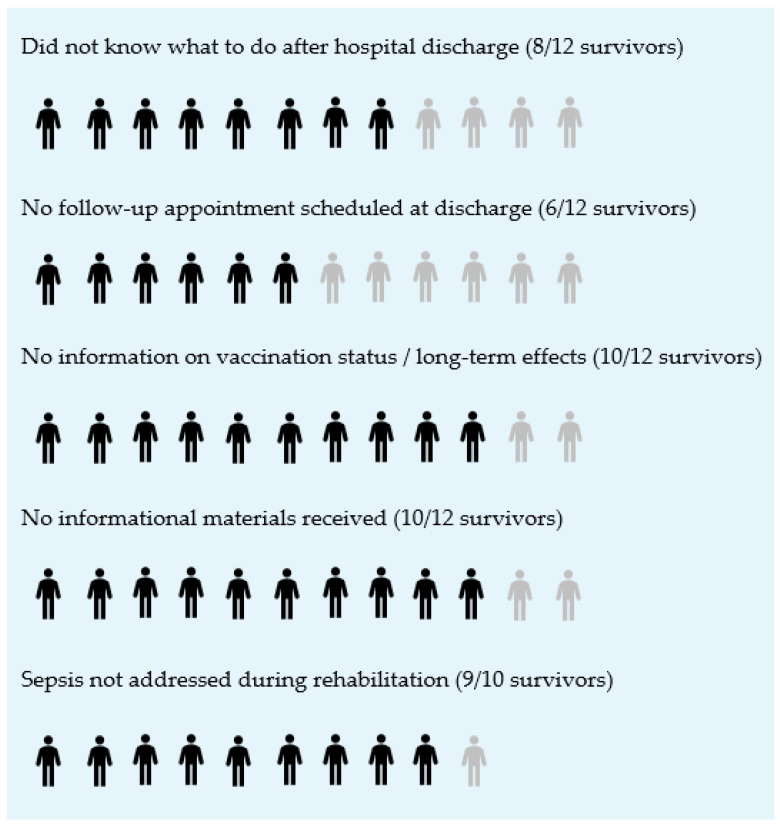 Figure 3
Figure 3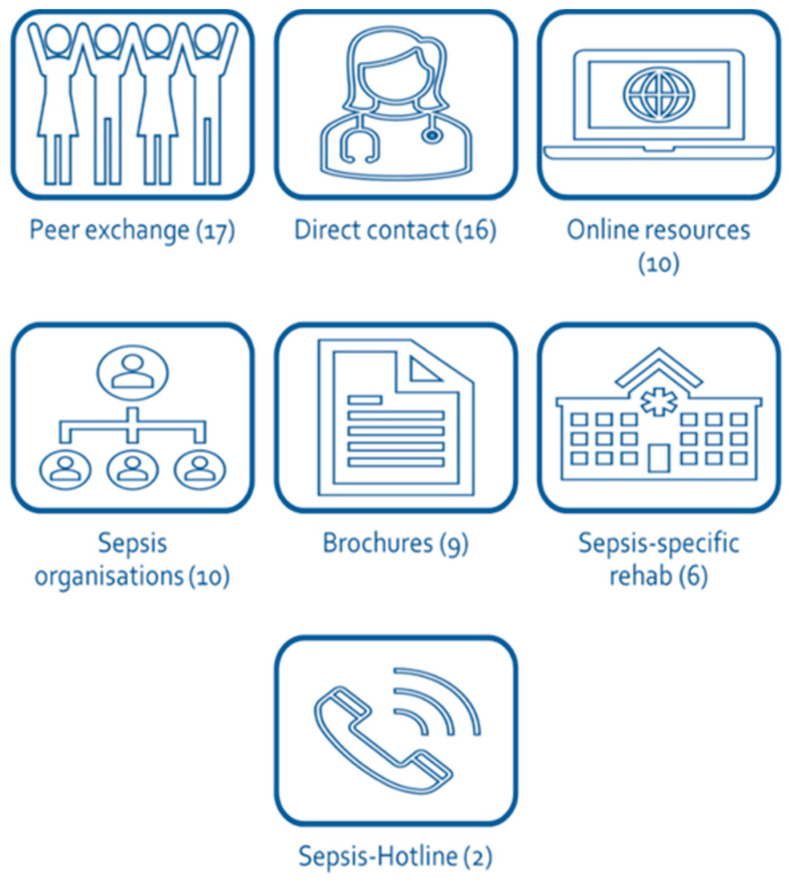 Figure 4
Figure 4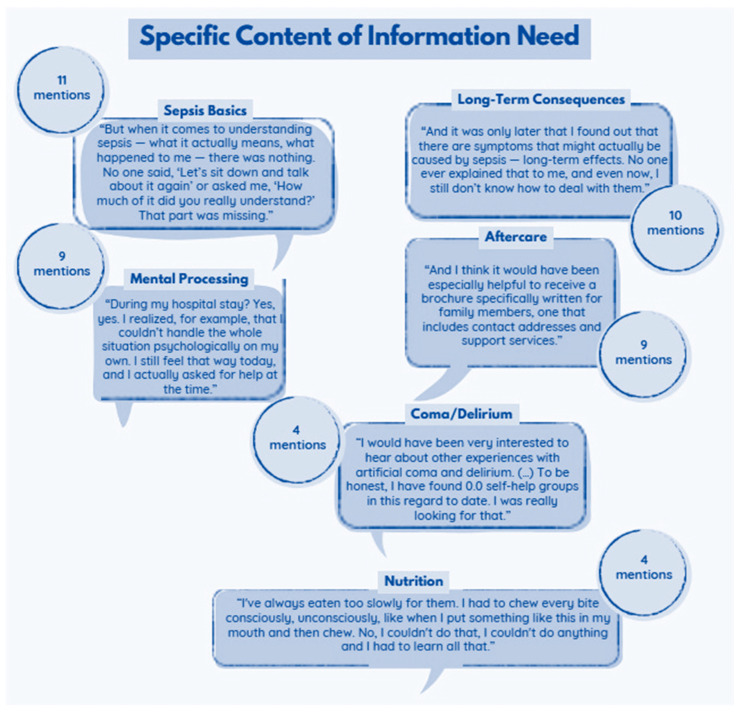 Figure 5
Figure 5- —German Innovations Fund of the Federal Joint Committee
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Sepsis Diagnosis and Treatment · Family and Patient Care in Intensive Care Units
1. Introduction
Sepsis is a life-threatening condition caused by a dysregulated host response to infection. It remains a major global contributor to morbidity and mortality. According to estimates from the Global Burden of Disease Study, approximately 49 million people develop sepsis each year, and around 11 million die—representing nearly one in five deaths worldwide [1]. In Germany, sepsis also poses a substantial challenge to the healthcare system. An analysis of national hospital discharge data reported an incidence of 158 per 100,000 inhabitants, with an in-hospital mortality of 41.7% among identified cases. However, due to the low sensitivity of health claims data, true incidence is likely underestimated and mortality overestimated [2].
At the same time, improved intensive care has increased survival, but many survivors experience persistent impairments. A significant proportion develop Post-Sepsis Syndrome (PSS), which includes cognitive dysfunction, physical weakness, fatigue, anxiety, depression, and a high risk of newly acquired dependency on long-term care [3,4,5]. These sequelae overlap with symptoms of Post-Intensive Care Syndrome (PICS) and may last for months or years [6,7,8].
Despite the growing evidence on long-term consequences, structured aftercare remains insufficient in many settings [9,10]. Studies show that sepsis survivors often leave the hospital without clear follow-up plans, rehabilitative referrals, or targeted information about possible long-term effects [11,12,13]. Relatives also play a central role. They frequently take on informal caregiving responsibilities yet are rarely integrated into communication processes. Many relatives report emotional strain, uncertainty and a lack of guidance during and after hospitalization [14].
Timely and relevant information can help patients and families cope with the illness and its consequences. However, informational needs change across the disease trajectory, from the acute treatment phase to long-term recovery. Several studies document substantial sepsis-specific information deficits [15,16,17]. Many affected individuals are unfamiliar with what sepsis is, how it develops, and which long-term consequences may arise [18]. Sepsis-related topics are often missing from available materials, and many survivors receive no written information after discharge. Despite these recurring observations, there has been no systematic investigation into which specific information is lacking, when it is most urgently needed, and how it should be effectively tailored to survivors and relatives. This gap continues to limit the development of patient-centered communication strategies.
Qualitative research is well suited to identify these unmet needs because it provides deep insight into lived experiences of care. Building on this approach, the present study examines the informational needs of sepsis survivors and their relatives across different stages of illness and recovery. The study aims to identify shortcomings in current communication practices and to derive recommendations for needs-oriented information tools. It focuses not only on content and timing of information but also on preferred communication formats.
This work further expands the literature by mapping informational needs across multiple phases of the sepsis trajectory and by distinguishing the perspectives of survivors and relatives. By describing how readiness to receive and process information changes over time and differs between roles, it provides phase- and role-specific insights that may support more tailored communication strategies.
2. Materials and Methods
2.1. Background of the Study
This exploratory study is part of the AVENIR project (FKZ 01VSF21031), which aims to improve understanding of medical care and subjective experiences before, during, and after sepsis [19]. The project seeks to inform recommendations for organizing follow-up care and developing patient-centered informational materials, with active involvement of affected individuals. The study was pre-registered (DRKS00031302) and approved by the Jena University Hospital institutional review board (2023-2992-Daten).
2.2. Participants
Participants were recruited nationwide through social media advertisements, the sepsis foundation’s advisory network and flyers distributed in the post-intensive care unit of the Charité University Medicine Berlin. Although one recruitment pathway involved a single university hospital, participants themselves came from different regions across Germany. Eligibility criteria were age 18 years or older, fluency in German, and a sepsis diagnosis within the past five years. Both sepsis survivors and relatives who voluntarily agreed to participate were included. Recruitment continued until conceptual saturation was reached (see Section 2.5 and Section 3.1).
2.3. Data Acquisition
Data were collected through semi-structured telephone interviews with sepsis survivors and/or their relatives between May and November 2023. The interviews explored participants’ experiences with receiving a sepsis diagnosis and the communication of and supply with relevant medical information throughout the course of illness and recovery.
2.4. Expert Interviews: Characteristics and Setting
A semi-structured interview guide was used to explore core themes including general understanding of sepsis, experiences during hospitalization and communication with healthcare professionals, discharge and transitional care, rehabilitation and follow-up, initial diagnosis and communication, knowledge of sepsis before and after illness, psychological and social consequences, prevention and relapse, and moments of greatest informational need (Table 1).
All interviews were conducted via telephone by a trained final-year medical student (FV), under the supervision of an experienced social scientist (CTMK, M.A. in Educational Science, Psychology, and Sociology). CTMK has extensive expertise in conducting and analyzing qualitative interviews in healthcare and quality improvement settings. There was no prior relationship between interviewer and participants. Interviewees were informed in advance about the interviewer’s background and role. The interviews were conducted by telephone in a private setting with only the interviewer, the participant, and—in a few cases—accompanying relatives present.
2.5. Expert Interviews: Data Analysis
2.5.1. Analytical Approach
All interviews were audio-recorded and transcribed verbatim. Analysis followed qualitative content analysis, a systematic and rule-governed method of text interpretation [20]. The analytical process comprised three steps:
- Open coding of relevant text segments,
- Development of thematic categories, and
- Abstraction into overarching core categories.
2.5.2. Assessment of Saturation
We monitored saturation throughout the analysis by assessing whether additional interviews contributed new conceptual insights. Because the study aimed to understand informational needs across the full sepsis trajectory, we assessed saturation for the dataset as a whole rather than for survivors and relatives separately. We applied the concept of conceptual saturation, meaning that no new themes, meaning units, or dimensions emerged. After saturation was reached, three confirmatory interviews were conducted to test the stability of the category system. These interviews did not add new concepts, and recruitment was therefore concluded.
2.5.3. Reflexivity and Coding Validation
Reflexivity was maintained throughout data collection and analysis. The interviewer (FV) and the supervising social scientist (CTMK) engaged in regular discussions about potential influences of their professional backgrounds, expectations, or emotional engagement. Coding reliability was strengthened through iterative review: the interviewer conducted initial coding, and coding decisions were then refined through discussion until consensus was reached. As is standard in qualitative research, no statistical interrater metrics were calculated.
2.5.4. Data Management
Data were managed and analyzed using MAXQDA (version 24; VERBI Software, Berlin, Germany). Definitions of categories and selected original quotes are provided in Electronic Supplement S1. The study methods are reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) checklist [21].
3. Results
3.1. Interview and Participant Characteristics
In total, 18 interviews were included (12 survivors, 6 relatives). The median interview duration was 37 min, resulting in a total interview time of approximately 11 h and 15 min. Conceptual saturation was reached after 15 interviews. We then conducted three additional interviews to confirm the stability of the category system; these interviews did not introduce new concepts.
The median age of survivors and relatives was 53 years. All 12 survivors had received intensive care unit (ICU) treatment, and 10 had participated in post-ICU rehabilitation. The six relatives described providing essential emotional and practical support during hospitalization and recovery.
3.2. Diagnoses Communication
Five survivors said they were informed about the diagnosis by a physician, four by relatives, and two through their own review of medical records. Among relatives, five of six learned about the sepsis diagnosis from a physician. Participants also reported considerable variation in when and where they received this information. Three relatives and seven survivors were informed during the ICU stay, two participants received the information before admission, and six could not recall the timing. Among survivors, eight learned about the diagnosis in the ICU, one before admission, and three could not remember. Among relatives, two were informed in the ICU, one before admission, and three could not recall.
After learning about the diagnosis, most participants sought additional information on their own. Figure 1 shows the main information sources used. Experiences with online information varied widely: some described feeling overwhelmed (“There’s a lot on the internet, but it’s overwhelming and you don’t know what really applies to you.”), while others highlighted the value of online forums: “What helped me most was a forum. That’s where I got concrete answers.”
3.3. Timing of Informational Needs
Informational needs changed over time and differed between survivors and relatives. Figure 2 illustrates when these needs arose during and after hospitalization. A strong demand for information occurred during the hospital stay, especially in the ICU and primarily among relatives. At this stage, the severity of the illness became clear, and relatives described urgent needs for understandable updates and support in situations of decision pressure: “You are the spouse, you have to decide now.” Another added: “You are left completely in the dark.” Several also criticized the lack of clear explanations and written materials: “I would have liked to know what sepsis actually is.”/“You’re not prepared. You don’t know what to expect.”
Survivors described a different pattern. Many said they were unable to process information during the acute phase because they felt cognitively and emotionally overwhelmed in the ICU and early rehabilitation. They began to seek orientation after physical stabilization: “And at some point at home. Then I had a look at all the documents. After the rehab, actually. Yes, exactly when my health was better, when I was a bit stronger, no longer so weak.”
Informational needs remained high after discharge for both groups. Six survivors described a continued need for guidance on long-term effects, rehabilitation, and follow-up care. Two participants (one survivor, one relative) reported ongoing needs well beyond the acute phase. Survivors frequently described receiving little or no information when leaving the hospital. Many did not know what steps to take because no clear guidance had been provided (mentions: 8/12). About half had no scheduled follow-up appointment (mentions: 6/12), and most reported not receiving information on long-term consequences, vaccination recommendations, or continuing care needs (mentions: 10/12). Several summarized this period as an “information vacuum”: “Yes, of course, at first I didn’t know what to do next.”/“No, nothing at all. Nothing was planned at all.”.]
3.4. Long-Term Burden on Relatives
Over the longer term, many relatives assumed extensive coordination, caregiving, and emotional responsibilities without feeling adequately informed. One relative described: “My mother can’t do anything anymore. I have to take care of everything. And I still don’t really understand what sepsis actually did to her.” These accounts highlight a sustained informational and emotional burden that persisted well beyond the acute episode. Relatives described intense distress and a sense of being left alone: “I cried in the car every day before I went to the rehabilitation clinic. Every day. I didn’t know how I was going to cope with it all.”/“It was like another world. You were completely left alone.” Insufficient information about the illness and its consequences contributed to prolonged feelings of helplessness and isolation.
3.5. Informational Gaps and Post-Discharge Management
Many interviewees reported that they had not received any informational materials during their hospital stay (13 of 18; 9 survivors, 4 relatives). As shown in Figure 3, survivors in particular described substantial gaps in post-discharge management and information. These included uncertainty about required care, the absence of scheduled follow-up appointments, limited communication about vaccinations and long-term consequences, a lack of written materials, and no sepsis-specific discussions during rehabilitation.
3.6. Preferences for Information Delivery and Content
Participants expressed consistent preferences across interviews for how information should be delivered. Peer support was the most valued format. Many also emphasized the importance of direct, personal conversations with healthcare professionals. Trusted online resources such as those provided by the Sepsis Foundation and printed materials were viewed as helpful, especially references during recovery. Several interviewees additionally suggested integrating sepsis-focused education into rehabilitation programs and establishing or expanding a dedicated hotline for sepsis-related questions. As shown in Figure 4, these preferences reflect a strong desire for accessible, trustworthy, and personalized information pathways.
The content participants requested extended well beyond the acute illness. They wanted information about long-term risks, persistent symptoms, and strategies for day-to-day coping. One survivor noted: “And it was only later that I found out that there are symptoms that might actually be caused by sepsis—long-term effects. No one ever explained that to me, and even now, I still don’t know how to deal with them.” Another participant highlighted the absence of basic orientation: “But when it comes to understanding sepsis—what it actually means, what happened to me—there was nothing.” Figure 5 provides an overview of these informational needs.
Participants frequently requested basic knowledge about sepsis: what it is, how it develops, and why it is life-threatening. Many also wanted information about long-term effects, including what to expect after discharge and how symptoms may evolve. A substantial group emphasized psychological consequences and asked for clear explanations of possible emotional and mental health changes. Requests for navigation support were similarly frequent, such as information on whom to contact, how to access services, and where to find peer support. Some participants also sought explanations of coma- or delirium-related cognitive problems and practical advice on nutrition during recovery.
4. Discussion
This study describes a phase- and role-specific pattern of informational needs among sepsis survivors and their relatives. During the acute phase, particularly ICU, relatives reported an urgent need for timely, comprehensible, and empathetic updates. Survivors, in contrast, often felt unable to process information during this time and described seeking orientation only after physical and cognitive stabilization. Across care transitions, many participants reported an information vacuum after discharge, including unclear responsibilities, absent or insufficient follow-up-communication, and limited guidance on long-term consequences, vaccinations, or ongoing care. Sepsis-specific information in rehabilitation was also described as rare. Preferred formats included peer support and direct conversations with clinicians, supplemented by trusted online resources and written materials. Desired content ranged from basic explanation of sepsis to practical strategies for coping with long-term physical and psychological sequelae and navigating support services.
Overall, the findings are consistent with previous qualitative studies on sepsis survivorship. Gallop et al. described low awareness of the diagnosis, difficulties accessing appropriate providers, and persistent caregiver burden—patterns that were also reflected in our interviews [14]. Similarly, research on families of critically ill patients highlights acute informational needs, high uncertainty, and the value of repeated and structured communication, while survivors’ own ability to engage with information often re-emerges only after hospital discharge [22,23,24,25]. Evidence from the PICS and post-sepsis literature further documents long-term cognitive, psychological, and physical sequelae including cognitive impairment, anxiety/depression, fatigue, and disability, which helps explain why survivors in our interviews sought orientation on long-term effects and day-to-day coping [4,6,7,8,10,26,27,28].
The gaps described at the transition out of hospital mirror previous findings that ICU discharge summaries often lack the detail required for effective post-ICU care [11]. “Lost in transition” patterns at care interfaces have been observed in other settings as well [29]. Narrative review emphasizes the central role of general practitioners in post-ICU recovery and the importance of structured communication from the hospital to primary care [30]. Similarly to our interviews, studies on rehabilitation highlight inconsistent sepsis-specific content and variable access to aftercare services [10,13,17,31].
Preferences for peer support and for direct communication with clinicians align with evidence that ICU-recovery and peer-support programs can enhance orientation, self-efficacy, and emotional well-being, while clinician encounters can help translate general recommendations into individual guidance [16,24,32].
4.1. Potential Implications for Practice
The findings support a phase-specific and role-sensitive approach to information delivery. In the ICU, short and scheduled updates for relatives using clear language and addressing status, uncertainty, and immediate steps may reduce decisional strain [22,23,25]. At discharge, a structured information package that includes follow-up appointments, explanations of long-term effects and vaccination recommendations, and a named contact person could address the most pressing gaps [11,29,30]. During rehabilitation and early recovery, sepsis-specific educational modules (fatigue management, cognitive strategies, mental health, reinfection concerns), peer-support offers, and reliable online or printed resources may match survivors’ delayed readiness and practical needs [13,17,24,32]. Early transfer of concise, action-oriented information to primary care can also support coordinated recovery close to home [30]. These steps frame information as a central component of care quality and correspond to calls for structured survivorship and aftercare services for sepsis survivors [9,10,28].
4.2. Why Information Remains Hard to Obtain: Provider Knowledge and System Gaps
Our interviews indicate that informational gaps arise not only at care transitions but also from limited preparedness and confidence among healthcare professionals regarding sepsis-specific knowledge, particularly on long-term sequelae, prevention, and follow-up pathways. A scoping review highlights substantial variation in knowledge and awareness among patients, the general public and healthcare professionals, which complicates consistent counseling [18]. Evidence on information-seeking further indicates that how information is communicated is critical in contexts where time constraints and limited sepsis-specific expertise restrict counseling: a randomized trial demonstrated that text-based and graphical formats differentially influence informed choice [33], and multimodal campaigns offer models for targeted education [34]. Population surveys and digital-trace studies also reveal inconsistent public awareness and fluctuating information demand. In the absence of structured, sepsis-specific follow-up information within the healthcare system, this helps explain why many survivors and relatives rely on general internet sources yet struggle to identify specific and trustworthy information [18,35,36,37]. In the German context, pathway studies describe communication barriers, handover problems, time constraints, and low prioritization of sepsis routines, all of which impede reliable information transfer [38,39]. Non-standardized discharge summaries and weak linkage to primary care leave survivors without a clear point of contact, extending the post-discharge information vacuum reported in our interviews [11,29,30]. Within rehabilitation, programs often focus on generic physical recovery, while sepsis-specific education remains limited [10,13,17]. Addressing these issues may require improved education for healthcare professionals on sepsis survivorship and standardized handover processes that clarify whom to contact, when, and for which concerns—ensuring that information is accessible when patients and families are ready to receive it.
Furthermore, a notable characteristic of our sample is its comparatively young age. This may reflect the recruitment strategy, which relied on digital channels and a university hospital outpatient clinic. These pathways may preferentially engage younger and more health-active survivors. Older survivors, who represent a substantial proportion of the sepsis population and often have high multimorbidity and greater functional limitations, may therefore be underrepresented. This age distribution should be taken into account when interpreting the types of informational needs and preferred formats described here.
Finally, these findings should be interpreted as exploratory and reflect patterns observed within this qualitative sample rather than generalizable conclusions for all sepsis survivors and relatives.
5. Limitations
This study has several limitations. First, the sample size is small and the sample is not representative; therefore, the findings cannot be generalized to all sepsis survivors or their relatives. This constraint is inherent to the qualitative, exploratory design, which aims to generate in-depth insights rather than generalizable estimates.
Second, recruitment occurred largely through digital platforms and a university hospital outpatient clinic. This may have introduced a bias toward younger, more digitally literate, and more health-engaged individuals, potentially underrepresenting older survivors, who constitute a substantial proportion of the sepsis population and often experience higher multimorbidity and functional limitations. This demographic pattern may limit the transferability of the findings to older or more clinically complex groups.
Third, the study relied on retrospective self-reporting, which may be affected by recall bias, especially among survivors who experienced delirium or cognitive dysfunction. Survivors with more severe cognitive impairment were likely underrepresented because they may be less able to participate in interviews despite potentially high informational needs. Only limited clinical information was collected (age, ICU treatment, rehabilitation), and no granular clinical variables such as illness severity, organ dysfunction, comorbidities, delirium, mechanical ventilation, or length of ICU stay were available. As a result, findings cannot be contextualized across different clinical trajectories. In addition, we did not systematically collect sociodemographic characteristics such as educational level, employment status, or migration background, which limits the ability to assess variation across socioeconomic or cultural groups.
Fourth, although the study included both survivors and relatives, data saturation was assessed across the dataset as a whole and not separately for these two groups. Given that survivors and relatives may differ substantially in their perspectives, informational needs, and illness experiences, this approach may have obscured group-specific nuances. In a future study, saturation should therefore be assessed separately for survivors and relatives to allow for a more differentiated and methodologically rigorous analysis.
Fifth, we did not systematically distinguish between care settings (ICU, general ward, rehabilitation) in the analysis. Although participants described experiences across these settings, the study was not designed to generate setting-specific comparisons, which limits conclusions about differences in informational needs across environments.
Sixth, triangulation occurred within the research team but did not include multiple data sources, thereby narrowing methodological breadth.
Seventh, as the study was conducted within the German healthcare system, differences in structure and organization in other countries may limit international transferability.
Taken together, these limitations substantially restrict transferability and underscore that the results primarily inform hypothesis generation and future research.
6. Conclusions
This study indicates that participants reported gaps in informational support that affect sepsis survivors and their relatives across the illness and recovery trajectory. These gaps—from limited communication during the acute phase to insufficient guidance on long-term follow-up—may hinder recovery and contribute to prolonged physical, cognitive, and emotional challenges. Addressing them requires timely, accessible, and phase-specific information strategies.
Based on the findings, formats that support structured discharge planning, high-quality and tailored educational materials, and opportunities for peer support may help reduce uncertainty and strengthen coping in survivors and families. By mapping how informational needs differ between survivors and relatives and how they evolve across phases of care, the study provides phase- and role-specific insights that can inform the development of future follow-up structures and information tools. Accordingly, the conclusions drawn from this study are intended to inform understanding of informational needs rather than to define their prevalence or distribution across survivor populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rudd K.E. Johnson S.C. Agesa K.M. Shackelford K.A. Tsoi D. Kievlan D.R. Colombara D.V. Ikuta K.S. Kissoon N. Finfer S. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study Lancet 202039520021110.1016/S 0140-6736(19)32989-731954465 PMC 6970225 · doi ↗ · pubmed ↗
- 2Fleischmann-Struzek C. Schwarzkopf D. Reinhart K. Sepsis incidence in Germany and worldwide: Current knowledge and limitations of research using health claims data Med. Klin. Intensivmed. Notfmed.202211726426810.1007/s 00063-021-00777-533507316 PMC 7841759 · doi ↗ · pubmed ↗
- 3Fleischmann-Struzek C. Ditscheid B. Rose N. Spoden M. Wedekind L. Schlattmann P. Günster C. Reinhart K. Hartog C.S. Freytag A. Return to work after sepsis—A German population-based health claims study Front. Med.202310118780910.3389/fmed.2023.1187809 PMC 1024844937305145 · doi ↗ · pubmed ↗
- 4Iwashyna T.J. Ely E.W. Smith D.M. Langa K.M. Long-term Cognitive Impairment and Functional Disability Among Survivors of Severe Sepsis JAMA 20103041787179410.1001/jama.2010.155320978258 PMC 3345288 · doi ↗ · pubmed ↗
- 5Sell S. Fleischmann-Struzek C. Spoden M. Rosendahl J. Mental health in the first year after ICU-treated sepsis: Analysis of administrative diagnoses in German health claims data Gen. Hosp. Psychiatry 20259310911510.1016/j.genhosppsych.2025.02.00139923305 · doi ↗ · pubmed ↗
- 6Gupta L. Subair M.N. Munjal J. Singh B. Bansal V. Gupta V. Jain R. Beyond survival: Understanding post-intensive care syndrome Acute Crit. Care 20243922623310.4266/acc.2023.0115838863353 PMC 11167423 · doi ↗ · pubmed ↗
- 7Inoue S. Nakanishi N. Sugiyama J. Moriyama N. Miyazaki Y. Sugimoto T. Fujinami Y. Ono Y. Kotani J. Prevalence and Long-Term Prognosis of Post-Intensive Care Syndrome after Sepsis: A Single-Center Prospective Observational Study J. Clin. Med.202211525710.3390/jcm 1118525736142904 PMC 9505847 · doi ↗ · pubmed ↗
- 8Prescott H.C. Angus D.C. Enhancing Recovery From Sepsis: A Review JAMA 2018319627510.1001/jama.2017.1768729297082 PMC 5839473 · doi ↗ · pubmed ↗