Calcification of the Internal Carotid Artery and Its Influence on the Severity of Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage
Adrian Engel, Laurèl Rauschenbach, Argtim Rexhepi, Meltem Gümüs, Christoph Rieß, Jan Rodemerk, Li Song, Yan Li, Börge Schmidt, Yahya Ahmadipour, Philipp Dammann, Marvin Darkwah Oppong, Ulrich Sure, Ramazan Jabbarli

TL;DR
This study finds that calcification in the carotid artery may protect against cerebral vasospasm but is linked to worse outcomes in brain aneurysm patients.
Contribution
The study identifies carotid siphon calcification as a novel protective factor against cerebral vasospasm and a risk factor for poor functional recovery.
Findings
CSC is an independent predictor of reduced angiographic cerebral vasospasm severity and delayed ischemic neurological deficit.
Higher levels of CSC correlate with worse 6-month functional outcomes in aneurysmal subarachnoid hemorrhage patients.
CSC does not significantly affect transcranial Doppler-measured cerebral vasospasm presence or severity.
Abstract
Background/Objectives: Cerebral vasospasm (CV) is a serious complication of aneurysmal subarachnoid hemorrhage (aSAH). Carotid siphon calcification (CSC) has been associated with a reduced risk of CV. This study investigates the influence of CSC on the clinical and radiographic severity of CV and functional outcome of aSAH. Methods: A total of 475 patients with aSAH treated at the University Hospital Essen (2008–2016) were analyzed retrospectively. CSC was assessed using the Woodcock score. Study endpoints were the CV severity in digital subtraction angiography, presence of CV in transcranial Doppler (TCD) ultra-sonography, occurrence of delayed ischemic neurological deficit (DIND) and the functional outcome at 6 months measured with the modified Rankin scale. Results: CSC was confirmed as an independent predictor for the occurrence (aOR 0.76; 95% CI 0.60–0.97; p = 0.025) and severity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
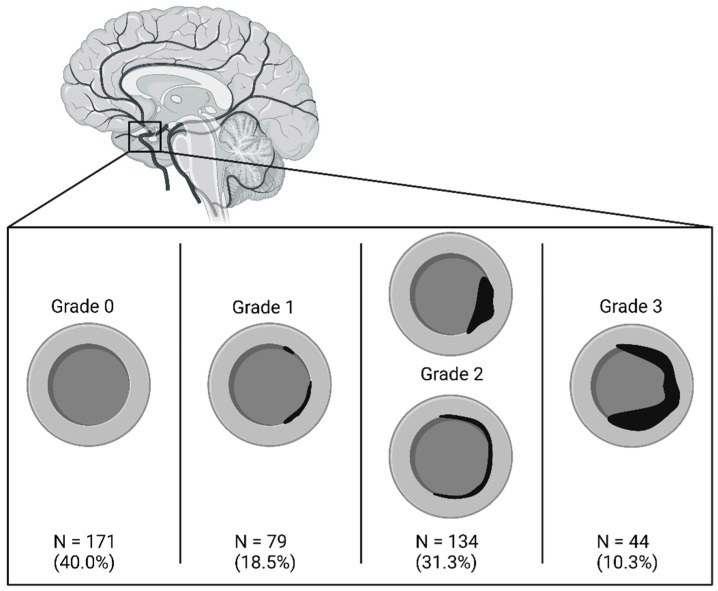 Figure 1
Figure 1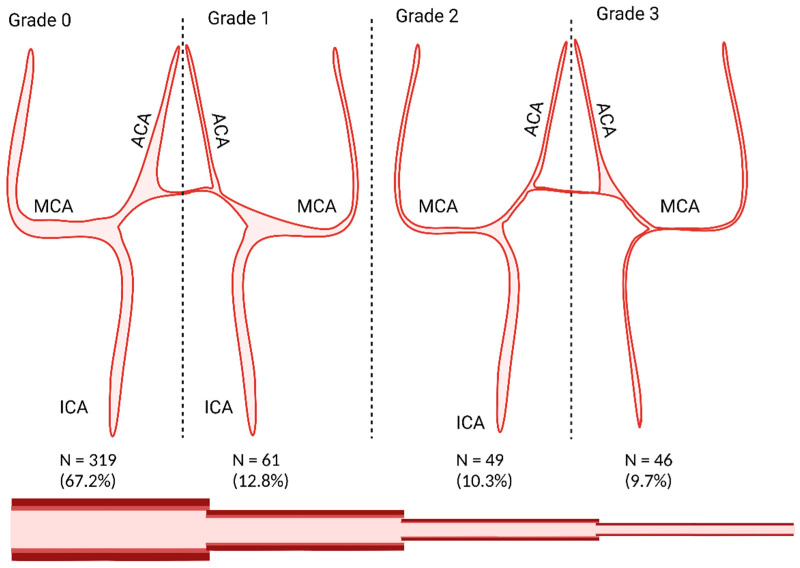 Figure 2
Figure 2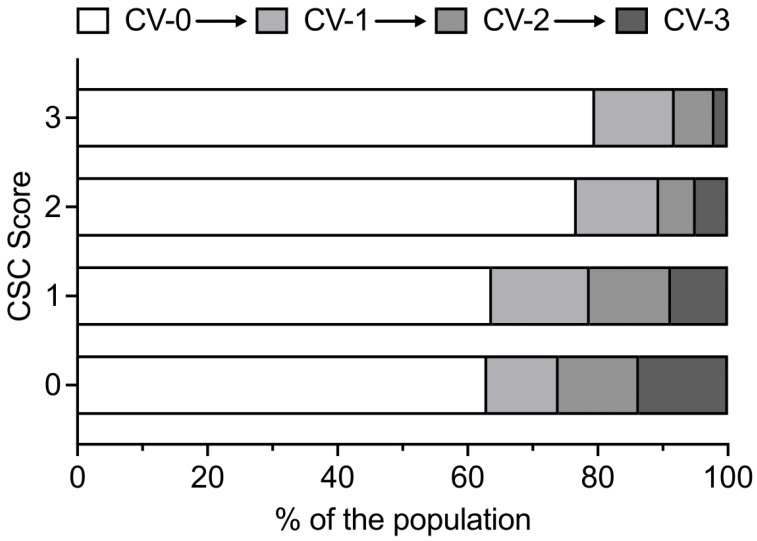 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Intracerebral and Subarachnoid Hemorrhage Research · Cerebrovascular and Carotid Artery Diseases
1. Introduction
In the treatment of aneurysmal subarachnoid hemorrhage (aSAH), cerebral vasospasm (CV) is a feared secondary complication [1]. Within the literature, the early detection and aggressive endovascular treatment of CV are known to reduce the risk of delayed cerebral ischemia (DCI) and to improve the functional neurological outcome [2]. Clinical and radiologic bleeding severity, smoking, female sex, and young age have been described as risk factors for CV [3,4]. Conversely, carotid calcification and intracranial calcification have been shown to be protective against angiographic and Doppler-sonographic CV [5,6,7]. However, carotid siphon calcification (CSC) was not only protective against angiographic CV but was also associated with an increased risk of DCI and an impaired functional neurological outcome [8].
CSC is linked with carotid stenosis and atherosclerosis [9]. Older age and a higher burden of atherosclerosis are associated with an increased arterial stiffness, which disrupts cerebral blood flow regulation [10,11]. Although CSC decreases the risk of CV after aSAH, at the same time it increases DCI risk due to disruption of the cerebral blood flow (CBF) [8]. Moreover, the influence of the CSC on clinical and radiographic severity and duration of CV has not been analyzed.
In this study, using a large consecutive aSAH cohort, we aimed to assess the impact of CSC on the severity of angiographic CV, the characteristics of CV detected through daily transcranial Doppler (TCD) ultrasonography, and the clinical manifestations of CV, specifically the occurrence of delayed ischemic neurological deficits (DINDs). Additionally, we evaluated the influence of CSC on long-term functional outcomes after aSAH.
2. Materials and Methods
From September 2008 to June 2016, 498 consecutive patients were included in our institutional aneurysm database at the university hospital of Essen. Patients with an aSAH and a CT scan available in our image viewing system were included in this retrospective study (n = 475). The local ethics committee approved this study, with the registration number 15-6331-BO. All patients or their legal representatives gave their written consent for the inclusion into the aneurysm database. The study is registered in the German Register for Clinical Trials (unique identifier: DRKS00008749; date of approval 30 June 2015, date of approval of supplementary requests 18 October 2016, 5 February 2019, 12 November 2019, 10 December 2019). The study data is available from the corresponding author upon reasonable request.
2.1. Treatment Process
All patients with suspected aSAH were subjected to a computed tomography (CT) scan upon arrival, unless a definitive diagnosis had already been established at another hospital. In such cases, the latter was the secondary referral center for the patients to our tertiary care center. Following the confirmation of the diagnosis, patients were subjected to digital subtraction angiography (DSA) in order to determine the source of bleeding. In instances where an aneurysm was identified as the bleeding source, the optimal course of action was discussed in a multidisciplinary fashion, including the possibility of performing either endovascular or microsurgical aneurysm occlusion. Patients were then transferred to our neurosurgical intensive care unit, where they remained for at least 14 days. Daily TCD studies were performed, and the patients were closely neurologically monitored to detect sings of possible CV. Oral or intravenous nimodipine was administered prophylactically to all aSAH patients during 3 weeks after aSAH. Acute hydrocephalus was managed with an external ventricular drain allowing continuous intracranial pressure (ICP) monitoring and drainage of cerebrospinal fluid if necessary. In case of elevated ICP >20 mmHg, medical management was performed to lower the ICP, followed by decompressive craniectomy in individuals with ICP crisis refractory to conservative management.
Events of new onset of focal or global neurological deficit, that could not be linked to other events, like, e.g., ICP increase, seizure, or rebleeding, were regarded as DINDs attributable to CV [12]. In these cases, the patients were taken for repeated DSA for further CV management. Moreover, DSA for CV verification was also initiated in unconscious aSAH patients with increasing cerebral blood flow velocity ([CBFV] mean value > 120 cm/s) in TCD. Confirmed angiographic CV was treated with intra-arterial nimodipine and, if insufficient, with angioplasty. After the acute monitoring period and hospitalization, all patients were transferred to appropriate neurological rehabilitation units. Patients were followed up clinically at our outpatient service, or, if not possible, by telephone at 6 months after aSAH.
2.2. Data Management and Statistics
The objective of this study was to analyze the impact of the CSC on the severity of the CV. To quantify the findings, the first author (AE) evaluated the non-contrast-enhanced CT scans and graded the most severe CSC for each patient according to the Woodcock score (grade 0: no calcification; grade 1: thin discontinuous calcification; grade 2: thin continuous calcification or thick discontinuous calcification; grade 3: thick continuous calcification) [13]; see Figure 1. To quantify the CV, the first author analyzed all available DSAs and graded the most severe CV on the DSAs according to the scale proposed by Merkel et al. (grade 0: all intracranial vessels show a physiological shape; grade 1: minimal narrowing affecting A2, A1 and/or M2; grade 2: moderate narrowing from M1 and terminal (intradural) segments of the internal carotid artery; grade 3: severe narrowing of the intradural internal carotid artery and the M1 with filiform (“ghost-like”) appearance of A1 and M1) [14]; see Figure 2. If no DSA was performed, the angiographic grade was defined as 0, and CV was considered absent.
The electronic health records of patients and the institutional aneurysm database were screened for the following data: clinical (using the World Federation of Neurosurgical Societies [WFNS] scale [15]) and radiographic (using the original Fisher scale [4]) bleeding severity, presence of acute hydrocephalus, type of aneurysm treatment (endovascular or microsurgical), daily TCD measurements, occurrence of ICP increase >20 mmHg, and/or DIND. Additionally, the following acknowledged or widely disputed risk factors for CV were also recorded for further analysis as confounders: age, sex, and smoking status. In all patients, the clinical outcome was documented 6 months after the discharge from hospital using the modified ranking scale (mRS) [16].
A descriptive statistic was performed, using mean values (± standard deviation [SD]), median values (interquartile range [IQR]), or absolute numbers (relative amount [%]), wherever applicable. A binary logistic regression was used to predict the occurrence of angiographic and TCD CV and DIND, adjusting for the risk factors such as age, sex, smoking status, radiographic (fisher score ≥ 3) and clinical (WNFS score ≥ 4) bleeding severity, treatment modality, and ICP crisis. Results were presented using adjusted odds ratios (aOR) and the 95% confidence interval (CI), as well as p-value (≤0.05). Additionally, a multinominal linear regression was performed to analyze the impact of CSC on the severity of angiographic CV, the number of days with increased CBFV, and the maximal CBFV values in TCD, using the same confounders, as mentioned above. Results are preesnted using regression coefficient (RC) and 95% CI, as well as p-value (≤0.05). Missing values were handled by multiple imputations for the following variables: patient age, patient sex, smoking status, Fisher grade, WFNS grade, aneurysm occlusion, angiographic CV, increased TCD, DIND, severity of angiographic CV (according to the Merkel scale), days of increased TCD values (>120 cm/s), and mRS 6 months after discharge. Additionally, a multinominal linear regression was performed to predict the outcome 6 months after discharge (using the mRS) based on the maximum CSC per patient, using the same confounders as mentioned above and also including the severity of the angiographic CV as a confounder. In all performed analyses, CSC was used as a continuous variable.
Statistical analysis was performed using IBM SPSS Statistics Version 29.0.0.0, and GraphPad PRISM Version 9.0 was used for visualization. All correlations with p ≤ 0.05 were considered significant. www.BioRender.com was used for visualization of the Woodcock scale and the Merkel scale. The manuscript was checked and improved by using www.DeepL.com. The article follows the STROBE reporting guidelines.
3. Results
The mean age of the final study population (n = 475) was 55.83 years (±SD 14.04), 320 patients were female (67.4%), and 267 patients were microsurgically clipped (58.4%). The missing values are displayed in absolute numbers. For detailed information on the study population, see Table 1.
There was no CSC in 40% of the cohort, and 41.6% had a CSC grade 2 or higher; see Figure 1. The distribution of angiographic severity of CV is shown in Figure 2. Approximately two-thirds of the aSAH population did not experience any CV. In total, 20% of the patients had a CV grade 2 or higher.
Within the binary logistic regression, the CSC showed independent association with the occurrence of DIND (aOR 0.76; 95% CI 0.59–0.98; p = 0.034) and angiographic CV (aOR 0.76; 95% CI 0.60–0.97; p = 0.025); see Table 2. Additionally, CSC was predictive of the severity of the angiographic CV (RC −0.14; 95% CI −0.24 to −0.04; p = 0.006) in the linear regression; see Table 3. The distribution of angiographic CV severity in the cohort depending on the CSC gradings is shown in Figure 3. A decline in the relative proportions of higher-grade CVs has been observed, concomitant with an increase in CSC.
With regard to the manifestation of CV in TCD observations, multivariable analysis did not demonstrate a significant correlation between CSC severity and the occurrence of CV (aOR 0.87; 95% CI 0.68–1.11; p = 0.265; see Table 2), nor with the absolute maximum CBFV value (RC +1.57; 95% CI −7.45 to +10.58; p = 0.731; see Table 3). Nevertheless, a substantial inverse relationship was observed between CSC severity and the number of days on which CVs (>120 cm/s) were recorded by TCD. (RC −0.43; 95% CI −0.77 to −0.10; p = 0.010; see Table 3).
Conversely, a higher maximum severity of CSC has been shown to correlate with poorer functional outcomes at six months following aSAH (RC +0.12; 95% CI +0.05 to +0.18; p < 0.001); see Table 4.
4. Discussion
Our data shows that atherosclerosis of the large intracranial vessels, as represented by CSC, not only has a protective effect against the occurrence of CV, but also mitigates the severity of angiographic CV.
Specifically, we observed that higher levels of CSC were associated with lower rates of angiographic CV. Furthermore, our findings reveal an inverse correlation between increasing CSC levels and the severity of angiographic CV, suggesting a potential protective mechanism. A previous study performed by our group [8] showed an inverse correlation between the occurrence of an angiographic CV in the specific vascular territories of ICA, ACA, and MCA and the CSC, also measured using the Woodcock scale [13]. This protective effect of CSC against CV could be caused by the increasing arterial stiffness in patients with a higher level of atherosclerosis [10,11]. Our data suggests that any level of atherosclerosis in the cerebral vessels reduces the severity of angiographic CV. These findings contradict the results of previous studies, which reported a protective effect against CV detected by TCD only at higher levels of atherosclerosis [6]. Interestingly, the CSC was found to be independently linked to a decreased severity of angiographic CV, even though the analyses included age as a confounder. It is generally accepted that younger age is one of the major risk factors for suffering from CV [3], while older age is known to be a risk factor for the progression of atherosclerosis [17]. This observation, when supported by these findings, suggests that younger age itself may not be a significant risk factor and may merely coincide with more severe CV, most likely due to a general lower prevalence of atherosclerosis, such as CSC, in this age group. At the same time, our analysis confirms age as a significant risk factor for both the occurrence and severity of CV, indicating that its influence may extend beyond the effects of atherosclerosis alone.
Although our data showed a predictive value of the CSC for angiographic CV, we could not predict CV detected by TCD using a cut-off value of >120 cm/s. Another study showed an inverse correlation between the CSC and the occurrence of TCD-detected CV, but also an inverse correlation between CSC and the severity of TCD-detected CV [7]. Our data did not show these inverse correlations. It is possible that vessel reactivity is decreased by intracranial atherosclerosis. This hypothesis is supported by the evidence that such atherosclerosis has been demonstrated to reduce cerebral autoregulatory responses to neuronal activity and the CBF [11]. Therefore, it may be that lower levels of CV are not as readily detected by TCD, which naturally covers only the larger intracranial vessels, in patients with higher levels of CSC. A different cut-off threshold might be chosen in future studies to further investigate this hypothesis. However, due to a loss of data, we were not able to analyze the TCD-measured CV utilizing different cut-offs.
In addition, we were able to show a lower probability of DIND in aSAH individuals with higher level of CSC. A correlation between the occurrence of DIND and CV has been reported in the literature [12,18], supporting our findings of a lower incidence of DIND in patients with CSC. However, it has also been critically discussed that angiographic CV is not exclusively the cause of DIND and that it could also be caused by local changes in cerebral perfusion [19]. This association is not explained by our data but could be related to local small CV not detected by either TCD or DSA, and it opens new questions for future research projects.
However, our data also showed a link between higher levels of CSC and unfavorable outcomes, independent of the severity of the angiographic CV. This clearly shows that the protective effect against CV, be it angiographic or Doppler sonographic, and the protective effect against DIND are not the only factors influenced by the higher burden of atherosclerosis shown by CSC. CSC has been shown to be predictive of the occurrence of early cerebral ischemia, but not of delayed cerebral ischemia [8]. The missing link to the DCI is still unexplained and can only be postulated due to a multifactorial process leading to these DCIs and therefore potentially leading to an unfavorable outcome. Potential effects leading to worse neurological outcomes could be due to the generally increased incidence of ischemic events in populations with a higher burden of atherosclerosis [20,21]. The higher burden of cerebral small vessel disease [22] and the higher burden of downstream micro emboli in patients with higher levels of atherosclerosis [23] may also contribute. Furthermore, the lack of appropriate CBF responses to neural activities [11] could be a contributing factor to fill be the missing link between the decreased severity of CV at higher levels of CSC.
The limitations of this study are its purely retrospective nature and therefore its selection bias. Nonetheless, the implementation of linear and binary logistic regression, in conjunction with the correction of analyses for the aforementioned confounders, has been demonstrated to partially surmount these limitations. Furthermore, the results of the lack of correlation with CBFV should be interpreted with caution due to the high number of missing patients in this analysis. Additionally, the calcifications and plaques in the carotid artery were not differentiated, and potentially vulnerable non-calcified plaques were not analyzed separately.
5. Conclusions
In summary, our data strongly suggests that CSC not only protects against the occurrence of angiographic CV, but also reduces the severity of angiographic CV, reduces the duration of CV detected by TCD, and reduces the incidence of DIND in aSAH patients. Our findings indicate that the atherosclerotic status of patients, as measured by CSC, should be incorporated into patient therapy. This would enable the identification of patients at risk of CV with lower CSC levels, as well as patients with lower CV risk who are still at higher risk of adverse outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Romenskaya T. Longhitano Y. Piccolella F. Berger J.M. Artico M. Taurone S. Maconi A. Saviano A. Caramuta M. Savioli G. Cerebral Vasospasm: Practical Review of Diagnosis and Management Rev. Recent. Clin. Trials 202318121810.2174/157488711766622081012104835950252 · doi ↗ · pubmed ↗
- 2Jabbarli R. Pierscianek D. Rölz R. Oppong M.D. Kaier K. Shah M. Taschner C. Mönninghoff C. Urbach H. Beck J. Endovascular treatment of cerebral vasospasm after subarachnoid hemorrhage: More is more Neurology 201993 e 458e 46610.1212/WNL.000000000000786231278116 · doi ↗ · pubmed ↗
- 3Rumalla K. Lin M. Ding L. Gaddis M. Giannotta S.L. Attenello F.J. Mack W.J. Risk Factors for Cerebral Vasospasm in Aneurysmal Subarachnoid Hemorrhage: A Population-Based Study of 8346 Patients World Neurosurg.2021145 e 233e 24110.1016/j.wneu.2020.10.00833049382 · doi ↗ · pubmed ↗
- 4Fisher C.M. Kistler J.P. Davis J.M. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning Neurosurgery 198061910.1227/00006123-198001000-000017354892 · doi ↗ · pubmed ↗
- 5Colip C.G. Wo S. Hippe D.S. Watase H. Urdaneta-Moncada A.R. Zhu C. Wu L. Vranic J.E. Kelly C.M. Levitt M.R. Computed tomography angiography findings predictive of post-intervention vasospasm in patients with aneurysmal subarachnoid hemorrhage Br. J. Radiol.2021942020089310.1259/bjr.2020089333661704 PMC 8506174 · doi ↗ · pubmed ↗
- 6Hussein H.M. Zacharatos H. Cordina S. Lakshminarayan K. Ezzeddine M.A. Intracranial vascular calcification is protective from vasospasm after aneurysmal subarachnoid hemorrhage J. Stroke Cerebrovasc. Dis.2014232687269310.1016/j.jstrokecerebrovasdis.2014.06.01325307431 · doi ↗ · pubmed ↗
- 7Jayaweera M. Hernandez A. Haripottawekul A. Stretz C. Furie K.L. Yaghi S. Mahta A. Impact of intracranial atherosclerosis burden on vasospasm risk and outcomes in aneurysmal subarachnoid hemorrhage J. Stroke Cerebrovasc. Dis.20243310807710.1016/j.jstrokecerebrovasdis.2024.10807739396660 · doi ↗ · pubmed ↗
- 8Engel A. Song L. Rauschenbach L. Gümüs M. Santos A.N. Dinger T.F. Oppong M.D. Li Y. Gembruch O. Ahmadipour Y. Impact of Carotid Siphon Calcification on the Course and Outcome of Patients with Aneurysmal Subarachnoid Hemorrhage Stroke 2024552305231410.1161/STROKEAHA.124.04759439101226 · doi ↗ · pubmed ↗