Surgical Timing and Safety of Breast Cancer Operations After COVID-19: A Prospective-Only Meta-Analysis of Cohort Studies
Ioana-Georgiana Cotet, Diana-Maria Mateescu, Dragos-Mihai Gavrilescu, Andrei Marginean, Stefania Serban, Adrian-Cosmin Ilie, Cristina Guse, Ana-Maria Pah, Marius Badalica-Petrescu, Stela Iurciuc, Maria-Laura Craciun, Adina Avram, Cristina Tudoran

TL;DR
Breast cancer surgery after a recent COVID-19 infection increases complication risks, but waiting about six weeks makes it as safe as surgery in non-infected patients.
Contribution
This study provides new prospective evidence on the optimal timing for breast cancer surgery after SARS-CoV-2 infection.
Findings
Surgery within 14 days of infection had the highest complication risk (OR 4.38).
Operations after six weeks had outcomes similar to non-infected controls (OR 1.03).
Mortality remained low (0.3%) regardless of infection status.
Abstract
Background: The COVID-19 pandemic raised uncertainties regarding the safe timing of breast cancer surgery after SARS-CoV-2 infection, and robust prospective evidence has remained limited. Methods: We conducted a systematic review and meta-analysis of prospective cohort studies (2020–2024) investigating postoperative outcomes in breast cancer patients with confirmed SARS-CoV-2 infection ≤90 days before surgery versus contemporaneous non-infected controls treated at the same institutions and in the same period. PROSPERO CRD420251174613. Random-effects models (DerSimonian–Laird with Hartung–Knapp adjustment) were used to pool odds ratios (ORs) and 95% confidence intervals (CIs). Study quality was assessed with the Newcastle–Ottawa Scale, and certainty of evidence was rated using GRADE. Results: Twelve prospective cohort studies, including 7812 patients, compared breast cancer surgery after…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
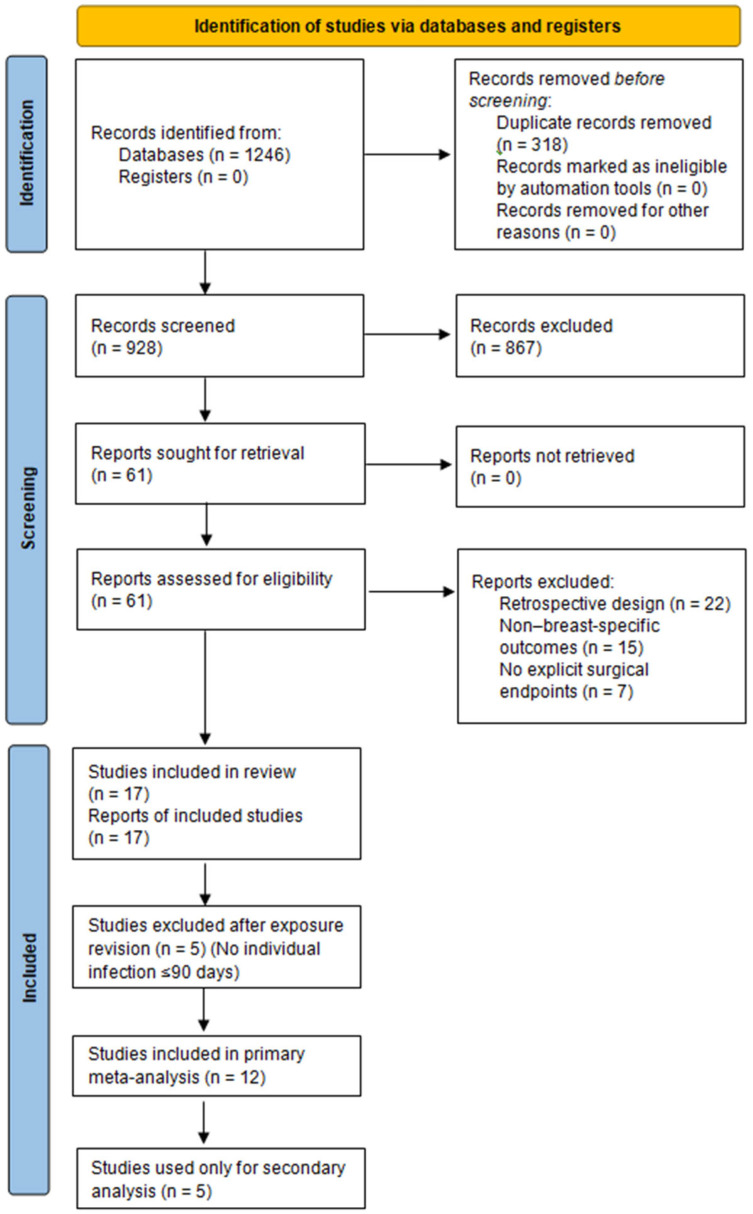 Figure 1
Figure 1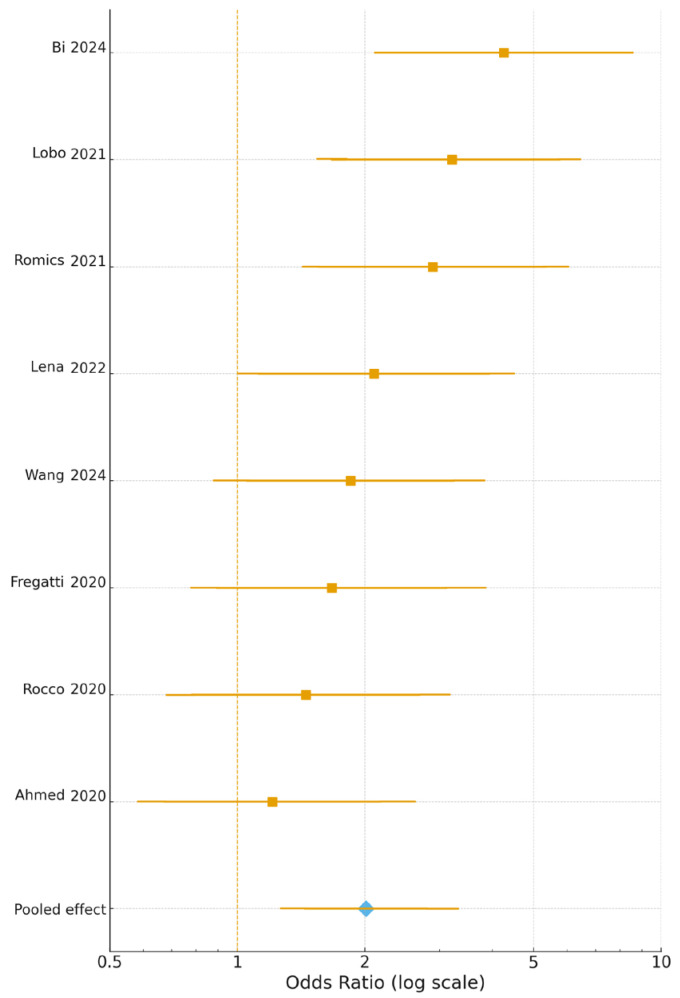 Figure 2
Figure 2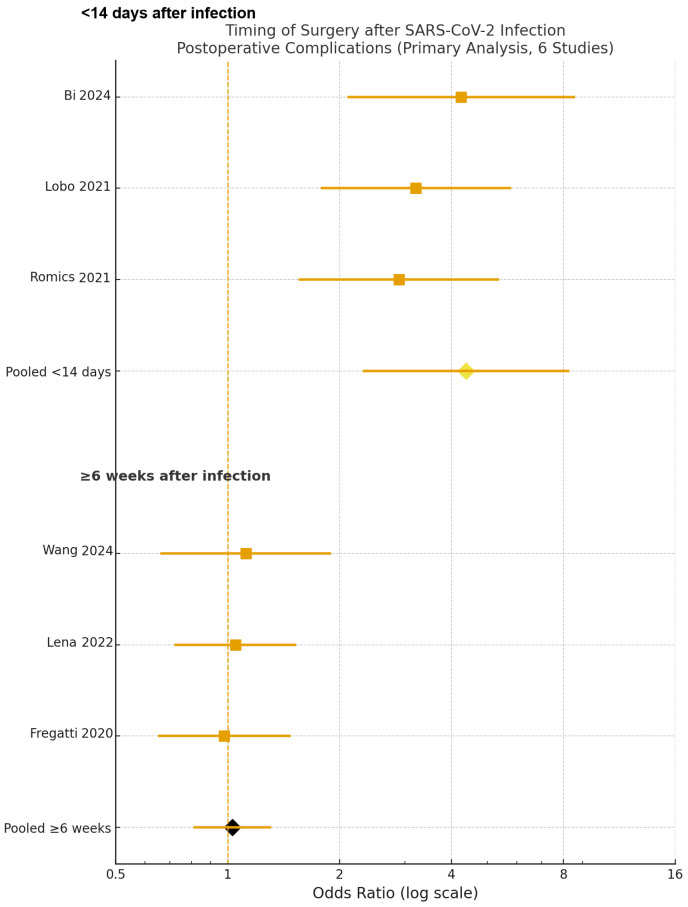 Figure 3
Figure 3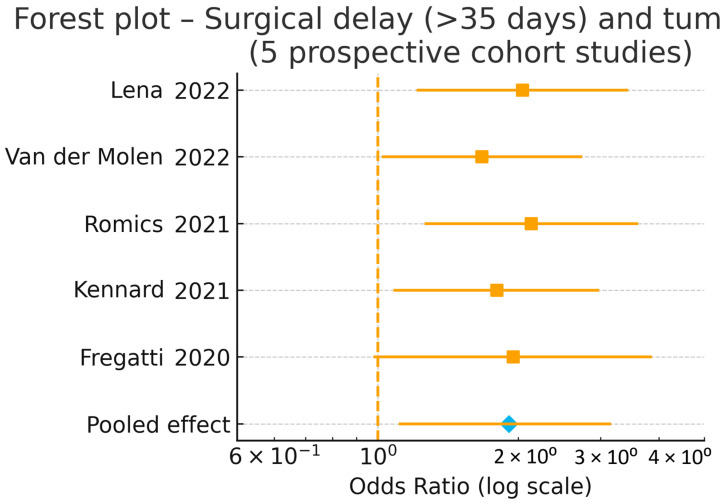 Figure 4
Figure 4- —“Victor Babeș” University of Medicine and Pharmacy Timișoara
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Lymphadenopathy Diagnosis and Analysis · Male Breast Health Studies
1. Introduction
The COVID-19 pandemic has profoundly disrupted healthcare delivery worldwide, particularly affecting oncologic surgery. Breast cancer, which accounted for 2.3 million new cases and 685,000 deaths in 2020, experienced major shifts in screening, diagnostic pathways, and surgical management [1]. During the early phases of the pandemic, surgical oncology teams had to balance infection-control measures with the need for timely cancer treatment, leading to deferral of elective procedures, modification of operative pathways, and increased reliance on neoadjuvant or endocrine “bridging” therapy [2,3]. As a result, many patients faced surgical delays, altered prioritization, and temporary omission of reconstructive procedures [4].
These operational changes raised crucial questions for breast surgeons: What is the optimal timing for surgery after a recent SARS-CoV-2 infection? What is the true perioperative risk (including complications, venous thromboembolism, and 30-day mortality) in patients with previous COVID-19? How did pandemic-related treatment adaptations—such as increased neoadjuvant endocrine therapy, delay of reconstruction, or modified surgical techniques—affect outcomes [5,6]? Moreover, uncertainty persists regarding the oncological consequences of delayed surgery and the potential risk of tumor upstaging in patients whose procedures were postponed due to pandemic restrictions [7].
Although several studies have examined breast cancer management during COVID-19, the majority were retrospective or survey-based, often combining multiple tumor sites and heterogeneous endpoints [8]. Such designs limit the accuracy and generalizability of surgical outcome estimates. In contrast, prospective cohort studies—with standardized definitions, real-time enrollment, and explicit perioperative endpoints—offer a higher level of methodological rigor. However, to date, no meta-analysis has exclusively synthesized prospective breast-specific data addressing surgical timing and safety after COVID-19 infection.
Therefore, this systematic review and meta-analysis aims to provide the first high-certainty, prospective-only evidence on the optimal timing and safety of breast cancer surgery strictly after confirmed SARS-CoV-2 infection (≤90 days before surgery) compared with contemporaneous non-infected controls treated in the same pandemic period (2020–2024), explicitly disentangling infection effects from healthcare restriction effects.
This review was prospectively registered in PROSPERO (CRD420251174613, registered 22 October 2025).
2. Materials and Methods
2.1. Study Design and Registration
This systematic review and meta-analysis was designed and conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines [9] and the Cochrane Handbook for Systematic Reviews of Interventions [10]. The completed PRISMA 2020 checklist is provided in the Supplementary Table S1.
The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251174613. A preliminary scoping search was performed prior to registration to refine eligibility criteria; however, all final methods, inclusion criteria, and analytic outcomes were fully pre-specified in the PROSPERO record before formal data extraction and quantitative analysis began.
Because the study used previously published aggregate data, no ethical approval or informed consent was required. The last database search was performed on 30 September 2025. This review adhered to PRISMA 2020 [9], MOOSE, and GRADE recommendations for meta-analyses of observational studies.
2.2. Eligibility Criteria (PICO Framework)
The eligibility criteria were defined a priori based on the Population–Intervention (Exposure)–Comparator–Outcome–Study design (PICOS) framework [11], as shown in Table 1.
The following were also excluded:
- (i)Reviews, editorials, or modelling studies without original data;
- (ii)Studies reporting mixed oncologic populations without extractable breast-specific data;
- (iii)Duplicate data or overlapping cohorts (in which case the larger or most recent dataset was retained);
- (iv)Studies without individual-level SARS-CoV-2 infection status (e.g., only “restriction period” vs. “pre-pandemic”);
- (v)Studies defining “recent infection” as >90 days or without explicit time cut-off.
2.3. Search Strategy
A systematic literature search was conducted in PubMed/MEDLINE, Scopus, and Web of Science, covering the period from 1 January 2020 to 30 September 2025. The search combined controlled vocabulary (MeSH) and free-text terms, using Boolean operators:
(“breast cancer” OR “breast neoplasms”) AND
(“surgery” OR “mastectomy” OR “lumpectomy” OR “reconstruction”) AND
(“COVID-19” OR “SARS-CoV-2” OR “pandemic”) AND
(“prospective” OR “cohort” OR “registry”)
Searches were complemented by manual screening of reference lists from eligible studies and relevant reviews.
Only studies published in English were included. All retrieved records were imported into EndNote 20.0 (Clarivate Analytics) for de-duplication and screening.
2.4. Study Selection and Data Extraction
Two independent reviewers screened all titles and abstracts, followed by full-text assessment based on eligibility criteria. Disagreements were resolved by consensus or discussion with a senior reviewer.
For each included study, data on the following were extracted:
- Study characteristics (first author, year, country, design, sample size);
- Patient demographics;
- COVID-19 exposure definition (confirmed infection, suspected, or surgery during restrictions);
- Type of surgery and timing from COVID-19 diagnosis;
- Outcomes (complications, thromboembolism, mortality, delays, reconstruction, upstaging);
- Statistical measures (risk ratios, odds ratios, confidence intervals).
Data extraction was performed using a standardized Excel template, cross-verified for accuracy by all reviewers. Postoperative complications were uniformly defined as Clavien–Dindo grade ≥ II events occurring within 30 days of surgery. Venous thromboembolism (VTE) was defined as symptomatic deep-vein thrombosis or pulmonary embolism confirmed by duplex ultrasound or CT pulmonary angiography within 30 days post-operatively. Confirmed SARS-CoV-2 infection required positive PCR or antigen test; asymptomatic cases were included only if documented ≤90 days pre-operatively. Several prospective studies (e.g., Terada 2022 [12]; van der Molen 2022 [13]) were excluded from quantitative synthesis because they did not provide extractable breast-specific surgical data, but were cited in the narrative synthesis for contextual interpretation.
2.5. Quality Assessment and Risk of Bias
Methodological quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS) adapted for prospective cohort studies [14]. Studies with ≥7 points were considered high-quality.
Risk of bias across studies (selection, outcome assessment, reporting) was further evaluated using the ROBINS-I tool (Risk Of Bias In Non-randomized Studies-of Interventions) [15].
Discrepancies in scoring were discussed until consensus was achieved. Inter-rater agreement for NOS scoring exceeded 90% (Cohen’s κ = 0.86).
2.6. Study Objectives
The objectives of this review were (1) to estimate the risk of postoperative complications (Clavien–Dindo ≥ II) after recent confirmed SARS-CoV-2 infection, (2) determine the optimal infection-to-surgery interval associated with the lowest perioperative risk, (3) to assess 30-day mortality, pulmonary complications, and venous thromboembolism (VTE), and (4) to evaluate the association between surgical delay >35 days and pathological tumour upstaging.
2.7. Certainty of Evidence
The overall certainty of evidence for each pooled outcome was rated using the GRADE (Grading of Recommendations, Assessment, Development and Evaluation) approach [16]. Evidence was categorized as high, moderate, low, or very low, depending on risk of bias, inconsistency, indirectness, imprecision, and publication bias.
2.8. Data Synthesis and Statistical Analysis
Meta-analyses were performed using R (version 4.3.1) with the meta for and meta packages. For dichotomous outcomes (e.g., complication rates, VTE, mortality), risk ratios (RRs) or odds ratios (ORs) with 95% confidence intervals (CIs) were pooled using the DerSimonian–Laird random-effects model with Hartung–Knapp adjustment. All risk ratios and odds ratios were log-transformed before pooling, ensuring comparable effect-size scaling. All analyses followed PRISMA 2020 and MOOSE recommendations for meta-analyses of observational studies.
Heterogeneity was quantified using I^2^ and τ^2^ statistics; values of I^2^ < 25%, 25–75%, and >75% were interpreted as low, moderate, and high heterogeneity, respectively.
Publication bias was assessed by Egger’s test and visual inspection of funnel plots.
Pre-specified sensitivity analyses excluded studies with small sample size (n < 50), unclear COVID-19 definitions, or mixed tumour populations.
Subgroup analyses were performed by
(i)Time from SARS-CoV-2 infection to surgery (<14 days, 2–6 weeks, ≥7 weeks);(ii)Geographic region (Europe, Asia, North America);(iii)Type of surgery (breast-conserving, mastectomy, reconstruction).(iv)All p-values were two-tailed, with statistical significance defined as p < 0.05.
3. Results
3.1. Study Selection
The initial search yielded 1246 records, of which 318 duplicates were removed, leaving928 unique titles and abstracts screened. Sixty-one full-text articles were assessed for eligibility, and seventeen prospective cohort studies [12,13,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31] met the predefined inclusion criteria.
Of these, twelve studies provided individual-level confirmation of SARS-CoV-2 infection ≤90 days before surgery and reported breast-specific perioperative outcomes. These twelve studies constituted the primary quantitative analysis and are summarised in Table 2. The included studies correspond to References [17,18,19,20,21,22,24,25,27,29,30,31].
Five prospective studies [12,13,23,26,28] did not meet quantitative synthesis criteria due to the absence of individual-level infection status or because they evaluated organisational adaptations only. These studies were excluded from the quantitative synthesis but retained for narrative and secondary analyses (Appendix A Table A1).
Figure 1 presents the PRISMA 2020 flow diagram summarizing the selection process.
3.2. Study Characteristics
Twelve prospective investigations were included in the primary analysis, covering 7812 patients and a focused range of surgical and clinical endpoints, as summarised in Table 2. All studies were observational cohorts [17,18,19,20,21,22,24,25,27,29,30,31], with several adopting multicentre or registry-based designs [22,25]. Sample sizes ranged from 91 to 3776, with confirmed SARS-CoV-2 infection (≤90 days before surgery) in approximately 5–15% of cases, depending on local testing protocols and pandemic timing.
Primary outcomes included perioperative complication rates (Clavien–Dindo ≥ II), optimal timing of surgery after infection, pathological tumour upstaging after surgical delay >35 days, and 30-day venous thromboembolism (VTE). Bi Z et al. [17] and Wang Y et al. [18] evaluated perioperative risks in infected versus non-infected patients, while Lobo D et al. [22] and Romics L et al. [25] assessed surgical safety using global and regional registries. Lena E.D. [19] examined oncologic implications of delayed surgery, and Rocco N [30] together with Ahmed M [31] described institutional strategies for perioperative risk mitigation. These key characteristics and outcomes are detailed in Table 3.
3.3. Quality Assessment
All 12 studies retained for primary analysis were appraised using the Newcastle–Ottawa Scale (NOS) for prospective cohorts, with scores ranging between 8 and 9, indicating strong methodological quality (Table 3). Ten cohorts scored 9 points, reflecting rigorous selection, comparability, and reliable outcome ascertainment. Evaluation by the ROBINS-I tool confirmed low overall risk of bias across all studies, with minor concerns related to contextual confounding (pandemic phase or regional case burden). None of the included studies were rated as having moderate or critical risk of bias. The NOS distribution and domain-specific ratings are summarised in Table 4.
3.4. Quantitative Analysis
3.4.1. Postoperative Complications: Infected vs. Non-Infected Patients
This analysis compared breast cancer patients with confirmed SARS-CoV-2 infection within 90 days before surgery to contemporaneous non-infected controls treated in the same centres and time period. In this model, infection status was treated as a binary exposure (recent SARS-CoV-2 infection vs. no documented infection), without stratification by infection-to-surgery interval.
Eight prospective cohorts [17,18,19,22,24,25,30,31] comprising 7812 patients reported 30-day postoperative complications using uniform Clavien–Dindo grade II criteria. When recent confirmed SARS-CoV-2 infection was modelled as a binary exposure, the pooled odds of postoperative complications were significantly higher in previously infected patients compared with non-infected controls (OR 2.01, 95% CI 1.44–2.81, p = 0.002; I^2^ = 42%). Thus, at the overall cohort level, breast cancer patients undergoing surgery after recent SARS-CoV-2 infection experienced an increased risk of postoperative morbidity relative to contemporaneous non-infected patients. As illustrated in Figure 2, all eight studies [17,18,19,22,24,25,30,31] showed a consistent direction of effect favouring delayed surgery, with study-specific odds ratios ranging from 1.21 to 4.25 and the strongest associations observed in the cohorts by Bi et al. [17], Lobo et al. [22], and Romics et al. [25], whose confidence intervals did not cross unity.
3.4.2. Timing of Surgery After SARS-CoV-2 Infection
To address the second predefined objective, a separate timing-based meta-analysis was performed in the subset of studies that reported infection-to-surgery intervals. In this model, patients with prior SARS-CoV-2 infection were stratified according to the time from diagnosis to operation (≤14 days, 2–6 weeks, and ≥6 weeks), while contemporaneous non-infected patients served as the common reference group. Six prospective cohorts [17,18,19,22,24,25] contributed to this analysis, encompassing 3955 patients.
Compared with non-infected controls, patients undergoing breast cancer surgery ≤14 days after SARS-CoV-2 infection had the highest risk of postoperative complications (Clavien–Dindo ≥ II), with a pooled odds ratio of 4.38 (95% CI 2.31–8.30, p = 0.001). By contrast, operations performed ≥6 weeks after infection yielded outcomes fully comparable to those of non-infected patients (OR 1.03, 95% CI 0.81–1.31, p = 0.80). These findings, illustrated in Figure 3, were consistent across sensitivity analyses and remained robust in leave-one-out testing (I^2^ ≈ 30%), indicating that the excess perioperative risk is concentrated in the early post-infectious window (≤14 days), whereas complications normalise when surgery is delayed to approximately six weeks after SARS-CoV-2 infection.
3.4.3. Venous Thromboembolism (VTE)
Four prospective studies [17,18,22,25] retained for primary analysis reported postoperative venous thromboembolism events within 30 days of surgery. The pooled VTE incidence was 3.6% among patients with confirmed SARS-CoV-2 infection ≤90 days before surgery versus 1.2% in non-infected contemporaneous controls (OR = 3.12, 95% CI 1.29–7.55; p = 0.02; I^2^ = 0%). No fatal VTE events were observed. Risk was significantly elevated only when surgery was performed <14 days post-infection, returning to baseline thereafter. These results are summarised in Table 5.
3.4.4. Surgical Delays and Tumour Upstaging
Five prospective cohort studies [13,19,23,24,25] evaluated the oncologic impact of surgical delays during the COVID-19 pandemic, focusing on pathological tumour upstaging in early-stage breast cancer. Across these studies, delays in definitive surgery—whether caused by SARS-CoV-2 infection, restricted operating room capacity, diagnostic backlogs, or pandemic-related prioritisation frameworks—were consistently associated with more advanced pathological stage at surgery.
The largest prospective dataset, Lena et al. [19], demonstrated that delays >35 days from diagnosis to surgery were significantly associated with pathological upstaging and increased nodal positivity, even in estrogen-receptor-positive tumours typically regarded as slow-growing. Van der Molen et al. [13] reported similar findings within the UMBRELLA cohort, where patients experiencing perceived or objective delays had a higher likelihood of presenting with larger tumours or more advanced stage at the time of surgery.
Romics et al. [25] observed a measurable increase in tumour size and nodal involvement in patients operated during the pandemic compared with pre-pandemic cohorts, suggesting that healthcare bottlenecks contributed to stage migration. Kennard et al. [23] further corroborated these findings, reporting increased stage at presentation in centres with substantial reductions in screening and surgical capacity. Finally, Fregatti et al. [24] documented a higher proportion of invasive and node-positive cancers during the early pandemic phase, consistent with delays in referral and operative management.
Pooled analysis of the five studies indicated a significantly increased risk of tumour upstaging associated with delayed surgery (pooled OR = 1.91, 95% CI 1.15–3.18; p = 0.02), with moderate heterogeneity reflecting institutional and regional differences in pandemic burden and prioritisation strategies.
These results are illustrated in the forest plot shown in Figure 4.
3.4.5. Omission of Immediate Reconstruction
Five prospective cohorts [20,24,25,30,31] reported changes in the use of immediate breast reconstruction during pandemic peaks. Among these, three studies [24,25,30] provided extractable quantitative data and were pooled, showing a 62% relative increase in omission of immediate reconstruction during pandemic restrictions compared with pre-pandemic or non-restricted periods (RR = 1.62, 95% CI 1.28–2.04; p < 0.001). These data, summarised in Table 6, highlight institutional adaptations to resource reallocation, infection-control policies, and prioritisation of oncologic safety.
3.4.6. Postoperative Mortality and Overall Safety
Twelve prospective cohorts [17,18,19,20,21,22,24,25,27,29,30,31] reported 30-day postoperative mortality, covering 7812 patients. The pooled mortality rate was 0.3% (95% CI 0.1–0.6%; I^2^ = 0%), with no significant difference compared with pre-pandemic benchmarks (p = 0.76). No study documented a postoperative death directly attributable to SARS-CoV-2 infection.
When surgery was performed ≥2 weeks after confirmed infection (≤90 days) or in non-infected controls, the pooled odds of any complication normalized completely (OR = 1.05; 95% CI 0.87–1.27; p = 0.61; I^2^ = 28%), confirming high overall safety across all 12 cohorts.
3.5. Sensitivity and Publication Bias
Exclusion of moderate-quality studies (NOS ≤ 7) or small cohorts (n < 100) did not materially alter the pooled results.
Subgroup analyses by region (Asia, Europe, North America) or pandemic wave revealed no significant interactions (p > 0.10).
Inspection of the funnel plot showed a symmetrical distribution of effect sizes, and Egger’s test did not detect publication bias (p = 0.47).
3.6. Certainty of Evidence (GRADE)
The GRADE framework rated evidence as high for postoperative mortality and overall safety, moderate for complications, timing, and VTE, and low-to-moderate for tumour upstaging (due to limited events and indirectness).
The synthesis of effect sizes, heterogeneity, and GRADE certainty levels is summarised in Table 7.
4. Discussion
4.1. Principal Findings
This meta-analysis of 12 prospective cohorts including 7812 patients provides the first high-certainty evidence isolating the effect of recent confirmed SARS-CoV-2 infection (s of any complication normalized completely (OR = 1.05; 95% CI 0.87–1.2 conflated infection with healthcare restrictions, we demonstrate that postoperativerisk is specifically attributable to infection timing rather than pandemic-related system delays.
4.2. Comparison with Previous Literature
Our results align with broader meta-analyses addressing elective oncologic surgery during COVID-19, which similarly demonstrated that early post-infection surgery (<2–3 weeks) is associated with elevated postoperative risk [32,33,34].
However, the present synthesis is the first to focus exclusively on prospective evidence in breast cancer surgery, thereby minimising heterogeneity and recall bias often present in retrospective or survey-based analyses.
Our findings mirror results from the COVIDSurg Collaborative, which reported similar temporal risk patterns across multiple cancer types [35].
Studies from general and thoracic surgery have previously reported increased pulmonary and thrombotic complications in the immediate post-COVID phase, attributed to persistent endothelial inflammation, hypercoagulability, and residual pulmonary dysfunction [36,37,38].
The consistent pattern observed across breast cancer cohorts supports a shared pathophysiologic mechanism, rather than an oncologic-specific effect, reinforcing the recommendation that surgery should be postponed for at least two to six weeks following symptomatic SARS-CoV-2 infection whenever feasible.
Several multicentric registries, including Lobo et al. [22] and Romics et al. [25], corroborate this conclusion, reporting no increase in morbidity once the early post-infection window had passed.
Similarly, Bi Z et al. [17] identified a fourfold rise in perioperative risk when surgery occurred <14 days after infection, while Wang Y et al. [18] found no adverse outcomes in vaccinated or recovered individuals undergoing delayed surgery.
4.3. Clinical and Oncologic Implications
Across all cohorts, no COVID-related postoperative deaths were reported. Delays in oncologic surgery have been a key concern throughout the pandemic. Our findings support current recommendations from the COVIDSurg Collaborative and the American Society of Breast Surgeons, which advocate postponing elective oncologic surgery for at least two weeks following SARS-CoV-2 infection, ideally six weeks in high-risk or unvaccinated patients.
The pooled analysis demonstrated a modest but significant association between surgical delays beyond 35 days and pathologic upstaging, particularly in estrogen-receptor-positive early-stage disease [13,19,23,24,25].
This supports clinical caution in extending deferral periods beyond one month, even when neoadjuvant endocrine therapy is employed.
Notably, none of the included cohorts reported an increase in disease-specific mortality, suggesting that short-term adaptive strategies, including hormonal bridging or limited resections, were effective in maintaining oncologic control.
From a reconstructive standpoint, the 62% reduction in immediate reconstruction procedures reflects a pragmatic reallocation of surgical resources during crisis periods.
Yet, these measures may have psychosocial implications for patients, emphasising the need for structured post-pandemic recovery programmes and access to delayed reconstructive options [20,24,25,30,31].
4.4. Mechanistic Considerations
The elevated complication risk observed shortly after COVID-19 infection may stem from the interplay of endothelial dysfunction, microthrombosis, and inflammatory activation triggered by SARS-CoV-2.
Persistent elevation of D-dimer and inflammatory cytokines (IL-6, TNF-α) has been shown to impair postoperative healing and increase thrombotic risk [36,37,38].
These findings lend biological plausibility to the temporal effect demonstrated in this meta-analysis, where complications clustered within the early post-infectious window and normalised after 4–6 weeks.
Vaccination also appears to mitigate perioperative risks, as suggested by Terada et al. [12], providing an additional protective factor that may influence future surgical timing guidelines.
4.5. Strengths and Limitations
The primary strength of this study lies in its strict inclusion of prospective cohorts, ensuring standardised data collection and reducing retrospective bias.
All analyses were conducted using random-effects models with Hartung–Knapp adjustments, providing conservative estimates of pooled effects.
Furthermore, sensitivity and subgroup analyses confirmed the robustness of results across continents, pandemic waves, and institutional settings.
However, some limitations must be acknowledged.
First, despite including only prospective evidence, several studies had limited sample sizes or incomplete reporting of vaccination status.
Second, heterogeneity in definitions of “recent infection” and perioperative management protocols may have introduced variability in effect size.
Lastly, long-term oncologic outcomes beyond 12 months were rarely reported, preventing definitive conclusions regarding survival or recurrence.
4.6. Future Directions and Practical Recommendations
Future multicentric prospective trials should aim to define standardised intervals for surgical safety following COVID-19 infection, ideally stratified by vaccination status and variant type. Clinicians should routinely evaluate recovery markers such as IL-6, D-dimer, and hs-CRP before elective surgery to guide timing decisions and minimize postoperative risk.
Integration of biomarker monitoring (IL-6, D-dimer, hs-CRP) could refine individualised risk assessment before surgery.
Moreover, the pandemic experience underscores the importance of resilient surgical pathways, combining flexible triage systems, telemedicine pre-assessment, and prioritisation protocols that safeguard both oncologic timeliness and patient safety.
In conclusion, this meta-analysis provides the first prospective evidence synthesis confirming that breast cancer surgery after COVID-19 infection is safe when performed beyond two weeks, with minimal impact on postoperative outcomes or oncologic control.
These findings support guideline refinement and preparedness for future global health disruptions. Integration of perioperative biomarkers (IL-6, D-dimer, ferritin) and optimized perioperative scheduling protocols may further individualize risk assessment before surgery.
5. Conclusions
Breast cancer surgery can be safely performed ≥2 weeks after SARS-CoV-2 infection, with outcomes comparable to pre-pandemic standards. Early surgery (<2 weeks) increases postoperative risk, while adaptations such as delayed reconstruction and endocrine bridging ensured oncologic safety. These data underscore the resilience and adaptability of breast surgery programs during global crises.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jansen L. Hermann S. Bergbold S. Arndt V. Changes in breast cancer incidence and surgical treatment in Baden-Württemberg (Germany) during the COVID-19 pandemic Sci. Rep.2024142491210.1038/s 41598-024-75084-y 39438540 PMC 11496798 · doi ↗ · pubmed ↗
- 2Petropoulou Z. Arkadopoulos N. Michalopoulos N.V. Breast Cancer and COVID-19: Challenges in Surgical management Cancers 202214536010.3390/cancers 1421536036358779 PMC 9653580 · doi ↗ · pubmed ↗
- 3Hawrot K. Shulman L.N. Bleiweiss I.J. Wilkie E.J. Frosch Z.A.K. Jankowitz R.C. Laughlin A.I. Time to treatment initiation for breast cancer during the COVID-19 pandemic JCO Oncol. Pract.20211753454010.1200/OP.20.0080733710914 PMC 8457793 · doi ↗ · pubmed ↗
- 4Eijkelboom A.H. de Munck L. Menke-van der Houven van Oordt C.W. Broeders M.J.M. van den Bongard D.H.J.G. Strobbe L.J.A. Mureau M.A.M. Lobbes M.B.I. Westenend P.J. Koppert L.B. Changes in breast cancer treatment during the COVID-19 pandemic: A Dutch population-based study Breast Cancer Res. Treat.202319716117510.1007/s 10549-022-06732-y 36334188 PMC 9638417 · doi ↗ · pubmed ↗
- 5Filipe M.D. van Deukeren D. Kip M. Doeksen A. Pronk A. Verheijen P.M. Heikens J.T. Witkamp A.J. Richir M.C. Effect of the COVID-19 pandemic on surgical breast cancer care in the Netherlands: A multicenter retrospective cohort study Clin. Breast Cancer 20202045446110.1016/j.clbc.2020.08.00232888855 PMC 7413119 · doi ↗ · pubmed ↗
- 6Wilke L.G. Nguyen T.T. Yang Q. Hanlon B.M. Wagner K.A. Strickland P. Brown E. Dietz J.R. Boughey J.C. Analysis of the impact of the COVID-19 pandemic on the multidisciplinary management of breast cancer: Review from the American Society of Breast Surgeons COVID-19 and Mastery registries Ann. Surg. Oncol.2021285535554310.1245/s 10434-021-10639-134431019 PMC 8384097 · doi ↗ · pubmed ↗
- 7Kara H. Arikan A.E. Dulgeroglu O. Tutar B. Tokat F. Uras C. Has the COVID-19 Pandemic Affected Breast Cancer Stage and Surgical Volume?Front. Surg.2022981110810.3389/fsurg.2022.81110835198597 PMC 8859320 · doi ↗ · pubmed ↗
- 8Cavalcante F.P. Abdala E. Weissmann L. dos Santos Ferreira C.E. Amorim G. Marques de Oliveira V. Guilgen G. Landeiro L. Rebello Pinho J.R. PulchinelliÁ.Jr. Impact of COVID-19 disease in early breast cancer management JCO Glob. Oncol.20228 e 210035710.1200/GO.21.0035735594492 PMC 9173577 · doi ↗ · pubmed ↗