Retrospective Analysis of Regorafenib Efficiency in Treatment of Metastatic Colorectal Cancer—Experience of Two Polish Comprehensive Cancer Centers
Magdalena Grabiec, Dominika Raźniewska, Tadeusz Kałużewski, Magdalena Krakowska, Barbara Radecka, Piotr Potemski

TL;DR
This study evaluated regorafenib's effectiveness in treating advanced colorectal cancer patients in Poland, finding similar results to previous trials but highlighting the need for better treatment strategies.
Contribution
The study provides real-world evidence of regorafenib's efficacy in a Polish patient cohort, emphasizing variability in outcomes and the need for personalized treatment strategies.
Findings
Median progression-free survival was 2.5 months and median overall survival was 5.8 months.
Disease stabilization was observed in five patients with a median duration of 5.6 months.
Results were comparable to the phase III CORRECT trial, with minor differences likely due to patient variability.
Abstract
Objectives: Colorectal cancer is a major public health concern, ranking third in incidence among all malignant tumors both in Poland and globally. We conducted a retrospective study to evaluate the effectiveness of regorafenib in patients with metastatic colorectal cancer ineligible for local therapy treated at two Polish comprehensive cancer centers between 2021 and 2024. Methods: The analysis included 29 patients who had previously received all standard therapies: fluoropyrimidines, oxaliplatin, and irinotecan (in a multi-agent regimen or sequentially) and bevacizumab (anti-VEGF therapy). In patients with tumors negative for KRAS, NRAS and BRAF mutations, cetuximab or panitumumab (anti-EGFR therapy) were also used. Results: The median progression-free survival (PFS) was 2.5 months, and the median overall survival (OS) was 5.8 months. Disease stabilization was observed in five…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
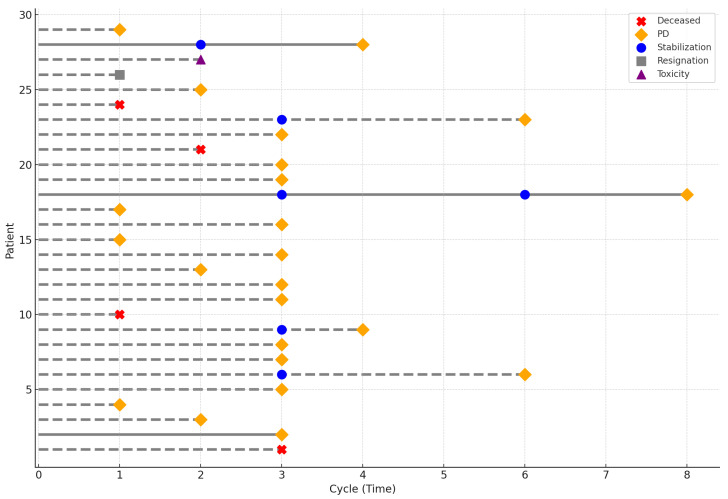 Figure 1
Figure 1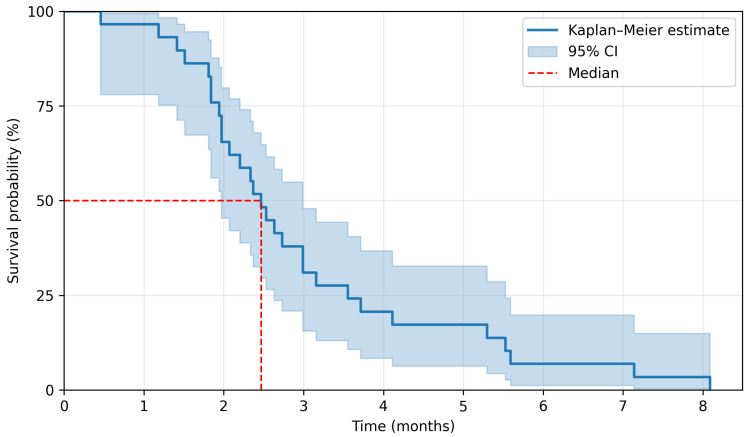 Figure 2
Figure 2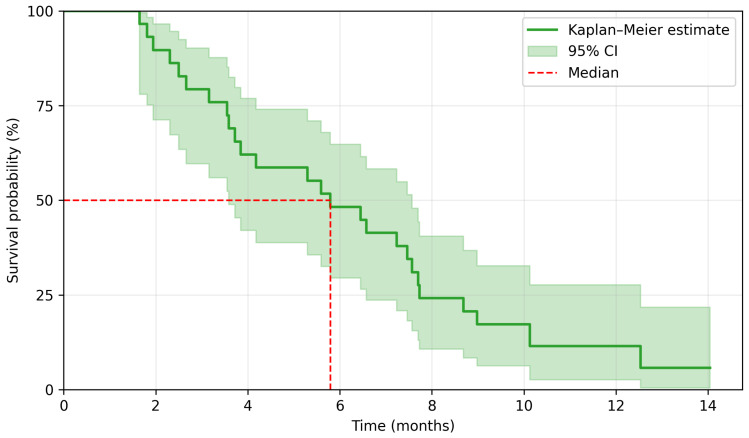 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Treatments and Studies · Advanced Breast Cancer Therapies · Melanoma and MAPK Pathways
1. Introduction
Colorectal cancer represents a significant public health problem, ranking third in terms of incidence among malignant neoplasms both in Poland and globally [1,2]. In Poland, 17,700 individuals were diagnosed with colorectal cancer in 2021 [2].
According to ESMO guidelines, 15–20% of patients present with metastatic disease at the time of diagnosis, and approximately 20–50% of patients with non-advanced disease will develop metastatic disease during the course of their illness [3].
In advanced disease, standard management is based on multi-drug chemotherapy, either combined with targeted agents or administered without them, as well as immunotherapy [3]. At the time of treatment qualification, therapeutic decisions are made considering the patient’s condition, comorbidities, preferences regarding the mode of treatment administration, and consent to potential adverse effects. Another critical factor influencing treatment strategy is the outcome of molecular testing, which includes the identification of mutations in the KRAS, NRAS, and BRAF genes, as well as the assessment of microsatellite instability/mismatch repair status.
Recent advancements in personalized medicine have enabled tailoring therapies to the molecular aberrations of tumors [4]. For patients with the BRAF V600E mutation, which occurs in 8–12% of cases, combination therapy with encorafenib and cetuximab can be considered based on the results of the BEACON study [5]. Another molecular aberration for which targeted therapy may be considered is HER2 overexpression, observed in 3–5% of patients [6]. Additionally, the KRAS G12C mutation, present in 3% of colorectal cancer cases, allows for the use of dual-drug regimens such as sotorasib and panitumumab, based on the phase III CodeBreak 300 trial [7], or adagrasib and cetuximab, based on the phase I/II KRYSTAL-1 trial [8]. Entrectinib and larotrectinib can be utilized in patients with NTRK1, NTRK2, or NTRK3 gene fusions, which occur in less than 1% of colorectal cancer cases [9]. Furthermore, based on the phase I/II basket trial Libretto-001, selpercatinib may be considered for patients with RET gene fusions, observed in fewer than 1% of cases [10].
For patients without the aforementioned molecular aberrations who had received all standard drugs and are in very good or good performance status and express a willingness to continue treatment, there are no clear guidelines regarding the continuation of therapy. One of the options to consider is regorafenib, a multikinase inhibitor, targeting kinases involved in tumor angiogenesis and oncogenesis as well as kinases associated with the tumor microenvironment. Regorafenib particularly inhibits mutated KIT kinase, a key driver of oncogenesis, thereby blocking tumor cell proliferation. Its efficacy after all approved standard therapies was confirmed in the phase III CORRECT trial [11]. This study was conducted between 2010 and 2011 across 114 centers in 16 countries. A total of 760 patients were enrolled and randomized in a 2:1 ratio into two groups: the first group received regorafenib, while the second group received a placebo. Both groups were provided with best supportive care. Eligible participants had to have life expectancy exceeding three months. The trial achieved statistical significance for both its primary and secondary endpoints, which were overall survival (OS) and progression-free survival (PFS), respectively.
The aim of our study was to evaluate the efficacy of regorafenib in patients from two Polish oncology centers by assessing PFS and OS, and compare them with the results of the CORRECT trial.
2. Materials and Methods
The study included 30 patients with inoperable metastatic colorectal cancer treated with regorafenib between 2021 and 2024 from two oncology centers (The Multidisciplinary Center of Oncology and Traumatology in Lodz and Tadeusz Koszarowski Cancer Center in Opole). One patient was excluded from the analysis as he did not attend the scheduled visit after the first treatment cycle and missed subsequent cycles. His survival exceeded the planned imaging evaluation after 3 months, leading to exclusion. The final analysis was conducted on data from 29 patients. All patients were initially qualified to receive the standard dose of 160 mg once daily for 3 weeks. The drug was reimbursed based on the individual approvals (the Emergency Access to Drug Technology).
Statistical analyses were performed to evaluate PFS and OS within a time-to-event framework. PFS was defined as the time from the start of treatment until disease progression or death from any cause, whichever occurred first. OS was defined as the time from the start of treatment until death from any cause. Patients who were alive at the last follow-up were censored at that time. The analysis included the calculation of median values of PFS and OS, along with the comparison of survival curves using Kaplan–Meier estimation. Data visualization was generated using Python (version 3) with the Matplotlib v3.10 and Lifelines v0.30 libraries.
3. Results
The median age of patients included in the study was 64 years. Baseline characteristics are presented in Table 1. Surgical resection of the primary tumor was performed in 72.4% of patients. All patients had metastatic disease, with 69% presenting distant metastases at initial diagnosis and 31% owing to relapse after previous radical local treatment. Prior to regorafenib treatment, 34.5% of patients had received more than three lines of therapy. Molecular testing for KRAS, NRAS, and BRAF mutations, as well as microsatellite instability (MSI), were not performed in one patient due to the difficulties in obtaining reliable material. Additionally, 44.8% of patients underwent HER2 expression testing by immunohistochemistry, all with negative results. None of the patients received immunotherapy due to the absence of microsatellite instability.
In the study group, seven patients received only one cycle of regorafenib, five received two cycles, twelve received three cycles, and five continued therapy beyond three cycles. Twenty-three patients discontinued treatment due to disease progression, while one patient discontinued due to treatment-related toxicity. Four patients died before disease progression could be confirmed. One patient voluntarily withdrew from treatment. The treatment course is illustrated in Figure 1.
The median duration of regorafenib treatment was 2.8 months. The last follow-up date for survival was 2 January 2025. There were 29 PFS events and 26 OS events. A median PFS (mPFS) was 2.5 months, and a median OS (mOS) was 5.8 months. The 3-month and 6-month PFS rate was 37.9% and 6.9%, respectively, whereas the 6-month and 12-month OS rate was 48.3% and 6.9%. Kaplan–Meier survival curves are presented in Figure 2 and Figure 3. Among 29 patients, 5 achieved disease stabilization as the best response to therapy, there were no partial or complete remissions. The median duration of disease stabilization was 5.6 months. The comparison of our results with the outcomes of the CORRECT trial is presented in Table 2.
4. Discussion
Managing treatment for patients in good performance status who have already received all standard therapies and whose tumors do not exhibit molecular aberrations amenable to targeted therapies is challenging. The CORRECT trial, published in 2013, provided evidence of the efficacy of regorafenib in such patients. In this study, regorafenib was shown to significantly improve OS and PFS compared to placebo. The use of regorafenib reduced the risk of disease progression by 51% (HR 0.49, 95% CI 0.42–0.58; p < 0.0001) and the risk of death by 23% (HR 0.77, 95% CI 0.64–0.94; p = 0.0052), extending the median PFS from 1.7 to 1.9 months and the median OS from 5 to 6.4 months. No patients achieved a complete response, while 5 patients receiving regorafenib achieved a partial response. Disease control was observed in 41% of patients, with a median duration of disease stabilization of 2 months compared to 1.7 months in the placebo group. A meta-analysis combining results from the CORRECT trial and three studies conducted in Asian populations [12,13,14] demonstrated a statistically significant improvement in OS (OR = 0.78; 95% CI = 0.65–0.94; p = 0.008) and PFS (OR = 0.52; 95% CI = 0.34–0.79; p = 0.002) compared with the control group [15]. The efficacy and safety of regorafenib have also been supported by European real-world data, including the French compassionate-use REBECCA cohort [16] and the Czech national registry-based analysis [17]. These findings are complemented by the international prospective observational CORRELATE study, which included a substantial number of European centers [18], as well as separate French cohort analysis [19]. Regorafenib was also investigated in the second-line setting in a phase II study that compared FOLFIRI combined with regorafenib versus FOLFIRI alone. The study demonstrated only a slight improvement in PFS (median: 6.1 vs. 5.3 months; HR 0.73, 95% CI = 0.53–1.01; p = 0.056); however, no benefit in OS was observed (HR 1.01, 95% CI = 0.71–1.44) [20]. In the Italian REALITY (GISCAD) study [21], clinical factors potentially identifying patients with a greater likelihood of benefit were explored, with the absence of liver progression and good early tolerability (without dose/schedule modifications) associated with improved outcomes. The patient characteristics in these cohorts appear broadly comparable to those in CORRECT and in our analysis. To the best of our knowledge, Polish centers were not represented in the above-mentioned studies.
The outcomes of the study conducted on the population from Polish oncology centers were comparable to those in the CORRECT trial. However, reliable comparison is not possible, as patients treated in real-word practice usually differ from those treated in controlled clinical trials. In the analyzed group, most patients had a performance status of 1 according to ECOG, compared to the registration trial, where patients with good and very good performance status were more evenly distributed. Additionally, the Polish population had a higher prevalence of rectal cancer—more than half compared to one-third of the CORRECT trial population with this diagnosis. Moreover, 34.5% of patients in the current study received more than three lines of treatment prior to regorafenib, compared to 49% in the 2013 trial. Thus, small numerical differences in mPFS and mOS seem to be negligible. Moreover, the difference in median PFS may be attributed to the timing of treatment response assessments, performed every 8 weeks in the registration trial but every 12 weeks in our study. Differences between the size of populations may also contribute to the observed discrepancies. The potential impact of improved supportive care quality for oncology patients since the time of the registration trial should also be considered.
For patients progressing on regorafenib or after exhausting available treatment options, fruquintinib emerges as a promising option. Approved by the FDA in 2023 [22] and by the EMA in June 2024 [23], fruquintinib is a selective VEGFR 1–3 kinase inhibitor that exerts its antitumor effects by inhibiting tumor angiogenesis. Its efficacy was confirmed in the phase III FRESCO-2 trial [24], a randomized study comparing fruquintinib + best supportive care (BSC) with placebo + BSC. This trial included 691 patients with metastatic colorectal cancer previously treated with standard therapies, including fluoropyrimidine, oxaliplatin, irinotecan, anti-EGFR agents (for KRAS, NRAS, and BRAF wild-type tumors), anti-VEGF agents, trifluridine/tipiracil, and immunotherapy for MSI-H tumors. Patients were stratified by prior therapy (trifluridine/tipiracil only, regorafenib only, or both), RAS genes status, and metastatic disease duration (≤18 months or >18 months). The primary endpoint was OS, with PFS as a key secondary endpoint. Fruquintinib significantly improved both endpoints, with a mOS of 7.4 months compared to 4.8 months in the placebo group (34% reduction in death risk) and a mPFS of 3.7 months versus 1.8 months (68% reduction in progression or death risk).
Another treatment approach after standard therapies could involve reintroducing previously used regimens [25]. Evidence suggests that irinotecan-based retreatment achieves a disease control rate (DCR) of 78.2%, compared to 57.8% for oxaliplatin retreatment [26,27]. However, oxaliplatin retreatment may not be feasible due to persistent neuropathy from prior therapy. Reintroduction of anti-EGFR agents in unselected patients is considered ineffective [28].
5. Limitations of Our Study
The main limitation of our study is a very small number of patients. This results from the limited availability of regorafenib at that time.
6. Conclusions
This analysis focused on patients who had completed standard treatment. The efficacy of regorafenib was evaluated in a population of Polish patients with metastatic colorectal cancer. Despite being a preliminary evaluation based on a small patient cohort our study confirmed the results of the CORRECT trial. Decisions regarding treatment after standard therapies remain challenging and, given the current state of knowledge, should be guided by the anticipated benefits and the side effect profile of available options. Fruquintinib has recently emerged as an additional important therapeutic option. Further comparative studies are necessary to determine the optimal treatment strategies in patients with chemorefractory disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global Burden of Disease 2019 Cancer Collaboration Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life Years for 29 Cancer Groups From 2010 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019 JAMA Oncol.2022842044410.1001/jamaoncol.2021.698734967848 PMC 8719276 · doi ↗ · pubmed ↗
- 2Didkowska J. Barańska K. Miklewska M.J. Wojciechowska U. Cancer Incidence and Mortality in Poland in 2023 Nowotwory. J. Oncol.202474759310.5603/njo.99065 · doi ↗
- 3Cervantes A. Adam R. RosellóS. Arnold D. Normanno N. Taïeb J. Seligmann J. Baere T.D. Osterlund P. Yoshino T. Metastatic Colorectal Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up Ann. Oncol.202334103210.1016/j.annonc.2022.10.00336307056 · doi ↗ · pubmed ↗
- 4Bashraheel S.S. Domling A. Goda S.K. Update on Targeted Cancer Therapies, Single or in Combination, and Their Fine Tuning for Precision Medicine Biomed. Pharmacother.202012511000910.1016/j.biopha.2020.11000932106381 · doi ↗ · pubmed ↗
- 5Kopetz S. Grothey A. Yaeger R. Cutsem E.V. Desai J. Yoshino T. Wasan H. Ciardiello F. Loupakis F. Hong Y.S. Encorafenib, Binimetinib, and Cetuximab in BRAF V 600E–Mutated Colorectal Cancer N. Engl. J. Med.20193811632164310.1056/NEJ Moa 190807531566309 · doi ↗ · pubmed ↗
- 6Ahcene Djaballah S. Daniel F. Milani A. Ricagno G. Lonardi S. HER 2 in Colorectal Cancer: The Long and Winding Road From Negative Predictive Factor to Positive Actionable Target Am. Soc. Clin. Oncol. Educ. Book 20224221923210.1200/EDBK_35135435580290 · doi ↗ · pubmed ↗
- 7Fakih M.G. Salvatore L. Esaki T. Modest D.P. Lopez-Bravo D.P. Taieb J. Karamouzis M.V. Ruiz-Garcia E. Kim T.-W. Kuboki Y. Sotorasib plus Panitumumab in Refractory Colorectal Cancer with Mutated KRAS G 12CN. Engl. J. Med.20233892125213910.1056/NEJ Moa 230879537870968 · doi ↗ · pubmed ↗
- 8Yaeger R. Weiss J. Pelster M.S. Spira A.I. Barve M. Ou S.-H.I. Leal T.A. Bekaii-Saab T.S. Paweletz C.P. Heavey G.A. Adagrasib with or without Cetuximab in Colorectal Cancer with Mutated KRAS G 12CN. Engl. J. Med.2023388445410.1056/NEJ Moa 221241936546659 PMC 9908297 · doi ↗ · pubmed ↗