When Should Physicians Consider Referring Elderly Patients with Suspected PFO-Related Stroke for Device Closure?
Alisha Varia, David Roberts

TL;DR
This paper examines whether closing a patent foramen ovale (PFO) is effective in preventing stroke recurrence in elderly patients, finding potential benefits but highlighting the need for better studies.
Contribution
The study evaluates the efficacy and safety of PFO closure in elderly patients with cryptogenic stroke, a population with limited evidence.
Findings
PFO closure reduced recurrent cerebral ischaemia by 45% and mortality by 85% in elderly patients.
Closure groups had lower disability scores but higher incidence of new-onset atrial fibrillation.
Study quality was limited by heterogeneous protocols and baseline imbalances between groups.
Abstract
Background: Guidelines recommend patent foramen ovale (PFO) closure for secondary prevention after cryptogenic stroke in patients aged 18–65 years, but there is limited evidence to guide management of elderly adults. This research aims to assess the efficacy, safety and methodological quality of trials comparing secondary prevention PFO closure with medial therapy alone (MTA) in patients aged ≥ 60 years. Methods: A PubMed search identified four studies comparing PFO closure with MTA in elderly patients—PFOSK (South Korea), PT (Taiwan), DEFENSE (South Korea) and PFOG (Germany). Primary analyses evaluated study quality—patient selection, allocation, crossover and adherence. Secondary analyses compared recurrent cerebral ischaemia, mortality, new-onset atrial fibrillation (AF) and disability. Results: In 644 patients ≥ 60 years old, PFO closure was associated with a 45% (95% CI 0.35–0.86,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
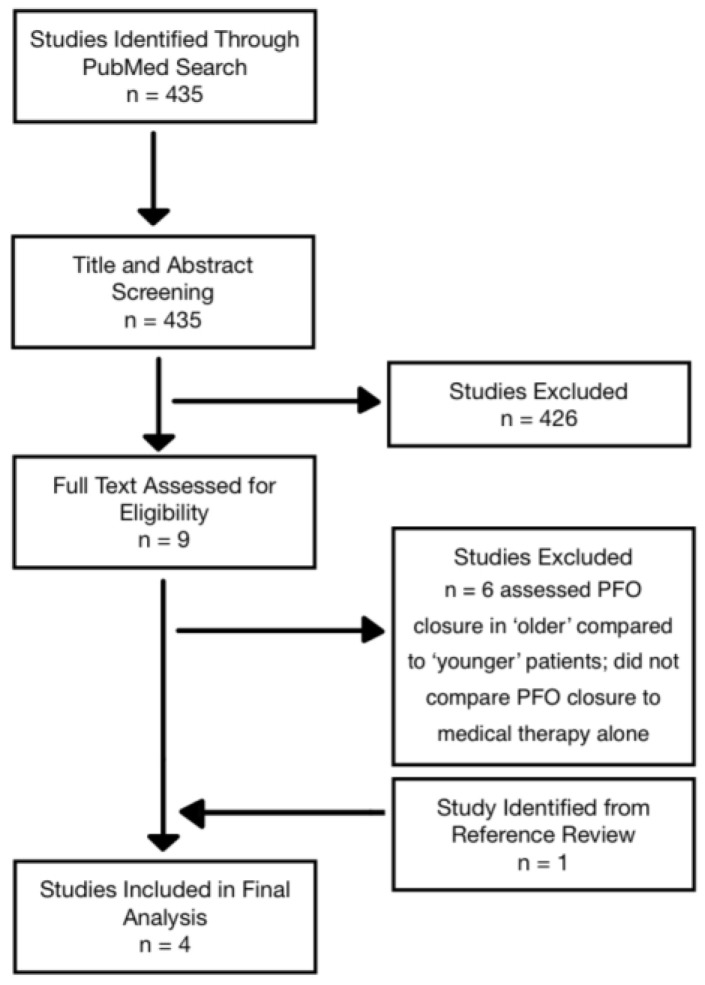 Figure 1
Figure 1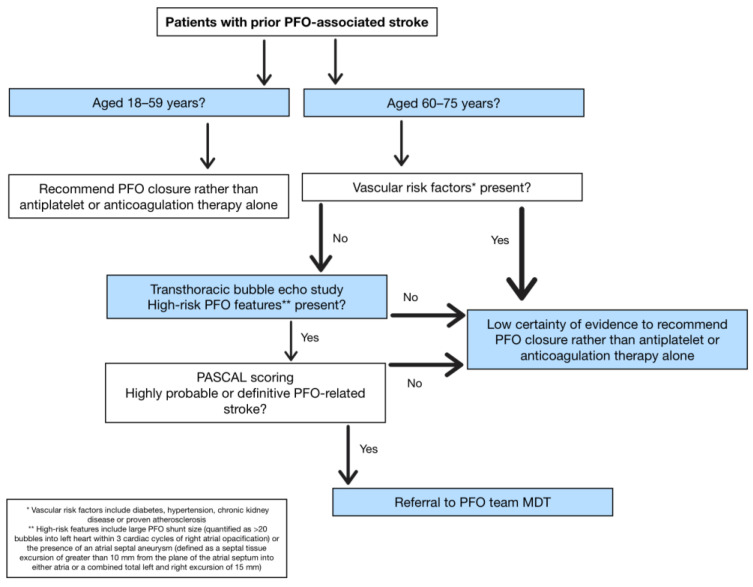 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Cerebrospinal fluid and hydrocephalus · Intracranial Aneurysms: Treatment and Complications
1. Introduction
ESC guidelines [1] recommend patent foramen ovale (PFO) closure as secondary prevention in patients aged 18 to 65 years with a cryptogenic stroke. They suggest case-by-case decision-making when patients over 65 present with this condition, providing no single recommendation for treatment [1,2]. NHS England [2] only commissions PFO closure as a secondary prevention in patients aged 60 years and under. Probability of causation has traditionally been determined using the paradoxical embolism (RoPE) score, with scores of seven and above indicating a greater likelihood of PFO causation for a cryptogenic stroke [3].
PFO presence ranges from 16 to 18% in patients above 55 years with a cryptogenic stroke [4], three times more prevalent compared to those patients with stroke of known cause [5]. In a systematic review and meta-analysis by Mazzuco et al., planned stratification by age showed a 150% increased risk of recurrent stroke in the presence of PFO in patients over 65 [6]. Despite this, there remains limited trial evidence exploring the benefits of PFO closure in elderly patients suffering a cryptogenic stroke.
This review aims to evaluate evidence for PFO closure in adults aged ≥ 60 years who experience PFO-related cerebrovascular events, specifically compared to those who receive secondary prevention with antiplatelet or anticoagulation therapy alone.
2. Materials and Methods
2.1. Literature Search and Paper Selection
This review was conducted as a structured narrative review incorporating systematic elements. Because evidence for PFO closure in adults ≥60 years is sparse, we intentionally adopted a broad search strategy to maximise sensitivity. The predefined search terms (Table 1) produced 435 results, of which 426 were excluded during title and abstract screening due to irrelevance arising from this broad approach (Figure 1). Additional six studies were excluded because they compared elderly versus younger closure populations rather than closure versus medical therapy alone. Screening of study references yielded an additional paper, comprising age-based subgroup analyses of a previous randomised controlled trial (RCT). Four studies met final inclusion criteria. A PRISMA flow diagram was used to transparently document the selection process.
2.2. Analysis
Primary analysis includes the methodological quality of included studies, assessed according to predefined criteria—patient selection, treatment allocation, crossover between treatment groups and adherence to assigned treatment. Secondary analysis pooled available event data for recurrent stroke and TIA, new-onset atrial fibrillation (AF), peri-operative complications and death. Subgroup analyses then determine any stratification factors associated with benefits from PFO closure in elderly patients. Measurements of disability, such as modified Rankin Scale (mRS), are reported.
Statistical analyses on pooled event rates were obtained from Wald Z-tests applied to Mantel–Haenszel-derived pooled relative risk (RR).
3. Results
3.1. Quality of Included Studies
Trials without given names were referred to as PFO(x), with “x” representing the country of conduct. The four studies included are PFOSK (South Korea—Lee at al., 2024) [7], PFOT (Taiwan—Chen et al., 2023) [8], DEFENSE (Kwon et al., 2021) [9] and PFOG (Germany—Poli et al., 2021) [10]. These studies compared the efficacy of PFO closure, followed by at least three months of dual antiplatelet therapy (DAPT), with standard medical therapy alone (MTA), which included antiplatelet agents and/or anticoagulation therapy. PFO was diagnosed by echocardiography and bubble study in all studies except PFOT, which used a transcranial Doppler. The Cardia PFO occluder was used in PFOT and Amplatzer PFO occluder in DEFENSE and PFOG (Table 2 and Table A1). A range of devices including Amplatzer, Cocoon and Figulla Flex II PFO occluders were used in PFOSK.
PFOT and PFOG included all patients over the age of 18, with planned subgroup analyses for patients ≥ 60 or >60 years, respectively. DEFENSE was a post hoc subgroup analysis of patients aged 60 years or older from the original study, while PFOSK specifically included those aged 60 years or older. DEFENSE only included patients with high-risk PFO features, defined as the presence of atrial septal aneurysm (ASA) or hypermobility and/or PFO ≥ 2 mm in diameter visualised on transoesophageal echocardiography. PFOG and PFOSK included planned subgroup analysis of patients with ‘high-risk’ echocardiographic features for thromboembolism.
Primary outcome in PFOT, PFOSK and DEFENSE was a composite of recurrent cerebral ischaemic events (ischaemic stroke (IS) or TIA), with additional all-cause mortality in PFOT. Primary outcome in PFOG was recurrent IS and intracranial haemorrhage. Cerebral ischaemia was assessed using magnetic resonance imaging (MRI) and angiography (MRA) or computed tomography angiography (CTA).
PFOSK and PFOT performed patient allocation using patient-centred multidisciplinary consensus and shared decision-making with the patient and family (Table 3). DEFENSE performed randomised 1:1 allocation, and PFOG used a predefined standard operating procedure (SOP) with an age-cutoff of 70 years for closure of a PFO with ‘high-risk’ features.
Adherence to MTA or percutaneous closure was only reported in PFOG, where as-treated analyses were performed. A total of 28 and 17 patients from closure and MTA groups, respectively, crossed over, either through patient- or physician decision. PFOSK reported 2.2% of MTA patients were taking no antithrombotic therapy at 30 days after stroke.
PFOG and PFOSK reported patients in the MTA groups were significantly older than those in PFO closure groups at baseline. Both described a greater prevalence of vascular risk factors—hypertension (HTN), smoking history, hyperlipidaemia, obesity, diabetes, coronary artery disease (CAD) or prior myocardial infarction (MI), chronic kidney disease (CKD), prior deep vein thrombosis (DVT) or pulmonary embolism (PE), migraine or cancer history—within MTA groups, although none are significantly different. DEFENSE reported no significant differences between baseline characteristics of closure and MTA groups.
PFOSK and PFOT reported ‘high-risk’ PFO features for thromboembolism. In PFOSK, there was a low prevalence of large shunt size in MTA group, while 22% and 70% of the closure group also did not have a large shunt or ASA, respectively. The PFOT MTA group had a greater prevalence of small shunts (63% vs. 20% in the closure group).
Baseline median mRS was not significantly different between the closure group and MTA (3 vs. 2, respectively, p = 0.989) in PFOT; meanwhile, in PFOG, ‘high-risk’ closure group had a similar number of patients with a baseline mRS score of 0 compared to ‘high-risk’ MTA (88% vs. 89%, respectively).
3.2. Secondary Outcomes
A total of 966 patients were included in the four studies, 644 years old, of which 392 were assigned to MTA and 252 to the PFO closure arm.
Collated incidence of recurrent cerebral ischaemia in all four studies was 9.1% in closure arm (n = 23) and 15.6% in MTA (n = 65)—this includes all-cause mortality data from PFOT due to sole reporting of composite primary outcome event rates. This corresponds to a significant reduction in recurrent cerebral ischaemia following PFO closure, with an RR of 0.55 (95% CI 0.35–0.86, p = 0.0091). Mortality rate, combining all studies except PFOT, to prevent duplicate use of results, was 1.1% following PFO closure (n = 3) and 7.9% in the MTA (n = 31), RR 0.15 (95% CI 0.05–0.49, p = 0.0016) in patients over 60 years.
New-onset AF occurred in 18 patients following PFO closure and in 13 patients in the MTA (RR 2.15, 95% CI 1.07–4.32, p = 0.0306). A total of 15 and 13 events with closure and MTA, respectively, were from PFOSK, which was the only paper to report a significant difference in the 5-year event rate between groups (p = 0.026). However, PFOT found no significant difference in new-onset AF between elderly and younger patient groups. DEFENSE only reported two cases of AF and did not specify the age or treatment arm. Modified Rankin scale (mRS) score at follow-up was reduced following PFO closure, i.e., better outcomes, compared to MTA in PFOT (1 (IQR 0–2) vs. 1 (IQR 0–3); p = 0.002) and PFOG (mRS score of 0/1—77% in high-risk closure group vs. 68% in high-risk MTA; RR 0.72).
Subgroup analyses identified that elderly patients with high-risk PFO features (aneurysmal septum, large shunt) benefit mostly from PFO closure. In PFOT, a significant reduction in ischaemic stroke risk was found with closure (HR 0.36, 95% CI 0.18–0.75, p = 0.006), compared to the overall cohort (HR 0.52, p = 0.034). PFOSK also showed a significant reduction in ischaemic stroke with PFO closure in propensity-score matched, high-risk patients (HR 0.47, 95% CI 0.23–0.95, p = 0.035), compared to a non-significant risk decrease in the overall cohort (HR 0.58, p = 0.107). DEFENSE showed a high incidence of TIA/stroke in patients over 70 years (HR 11.64, p = 0.03) and these benefited the most from PFO closure, but this finding was limited by a large confidence interval due to a small sample size.
4. Discussion
4.1. Summary of Evidence
We report a dual analysis as follows: examination of trial evidence quality and comparison of PFO closure versus medical management in patients over 60 years of age. This approach was driven by the limited studies focusing solely on elderly patients and the lack of guideline recommendations for the management of these patients.
The collated findings provide evidence that PFO closure in elderly patients decreases the incidence of recurrent IS and TIA and reduces mortality and disability scores compared to medical therapy alone. However, this evidence is limited by the comparability of trial protocols and results, including variations in treatment allocation and patient characteristics, medical therapies and closure devices, result analysis and treatment adherence.
Subgroup analyses in PFOSK and DEFENSE show that elderly patients with high-risk PFO features—ASA or large shunt size (≥2 mm on TEE)—may have the greatest benefit from closure. The probability of incidental PFO finding following cryptogenic stroke is 48% in those over 55, compared to just 20% in younger patients, both of which reduced to 26% and 9%, respectively, when a concomitant ASA was detected [4].
4.2. Comparison with Current Guideline Recommendations
Current ESC guidelines [1] strongly recommend PFO closure as secondary prevention for cryptogenic stroke in adults aged 18–65 years when a high probability of PFO causality is established. For individuals > 65 years, the guidelines advise case-by-case decision-making, acknowledging the absence of robust evidence in this age group accounting for personal confounders of surgical or medical intervention [1]. NHS England policy [2] similarly restricts percutaneous PFO closure to patients ≤ 60 years, reflecting comparable concerns regarding diagnostic certainty and increasing atherosclerotic risks in elderly populations.
Both ESC and NHS guidance [1,2] highlight the use of the RoPE score to estimate the likelihood of a PFO-related stroke but also note its limitations—particularly the lack of external validation. Although the guidelines acknowledge that other tools may complement RoPE scoring, they do not specify alternatives, such as the PASCAL classification system.
The evidence evaluated in this review suggests that selected elderly adults may benefit from percutaneous PFO closure, consistent with findings in younger populations. These findings reinforce the need for rigorous trials in those over 60 years of age to inform guideline updates. Until such data are available, incorporating anatomical high-risk features may assist in defining causal attribution of cerebral ischaemia and support personalised decision-making in elderly patients.
4.3. Strengths
This review uniquely emphasises methodological quality as its primary objective. By combining structured selection criteria, transparent reporting and pooled outcome assessment, it provides a unified appraisal of the available evidence base and highlights methodological issues that impede clinical translation.
4.4. Limitations of Trial Evidence
The interpretation of trial evidence in elderly adults remains constrained by several methodological and practical issues. Firstly, medical therapies and closure devices and procedures were not standardised across or within studies, with heterogeneity in anti-thrombotic regimes, closure devices and post-operative management. This variability limits comparability and introduces potential bias in outcome interpretation.
Secondly, adherence of assigned treatment was inconsistent—for example, forty-five patients in PFOG crossed over between treatment arms, while 2.2% of MTA patients in PFOSK were not on any antithrombotic therapy at 30 days. Those that crossed over tended to be younger and possess fewer risk factors, yet had larger shunts, presenting a selection bias that paradoxically produced a non-significant higher recurrence rate with closure. Furthermore, treatment allocation in PFOG was determined by a procedural age cut-off of 70 years, with analyses performed on a 60-year threshold, further complicating interpretation.
Thirdly, marked differences in baseline characteristics between treatment arms were consistently observed. Patients in MTA groups were generally elderly, with greater prevalence of vascular comorbidities such as HTN, diabetes and CAD, whereas those in closure groups often had larger shunt sizes and ASA—features associated with higher embolic risks. These imbalances confound results as vascular risk factors of PFO-independent determinants of recurrent stroke.
Event rates across studies were generally low, resulting in wide confidence intervals and limited statistical power to detect meaningful differences. Mortality outcomes were inconsistently reported, precluding firm attribution to PFO closure, medical therapy or recurrent stroke. Importantly, due to limited available data, pooled analyses necessarily combined intention-to-treat and as-treated, which introduces bias. This reflects deficiencies in reporting rather than analytic choice and highlights the need for standardised methodologies in future research.
The observed two-fold increase in new-onset AF following PFO closure may partially reflect greater baseline risk in elderly patients with pre-existing cardiovascular disease.
Collectively, these limitations highlight the need for adequately powered RCTs specifically designed for patients over 60 years with standardised endpoint definitions, device and medical therapy protocols and stratification by high-risk PFO features.
5. Recommendations and Clinical Implications
The findings in this review support the consideration of patients aged 60–75 years presenting with a cryptogenic stroke without vascular risk factors (diabetes, HTN, CKD) or proven atherosclerosis for PFO closure (Figure 2). Transthoracic bubble echo study should focus on identifying large PFO shunt size (quantified as >20 bubbles into left heart within three cardiac cycles of right atrial opacification [11]) and the presence of an ASA (defined as a septal tissue excursion of greater than 10 mm from the plane of the atrial septum into either atria or a combined total left and right excursion of 15 mm [12]).
Elderly patients inadvertently have a lower RoPE score due to age and comorbidity scoring, highlighting its limitation to determine eligibility for PFO closure. PASCAL is an alternative assessment tool that combines RoPE scores with the presence of high-risk PFO features [13]. Meta-analysis showed a greater reduction in risk of recurrent ischaemic stroke when using PASCAL categorisation to select patients for PFO closure age 18–60 years [13]. We suggest PASCAL classification (Table 4) for determining causal attribution of recurrent cerebral ischaemia and selection of elderly patients for potential PFO closure, aligned with current guidelines. Those patients scored with highly probable or definitive outcome of PFO-related stroke may be considered for PFO closure by referral to the PFO team MDT. All decision-making should also consider patient preference and weighing individual risk-to-benefit analysis.
Future studies of PFO closure in patients > 60 years of age must include adequately powered RCTs with:
- standardised medical and closure protocols
- predefined upper age limits
- consistent ITT reporting
- stratification by high-risk PFO anatomy
- robust follow-up and adherence reporting
Such trials are essential to generate definitive recommendations for patients ≥ 60 years.
6. Conclusions
Evidence from the four studies evaluating PFO closure in patients aged ≥ 60 years demonstrates a consistent trend towards reduced recurrent cerebral ischaemia, lower mortality and improved functional outcomes compared with MTA. However, interpretation must account for substantial heterogeneity between studies. While pooled analyses suggest meaningful benefit, differences in closure devices, medical regimens, participant allocation and baseline comorbidities—combined with low event rates—introduce uncertainty and limit generalizability.
Importantly, the greatest benefit appears concentrated in those with ‘high-risk’ PFO features—large shunt size and ASA—supporting the use of detailed assessment tools such as PASCAL to evaluate causality.
Taken together, the existing evidence supports MDT referral for selected elderly individuals, but it remains insufficient to form definitive guideline recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pristipino C. Sievert H. D’Ascenzo F. Mas J.L. Meier B. Scacciatella P. Hildick-Smith D. Gaita F. Toni D. Kyrle P. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism Eur. Heart J.2019403182319510.1093/eurheartj/ehy 64930358849 · doi ↗ · pubmed ↗
- 2NHS England Clinical Commissioning Policy: Percutaneous Patent Foramen Ovale Closure for the Prevention of Recurrent Cerebral Embolic Stroke in Adults (Around the Age 60 Years and Under)NHS England London, UK 2019 Available online: https://www.england.nhs.uk/commissioning/wp-content/uploads/sites/12/2019/07/Clinical-Commissioning-Policy_Percutaneous-patent-foraman-ovale-closure-for-the-prevention-of-recurrent-cerebr.pdf(accessed on 2 April 2025)
- 3Kavinsky C.J. Szerlip M. Goldsweig A.M. Amin Z. Boudoulas K.D. Carroll J.D. Coylewright M. Elmariah S. Mac Donald L.A. Shah A.P. SCAI guidelines for the management of patent foramen ovale J. Soc. Cardiovasc. Angiogr. Interv.2022110003910.1016/j.jscai.2022.10003939131947 PMC 11307505 · doi ↗ · pubmed ↗
- 4Alsheikh-Ali A.A. Thaler D.E. Kent D.M. Patent foramen ovale in cryptogenic stroke: Incidental or pathogenic?Stroke 2009402349235510.1161/STROKEAHA.109.54782819443800 PMC 2764355 · doi ↗ · pubmed ↗
- 5Handke M. Harloff A. Olschewski M. Hetzel A. Geibel A. Patent foramen ovale and cryptogenic stroke in older patients N. Engl. J. Med.20073572262226810.1056/NEJ Moa 07142218046029 · doi ↗ · pubmed ↗
- 6Mazzucco S. Li L. Rothwell P.M. Prognosis of cryptogenic stroke with patent foramen ovale at older ages and implications for trials: A population-based study and systematic review JAMA Neurol.2020771279128710.1001/jamaneurol.2020.194832628255 PMC 7550974 · doi ↗ · pubmed ↗
- 7Lee P.H. Kim J.-S. Song J.-K. Kwon S.U. Kim B.J. Lee J.S. Sun B.J. Woo J.S. Ann S.H. Suh J.W. Device closure or antithrombotic therapy after cryptogenic stroke in elderly patients with high-risk patent foramen ovale J. Stroke 20242624225110.5853/jos.2023.0326538836271 PMC 11164578 · doi ↗ · pubmed ↗
- 8Chen P.-L. Wang C.-S. Huang J.-A. Fu Y.-C. Liao N.-C. Hsu C.-Y. Wu Y.-H. Patent foramen ovale closure in non-elderly and elderly patients with cryptogenic stroke: A hospital-based cohort study Front. Neurol.202314119001110.3389/fneur.2023.119001137260604 PMC 10228363 · doi ↗ · pubmed ↗