Comparison Between RIRS and Mini-PCNL in the Treatment of Kidney Stones Exceeding 15 mm: Outcome Evaluation and Cost Analysis
Paolo Pietro Suraci, Andrea Fuschi, Manfredi Bruno Sequi, Fabio Maria Valenzi, Alice Antonioni, Onofrio Antonio Rera, Yazan Al Salhi, Damiano Graziani, Giorgio Martino, Giuseppe Candita, Filippo Gianfrancesco, Paolo Benanti, Cosimo De Nunzio, Giorgio Bozzini, Michele Di Dio

TL;DR
The study compares two kidney stone treatments, RIRS and mini-PCNL, finding that mini-PCNL is more cost-effective and achieves better stone-free results.
Contribution
This study provides a detailed cost and outcome comparison of RIRS and mini-PCNL for kidney stones over 15 mm using a micro-costing approach.
Findings
Mini-PCNL had a higher stone-free rate (94.7%) compared to RIRS (88.7%).
Mini-PCNL was more cost-efficient with lower total costs per treated patient.
Disposable materials were the main cost driver for both procedures.
Abstract
Background/Objectives: The optimal surgical approach for kidney stones (KS) measuring 15–20 mm remains debated. RIRS and mini-PCNL are both effective options, but they differ in invasiveness, resource use, and cost. This study aimed to compare perioperative outcomes and hospital costs of RIRS and mini-PCNL using a micro-costing approach. Methods: This retrospective study included patients with KS > 15 mm in diameter who were treated between January 2021 and December 2023 at the Department of Urology, Sapienza University of Rome-Polo Pontino. Clinical parameters, operative time (OT), length of stay (LoS), complications, and stone-free rate (SFR) were compared. Costs were estimated using a micro-costing method, including disposable materials, operating room (OR) time (3.9 EUR/min), imaging, and hospitalization (334 EUR/day). The total cost per treated and per SF patient was calculated for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
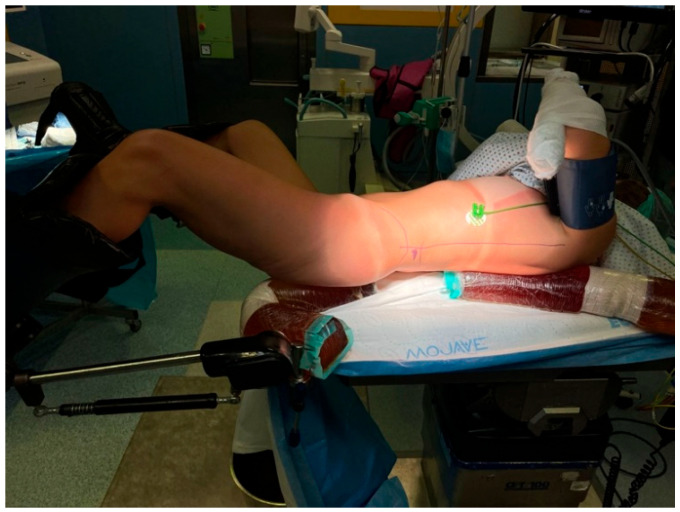 Figure 1
Figure 1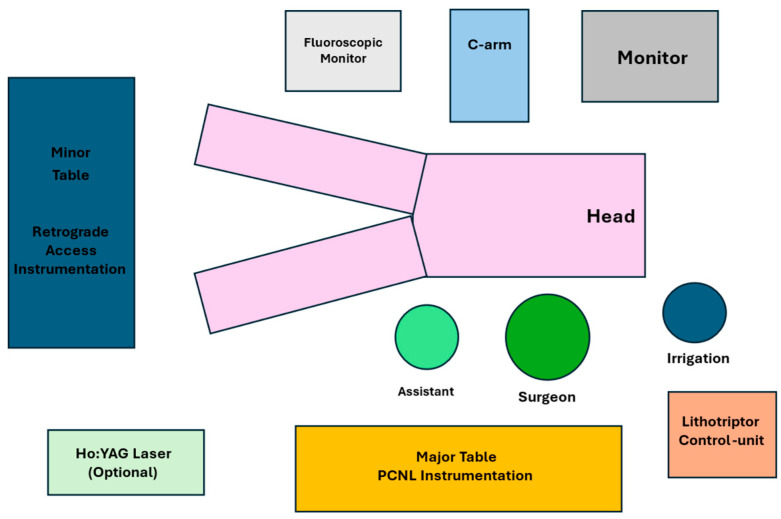 Figure 2
Figure 2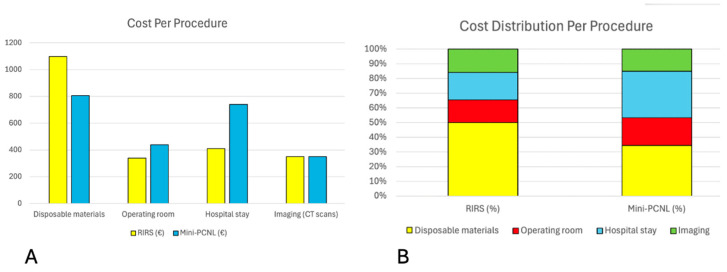 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Hemostasis and retained surgical items · Acute Kidney Injury Research
1. Introduction
Urolithiasis, in general, including kidney stones (KS), is among the most common and ancient urinary tract pathologies, representing a significant public health concern [1]. The incidence of kidney stones depends on geographical, climatic, ethnic, dietary, and genetic factors. In Italy, new cases are estimated to be around 100,000 per year [2,3]. In the general population, KS affects approximately 10% of males and 5% of females, with the majority occurring between ages 30 and 50, leading to significant complications and discomfort. In countries with a high Human Development Index (HDI), such as Sweden, Canada, or the United States, the prevalence of kidney stones is exceptionally high and continues to increase [1,4,5,6]. The main techniques used to treat urinary stones are extracorporeal shock wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), and retrograde endoscopic interventions, including ureteroscopy (URS) and retrograde intrarenal surgery (RIRS). Indications for laparoscopic and robot-assisted surgery remain for the treatment of large “staghorn” stones associated with concurrent need for urinary tract reconstruction [i.e, pyelo-ureteral junction (PUJ) stenosis] [7]. According to the European Association of Urology (EAU) guidelines, PCNL is preferable to RIRS or ESWL for stones larger than 20 mm. Conversely, RIRS or ESWL may be preferred for stones smaller than 10 mm [8]. However, for those with diameters between 10 and 20 mm, there is no definitive preference between PCNL and RIRS. According to the American Urological Association (AUA) guidelines, urologists should propose PCNL as the first-line therapy for overall stone diameters > 20 mm (Dmax); otherwise, RIRS might be considered [9]. Treatment options varied widely among surgeons, facilities, and even across countries and continents. It is also well known that the diagnosis-related group (DRG) system assigns RIRS and PCNL to different reimbursement levels within the National Health Service, favoring the latter [10]. In an era where optimizing expenditures and excellence in patient care are crucial, it is essential to consider the actual economic value of patient care. This study aims to compare RIRS and mini-PCNL with respect to perioperative outcomes and associated costs in treating KS ≥ 15 mm.
2. Materials and Methods
2.1. Study Design, Population, and Data Collection
The study was conducted retrospectively by examining the database and medical records of patients who underwent RIRS and mini-PCNL for kidney stones between January 2021 and December 2023 at the Department of Urology of Sapienza University of Rome-Polo Pontino, ICOT, in Latina. Up to April 2022, PCNL procedures were not performed in our department; therefore, patients treated during this period underwent RIRS exclusively. After the introduction of the mini-PCNL program, both procedures were available, and the choice of technique was primarily determined by the availability of trained personnel and equipment rather than specific stone or patient characteristics. The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (UROUNIVLT_OCT20/5821 approved on 12 October 2020). Inclusion criteria were as follows: age ≥ 18 years; and patients with a single KS or multiple adjacent calculi with a Dmax ≥ 15 mm. Patients undergoing concurrent ureteral lithotripsy, those with multiple non-contiguous KS, those with bilateral KS, those with kidney and/or ureter abnormalities, and those with incomplete data were excluded from the study. All patients underwent preoperative abdominal computed tomography (CT) and urine examination with culture. Patients received antibiotic therapy for preoperative infection based on antibiogram results and sensitivity testing. Expert surgeons (with >than 150 cases in both RIRS and mini-PCNL) performed all procedures (P.P.S., A.F., and Y.A.S.). The population was divided into two groups based on the treatment received: Group A (RIRS) and Group B (mini-PCNL). For each patient, the following data were collected: age, gender, body mass index (BMI), preoperative and 24 h postoperative hemoglobin (Hb), preoperative and 24 h postoperative serum creatinine, preoperative and postoperative leukocyte count (white blood cells, WBC), preoperative pharmacological therapy, comorbidities, number of stones, stone Dmax, location and density of stones assessed by CT in Hounsfield units (HU), renal anomalies, operative time (OT), number of procedures per patient, length of hospital stay (LoS), and complications according to Clavien–Dindo classification. Patients were re-evaluated 30 days after the procedure using non-contrast CT of the abdomen and pelvis to assess the stone-free rate (SFR). Absolute SFR was defined as the complete absence of visible residual fragments. SFR included clinically insignificant residual fragments (CIRF), which were the presence of residual fragments ≤ 4 mm. This definition was used as the primary outcome measure.
2.2. Surgical Technique and Instrumentation Used in RIRS
The procedure was performed as a one-day surgery based on the patient’s clinical condition. Under general anesthesia, the patient is placed in the lithotomy position. The bladder is accessed directly with a semi-rigid 7.5 Fr ureteroscope. An exploratory ureteroscopy is performed after inserting a Nitinol guidewire (Sensor-Boston Scientific, Marlborough, MA, USA) coated in polytetrafluoroethylene (PTFE) and designed for tactile feedback with a hydrophilic tip in the ureter. A10/12 Fr Rocamed dual-lumen ureteral is positioned under fluoroscopic guidance on the guidewire. The disposable flexible ureteroscope (PUSEN^®^ 7.5 Fr, Johns Creek, GA, USA) was used with Holmium Laser (Lumenis Pulse™ 100H, Yokneam, Israel) to perform lithotripsy. The stone is thus fragmented/pulverized after the laser is set according to the characteristics of the stone formation. A 365 µm laser fiber was routinely employed, whereas a 200 µm fiber was preferred for lower calyceal stones to enhance deflection and maneuverability. At the end of the procedure, a double-J stent is placed, and a 16/18 Fr Foley catheter is placed, which will be removed on postoperative day (POD) 1.
2.3. Surgical Technique and Instrumentation Used in the Mini-PCNL
The procedure was performed during routine admission, with discharge on POD2. Under general anesthesia, the patient is then positioned supine in the modified Valdivia–Galdakao position (Figure 1).
The typical OR setup is illustrated in Figure 2. Two instrument tables are prepared: a “lower” table and an “upper” table. The lower table contains all equipment required for retrograde access, including a single sterile drape, a 22 Ch rigid cystoscope with a camera head and light source, a 0.035-inch straight hydrophilic guidewire, a 4.8 Fr straight ureteral catheter, a 60 mL Luer-lock syringe prefilled with diluted contrast medium, and additional sterile gloves. The upper table is reserved for the mini-PCNL phase and includes a sterile C-arm drape, a 0.035-inch guidewire, a 12 Fr semi-rigid nephroscope with 6° optics, a 16 Fr 13 cm Clear Petra suction sheath, a stone-collection container, a Holmium:YAG laser with a 550 µm fiber, and a nephrostomy set comprising fascia dilators up to 14 Fr, an 18 G Chiba needle, and an 8 Fr nephrostomy catheter. The procedure begins with placing a 4.8 Fr × 74 cm ureteral catheter into the PUJ over a guidewire using a 22 Fr Storz rigid cystoscope. An 18 Fr Foley catheter is then inserted for bladder drainage. The ureteral catheter is used to perform retrograde pyelography and guide tract dilation for percutaneous puncture. The percutaneous phase is performed under ultrasound and fluoroscopic guidance. After successful puncture, a guidewire is advanced into the ureter, and progressive dilation is performed up to 14 Ch. The inner mandrel of the 10/12 Ch sheath is then used to introduce a second safety guidewire. The Clear Petra sheath is inserted and connected to a suction system via a dedicated stone-collection reservoir. All dilations, including sheath placement, are performed under continuous fluoroscopic monitoring. Once the stone is visualized, lithotripsy is performed using a 550 µm Holmium laser fiber. As fragmentation proceeds, stone fragments are aspirated through the Clear Petra system. Upon completion of lithotripsy, the sheath is removed, and an 8 Fr nephrostomy tube is positioned in the renal pelvis. The ureteral catheter is connected to the Foley catheter for continuous drainage. The Foley catheter is removed on POD1, and the nephrostomy is typically removed on POD2.
2.4. Cost Analysis
A cost analysis was conducted to compare the economic impact of RIRS and mini-PCNL from the hospital’s perspective. The analysis included both direct and indirect costs associated with each procedure, following standard micro-costing methodology [11]. Direct costs encompassed all single-use disposable materials, OR occupancy time, and surgical and anesthesia personnel resources. Because the same institutional OR cost per minute was applied to both techniques, differences in OR-related costs reflect differences in operative time rather than differences in cost assumptions. The disposable instruments used for each procedure were identified through the hospital’s procurement database and priced using institutional purchase costs. The OR time costs were calculated by multiplying the average duration of each procedure by the institutional per-minute rate, which accounts for staffing, anesthesia, and overhead expenses. Indirect costs included LoS, perioperative imaging, and ancillary pre- and postoperative care. Hospitalization costs were estimated using the average daily inpatient expenditure for urological procedures in the Italian National Health Service [9]. Minor perioperative costs, such as laboratory tests, medications, and drainage management (<EUR 200 per case), were included in the total cost per procedure. However, these costs were excluded from the adjusted cost per treated and stone-free patient, as they were considered fixed and similar across procedures. They would proportionally influence all repeated interventions without changing the relative cost differences between techniques. Imaging costs for preoperative and postoperative non-contrast CT scans were covered and calculated using institutional tariffs, with an estimated cost of approximately EUR 175 per scan, resulting in a total imaging cost of EUR 350 per patient for pre- and postoperative evaluation. The total cost per patient was determined by summing direct and indirect costs. For patients requiring multiple interventions to become SF, the total cost was adjusted proportionally to the average number of procedures per patient. All costs were calculated in euros (€) and based on 2023 institutional prices. Costs related to sterilization and reprocessing of reusable instruments were not itemized separately; they are incorporated into institutional operating room overhead and applied uniformly across procedures. A detailed breakdown of unit costs and cost assumptions is provided in Supplementary Table S1.
2.5. Statistical Analysis
Statistical analyses were conducted using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were compared between groups with either the independent Student’s t-test or the Mann–Whitney U test, depending on the data distribution. Categorical variables were analyzed using the chi-square test or Fisher’s exact test as appropriate. Results are presented as mean ± standard deviation (SD) for continuous variables and as absolute numbers with percentages for categorical data. A two-sided p-value < 0.05 was deemed statistically significant. To adjust for baseline differences in stone size, a multivariable logistic regression was performed, with final stone-free status as the outcome and treatment modality and stone size as covariates.
3. Results
3.1. Baseline Characteristics and Postoperative Outcomes
A total of 119 patients were included in the study: 62 who underwent RIRS (Group A) and 57 who underwent mini-PCNL (Group B). The mean age was 62.5 years in Group A and 63.2 years in Group B (p = 0.132). The proportion of female patients was comparable between the groups (45% vs. 47% in groups A and B, respectively, p = 0.111). The mean BMI was 22.6 kg/m^2^ (SD 3.56) for Group A and 23.1 kg/m^2^ (SD 4.29) for Group B (p = 0.098).
The prevalence of major comorbidities was comparable between groups. In Group A, hypertension was present in 37.1% of patients, compared with 38.6% in Group B (p = 0.76). Diabetes mellitus was reported in 16.1% of patients undergoing RIRS and in 15.8% of those treated with mini-PCNL (p = 0.84).
Preoperative Hb levels averaged 13.1 g/dL (SD 0.93) in group A and 12.6 g/dL (SD 0.99) in group B (p = 0.144). Preoperative serum creatinine was 1.14 mg/dL (SD 0.34) in Group A and 1.16 mg/dL (SD 0.22) in Group B (p = 0.112). The mean preoperative WBC count was 7.2 × 10^3^/µL (SD 0.48) in Group A and 7.4 × 10^3^/µL (SD 0.83) in Group B.
In Group A, 59.7% of patients were classified as ASA II, 33.9% as ASA III, and 6.5% as ASA IV. Similarly, in Group B, ASA II, III, and IV patients accounted for 61.4%, 33.3%, and 5.3% of cases, respectively. The mean stone Dmax was 21.9 mm (3.94) in group A and 24.4 mm (SD 4.61) in group B (p = 0.003). The mean stone density was 1031 HU (SD 217.3) and 1058 HU (SD 197.7) in Groups A and B, respectively (p = 0.322).
The presence of multiple adjacent stones (clustered KS located within the same calyceal system or renal segment) was observed in 8.1% of patients in Group A and 4.0% in Group B. In Group A, KS were located in the left kidney in 46.8% of cases and in the right kidney in 53.3%, whereas in Group B, left-sided KS accounted for 56.1% and right-sided stones for 43.9% of cases (all p > 0.05).
Similarly, the anatomical distribution of stones within the renal collecting system was balanced between groups. In Group A, KS were located in the renal pelvis or PUJ in 9.7%, in the upper calyx in 30.6%, in the middle calyx in 25.8%, and in the lower calyx in 33.9%. In Group B, the corresponding proportions were 10.5%, 28.1%, 29.8%, and 31.6%, respectively, with no statistically significant differences across locations (all p > 0.05) (Table 1).
3.2. Postoperative Outcomes
Mean operative time was significantly shorter in the RIRS group compared with the mini-PCNL group (87 ± 12.97 vs. 113 ± 15.25 min; p < 0.001). Conversely, the length of hospital stay was significantly longer after mini-PCNL (2.24 ± 0.46 vs. 1.22 ± 0.26 days; p = 0.008). At 24 h postoperatively, HB levels were significantly lower in Group B (10.7 ± 1.53 g/dL) compared to Group A (12.2 ± 0.95 g/dL; p = 0.032). No significant differences were observed in postoperative serum creatinine (1.14 ± 0.28 vs. 1.20 ± 0.37 mg/dL; p = 0.232) or WBC count (13.1 ± 3.42 vs. 13.4 ± 2.67 × 10^3^/µL; p = 0.187). The mean number of procedures per patient was significantly higher in Group A (1.68 ± 0.52) than in Group B (1.35 ± 0.27; p < 0.001). Postoperative complications were comparable between groups and were predominantly low-grade according to the Clavien–Dindo classification. In Group A, 16 patients experienced Clavien–Dindo grade I complications, mainly transient postoperative fever or mild pain managed conservatively. One patient developed a grade II complication (febrile UTI) requiring intravenous antibiotic therapy. One grade IIIa complication occurred due to postoperative bleeding, which was successfully managed with selective angioembolization. In the mini-PCNL group, 17 grade I complications were recorded, primarily consisting of self-limiting fever or minor postoperative discomfort. Two patients experienced grade II and required blood transfusions. One patient developed a grade IIIb complication related to significant postoperative hemorrhage, which required surgical exploration for hematoma evacuation and hemostasis and was successfully managed. No patients in either group required admission to the intensive care unit. There were no procedure-related mortalities. Stone-free outcomes differed significantly between the two techniques. After the first procedure, the CIRF-SFR was 43.55% in Group A and 70.17% in Group B (p < 0.0001). After completion of treatment, the final CIRF-SFR was 88.71% for RIRS and 94.74% for mini-PCNL (p = 0.043). The absolute SFR remained significantly higher in the mini-PCNL group (82.45% vs. 74.2%; p = 0.035) (Table 2).
3.3. Multivariable Analysis
Given the significant baseline difference in stone size between groups, a multivariable logistic regression analysis was performed to evaluate factors independently associated with final stone-free status. The model included treatment modality (RIRS vs. mini-PCNL), stone size (Dmax), stone density, and stone location (lower vs. non-lower pole). In multivariable analysis, treatment modality was not independently associated with final stone-free status (OR = 2.35, 95% CI = 0.47–11.69; p = 0.296). Stone size was also not independently associated with stone-free outcome (OR 1.01 per mm increase, 95% CI 0.84–1.21; p = 0.933). In contrast, higher stone density was independently associated with a lower likelihood of achieving stone-free status (OR 0.53 per 100 HU increase, 95% CI 0.35–0.79; p = 0.002). Stone location (lower vs. non-lower pole) was not independently associated with stone-free status (adjusted OR 0.77, 95% CI 0.17–3.42; p = 0.730). Table 3 summarizes these findings.
3.4. Cost Analysis
3.4.1. Direct Costs
Disposable materials accounted for the largest share of costs in both groups. Based on the consumables listed in Table 4, the total cost of disposable materials for a standard procedure was EUR 1097 for RIRS and EUR 806.42 for mini-PCNL (p = 0.004).
Mini-PCNL had a longer OT (113 min) compared with RIRS (87 min). Using an average cost of EUR 3.9 per operative minute, the estimated OR-related expense was EUR 340 for RIRS and EUR 440 for mini-PCNL (p = 0.012). Both procedures required similar preoperative and postoperative imaging, consisting of two non-contrast CT scans per patient, with a total imaging cost of approximately EUR 350.
3.4.2. Indirect Costs
Hospitalization accounted for an additional portion of total expenses. The mean LoS was 1.22 days for RIRS and 2.24 days for mini-PCNL. Based on an estimated inpatient cost of 334 EUR/day, there was an average hospitalization cost of approximately EUR 410 for RIRS and EUR 740 for mini-PCNL (p = 0.0001). Other pre- and postoperative costs, including laboratory tests, consultations, and drainage management, were considered minor and estimated at less than EUR 200 per patient. These expenses were not included in the adjusted cost calculations. When these expenditures were added, the total cost per procedure was EUR 2197 for RIRS and EUR 2336 for mini-PCNL (p = 0.138). Figure 3 displays the direct and indirect costs per procedure.
3.4.3. Re-Intervention Costs
The average number of procedures per patient was 1.68 for RIRS and 1.35 for mini-PCNL. The total cost per treated patient, after adjusting for the number of procedures, was approximately EUR 3689 for RIRS and EUR 3150 for mini-PCNL (p = 0.009). When total costs were adjusted for the final SFR, the estimated cost per SF patient was EUR 4159 for RIRS and EUR 3331 for mini-PCNL (p = 0.007). When accounting for absolute SFR, the cost per stone-free patient increased to EUR 4971 for RIRS and EUR 3825 for mini-PCNL. The cost analysis summary is presented in Table 5.
4. Discussion
The current EAU guidelines describe PCNL as the procedure of choice for KS ≥ 20 mm, and it is still recommended for stones with a Dmax ≥ 10 mm [8,12]. However, recent technological advances in endoscopy and the development of miniaturized PCNL systems have made both procedures safer and more effective [13,14,15,16]. Consequently, the choice between RIRS and mini-PCNL remains controversial for KS between 10 and 20 mm, where outcomes are comparable but differ in invasiveness and costs [17,18]. Hence, we aimed to compare these two procedures with respect to perioperative outcomes and other clinical manifestations, while also considering their direct and indirect costs. Consistent with the previous literature, our results showed that mini-PCNL achieved a higher SFR than RIRS. The SFR is a critical parameter in endourology, as residual fragments increase the risk of recurrence and the need for retreatment [17,18]. In the present study, SFR was primarily defined as ≤4 mm, a threshold widely used in the endourological literature. However, this approach may overestimate stone-free rates relative to stricter definitions requiring the complete absence of residual fragments, and spontaneous passage of small residual fragments, particularly after RIRS, may not be fully captured at the 30-day follow-up; this should be considered when interpreting and comparing outcomes across studies. Because stone size differed significantly between treatment groups, an adjusted analysis was performed to address the potential impact of baseline stone characteristics on stone-free outcomes. Multivariable logistic regression showed treatment modality was not independently associated with stone-free status after adjustment, cautioning against overinterpreting the higher unadjusted stone-free rate with mini-PCNL. Stone size was not an independent predictor, implying baseline differences alone did not explain success. Stone density, however, was a predictor, with higher density linked to lower clearance. Stone location, modeled as lower versus non-lower pole, was not independently associated. These findings emphasize that crude stone-free rate comparisons may be influenced by stone characteristics and highlight the importance of adjusted analyses in retrospective studies. While mini-PCNL had higher unadjusted rates and cost-efficiency due to fewer retreatments, the adjusted analysis indicates that treatment success depends on multiple factors, not just the procedure type. De et al. [19] reported that standard PCNL achieved higher SFRs than RIRS; however, it was associated with greater blood loss and longer hospitalization. In contrast, Cabrera et al. showed that mini-PCNL provided an optimal balance between efficacy and invasiveness in stones 10–20 mm [16]. Jiang et al. [15], however, did not observe significant differences in SFR between micro-PCNL and RIRS, whereas stone size, location, and anatomy were associated with treatment success. In this study, as expected, OT and LoS were longer for mini-PCNL, reflecting the greater invasiveness of the percutaneous approach. However, complication rates were comparable between the two techniques, with most events classified as Clavien–Dindo grade I–II. The rates of postoperative fever and urosepsis in both groups were comparable to those reported in the literature [20,21,22,23,24,25,26]. In this study, one patient in group A developed postoperative bleeding that was successfully treated with selective angioembolization. Another patient in the mini-PCNL group experienced a significant postoperative hemorrhage that required exploratory laparoscopy for the evacuation of the hematoma and hemostasis. Both events have been described as possible bleeding complications following endourological procedures [20,27,28]. In addition to clinical outcomes, understanding the economic impact of endourological procedures has become increasingly important. The growing adoption of minimally invasive techniques, single-use devices, and expensive disposables necessitates precise cost assessment using micro-costing methods, which account for each resource individually rather than relying on aggregate reimbursement rates [29,30]. In this study, disposable instruments represented the principal cost driver, particularly in RIRS, where single-use ureteroscopes increased per-procedure expenditure. Previous cost analyses suggest that consumables account for approximately 40–60% of the total cost of flexible ureteroscopy, depending on volume and reprocessing practices [31,32,33,34]. In high-volume centers, the per-case cost of reusable flexible ureteroscopes ranges from USD 1212 to USD 1743 [33]. In contrast, the main costs in PCNL are driven by OT and LoS [35,36]. Leow et al. reported that longer procedures and extended admissions were associated with higher total expenditure [36]. In our analysis, the single-procedure cost was EUR 2197 for RIRS and EUR 2336 for mini-PCNL. When adjusted for the average number of procedures per patient, the total cost per treated patient increased to EUR 3689 for RIRS and EUR 3154 for mini-PCNL. Further adjustment for the final SFR yielded a cost per SF patient of EUR 4159 for RIRS and EUR 3331 for mini-PCNL. While mini-PCNL entails more complex surgery and a longer LoS, its higher per-session success rate offsets these costs, resulting in better overall cost-effectiveness. Each additional RIRS procedure increases expenses for anesthesia, imaging, and staff, which accounts for the higher total cost per successfully treated patient. Although the single-procedure cost of mini-PCNL was higher than that of RIRS, the overall cost-efficiency advantage of mini-PCNL was driven by a higher single-session stone-free rate and a lower retreatment rate. Therefore, the economic benefit observed in the present study reflects treatment success per session rather than lower procedural costs. These results align with studies by Cabrera et al. and Kumar et al. [16,17], who found that PCNL has higher single-session success rates and lower retreatment rates than RIRS, both of which significantly affect total procedure costs and resource use. However, economic trends and reimbursements vary across healthcare systems. In the United States, PCNL is typically more expensive than RIRS [37,38]. In European public healthcare systems, fixed personnel costs and high disposable-use rates make RIRS comparatively costly, particularly when single-use ureteroscopes are used. Under the Italian National Health Service, reimbursement is based on DRG, which assigns higher tariffs to PCNL than to RIRS [10]; however, these tariffs do not accurately reflect real costs. The micro-costing approach that we utilized seems to provide a more precise estimate of actual hospital expenditure, highlighting that mini-PCNL achieves superior cost-efficiency despite a longer procedure and LoS. This cost analysis is based on institutional prices and assumptions that might differ across healthcare systems. The relative cost-effectiveness of RIRS and mini-PCNL could change in settings where reusable flexible ureteroscopes are used, where OR minute costs vary significantly, or where length-of-stay costs are lower. However, because the primary cost benefit of mini-PCNL in our study was a lower retreatment rate rather than lower per-procedure costs, the overall conclusions are likely to remain valid across plausible cost scenarios. Recent studies have emphasized that cost-efficiency should be considered alongside clinical efficacy in selecting the optimal treatment modality. The PUrE trial demonstrated that mini-PCNL achieved higher single-session clearance and marginally superior cost-effectiveness for lower-pole stones within the British National Health Service [39]. Future studies should focus on validating these results in larger, prospective, multicenter cohorts to reduce selection bias and to account for regional differences in costs and clinical practices. Using standardized micro-costing methods across different institutions would improve comparability and establish cost benchmarks for endourological procedures. Including patient-reported outcomes, quality-of-life data, and indirect societal costs would provide a more comprehensive view of true cost-effectiveness. Additional research should investigate how innovations such as digital and single-use ureteroscopes, miniaturized PCNL systems, and AI-assisted surgical planning impact both clinical outcomes and economic sustainability.
5. Limitations
This study has several limitations worth noting. Its retrospective nature may have introduced selection bias, particularly because mini-PCNL was introduced only after April 2022, whereas RIRS procedures occurred throughout the study period. As a result, the choice of procedure was influenced more by the availability of the PCNL program and institutional logistics than by random assignment. Mini-PCNL was introduced during the study period, and therefore, a time-related selection bias cannot be completely excluded, as procedure allocation was influenced by equipment and personnel availability. However, all procedures were performed by surgeons with extensive prior experience in PCNL (>150 cases for each surgeon), making a clinically relevant operator learning-curve effect unlikely. Although the baseline characteristics appeared similar, unmeasured factors such as stone complexity or anatomical differences could have affected the outcomes. The small sample size and single tertiary center setting may also limit the generalizability of these findings. The cost analysis was conducted from the hospital’s perspective and did not account for indirect societal costs, such as productivity losses or postoperative recovery time. Furthermore, patient-centered outcomes, including postoperative pain, time to return to normal activities, and quality-of-life measures, were not systematically collected and could not be analyzed in the present study. This represents an important limitation, particularly in the context of cost-effectiveness evaluations, as indirect costs and patient-reported outcomes may substantially influence the overall value of different treatment strategies. Additionally, long-term costs such as stone recurrence or outpatient management were not examined. Finally, variations in device prices and inpatient expenses across different healthcare systems could influence cost comparisons.
6. Conclusions
In summary, both mini-PCNL and RIRS are safe and effective options for treating KS ≥ 15 mm. Mini-PCNL tends to have higher single-session stone-free rates but involves longer OT and longer LoS. However, it is more cost-effective per patient SF when retreatment rates are considered. These results emphasize the need to integrate clinical and economic assessments when selecting the optimal treatment for individual patients. Further prospective, multicenter randomized trials that include patient-reported outcomes and long-term cost analysis are necessary to validate these findings and optimize procedural guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Stamatelou K.K. Francis M.E. Jones C.A. Nyberg L.M. Curhan G.C. Time trends in reported prevalence of kidney stones in the United States: 1976–1994 Kidney Int.2003631817182310.1046/j.1523-1755.2003.00917.x 12675858 · doi ↗ · pubmed ↗
- 2Izzo F. Langella A. Germinario C. Grifa C. Varricchio E. Di Meo M.C. Salzano L. Lotrecchiano G. Mercurio M. Morpho-Constitutional Classification of Urinary Stones as Prospective Approach for the Management of Human Pathological Biomineralization: New Insights from Southern Italy Minerals 202212142110.3390/min 12111421 · doi ↗
- 3Iossa A. Pastore A.L. Coluzzi I. Valenzi F.M. De Angelis F. Bellini D. Lelli G. Cavallaro G. Bariatric surgery does not affect kidney stone disease Sci. Rep.2024143019310.1038/s 41598-024-78771-y 39632988 PMC 11618519 · doi ↗ · pubmed ↗
- 4Hesse A. Brändle E. Wilbert D. Köhrmann K.U. Alken P. Study on the prevalence and incidence of urolithiasis in Germany comparing the years 1979 vs. 2000 Eur. Urol.20034470971310.1016/S 0302-2838(03)00415-914644124 · doi ↗ · pubmed ↗
- 5Sánchez-Martín F.M. Millán Rodríguez F. Esquena Fernández S. Segarra Tomás J. Rousaud Barón F. Martínez-Rodríguez R. Villavicencio Mavrich H. Incidence and prevalence of published studies about urolithiasis in Spain. A review Actas Urol. Esp.20073151152010.1016/S 0210-4806(07)73675-617711170 · doi ↗ · pubmed ↗
- 6Scales C.D.Jr. Smith A.C. Hanley J.M. Saigal C.S. Urologic Diseases in America Project Prevalence of kidney stones in the United States Eur. Urol.20126216016510.1016/j.eururo.2012.03.05222498635 PMC 3362665 · doi ↗ · pubmed ↗
- 7Shafi H. Moazzami B. Pourghasem M. Kasaeian A. An overview of treatment options for urinary stones Casp. J. Intern. Med.2016716 PMC 476111526958325 · pubmed ↗
- 8Skolarikos A. Geraghty R. Somani B. Tailly T. Jung H. Neisius A. Petřík A. Kamphuis G.M. Davis N. Bezuidenhout C. European Association of Urology Guidelines on the Diagnosis and Treatment of Urolithiasis Eur. Urol.202588647510.1016/j.eururo.2025.03.01140268592 · doi ↗ · pubmed ↗