Comparative Efficacy of Autologous Hematopoietic and Mesenchymal Stem Cell Transplantation in Patients with Systemic Sclerosis: A Systematic Review
Saltanat Bakirova, Abai Baigenzhin, Saltanat Tuganbekova, Manarbek Askarov, Elmira Chuvakova, Marlen Doskali, Ainur Doszhan

TL;DR
This paper compares two stem cell therapies for systemic sclerosis, finding that one is more effective but riskier while the other is safer but less studied.
Contribution
The study provides the first comparative systematic review of HSCT and MSCT in systemic sclerosis, highlighting their distinct clinical and safety profiles.
Findings
HSCT improves survival and pulmonary function but carries higher risks like transplant-related mortality.
MSCT shows benefits for skin and lung issues with lower toxicity but lacks long-term data.
HSCT is supported by stronger evidence, while MSCT remains investigational with preliminary results.
Abstract
Background/Objectives: Systemic sclerosis (SSc) is a rare and severe autoimmune disease with limited treatment options. Autologous hematopoietic stem cell transplantation (HSCT) and mesenchymal stem cell transplantation (MSCT) have emerged as promising therapeutic strategies, especially for patients with refractory or rapidly progressive forms of the disease. However, no comparative synthesis has yet evaluated the clinical outcomes, safety, and applicability of these two distinct stem-cell-based interventions. This systematic review aimed to perform a comparative qualitative synthesis of clinical outcomes, safety profiles, and evidence quality for HSCT and MSCT in patients with systemic sclerosis, focusing on survival, skin fibrosis, pulmonary function, and adverse events. Methods: A comprehensive search was conducted in PubMed, ScienceDirect, Cochrane Library, and Google Scholar for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
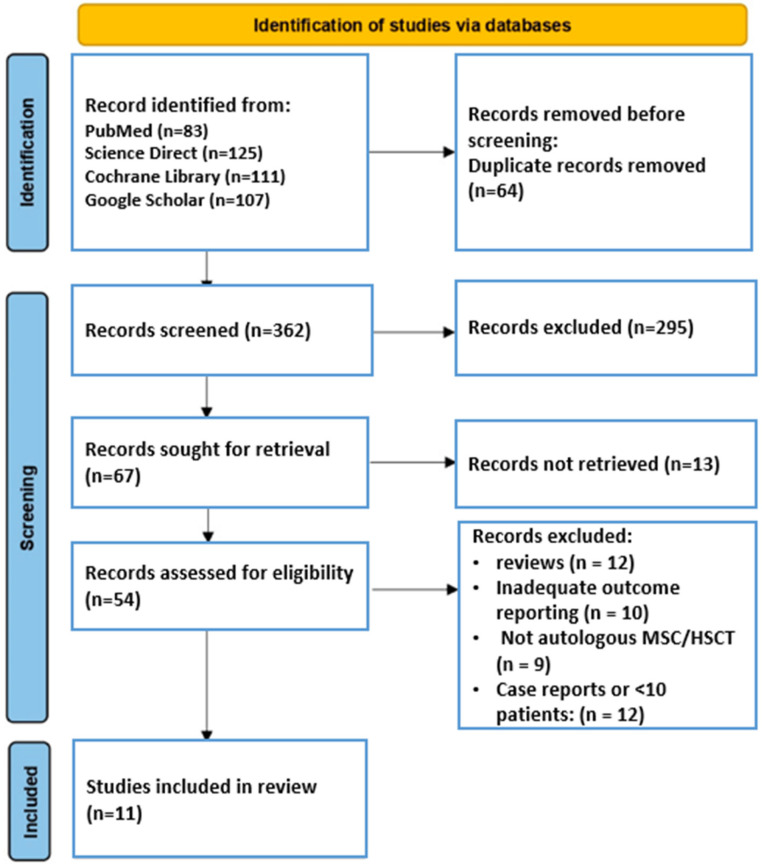 Figure 1
Figure 1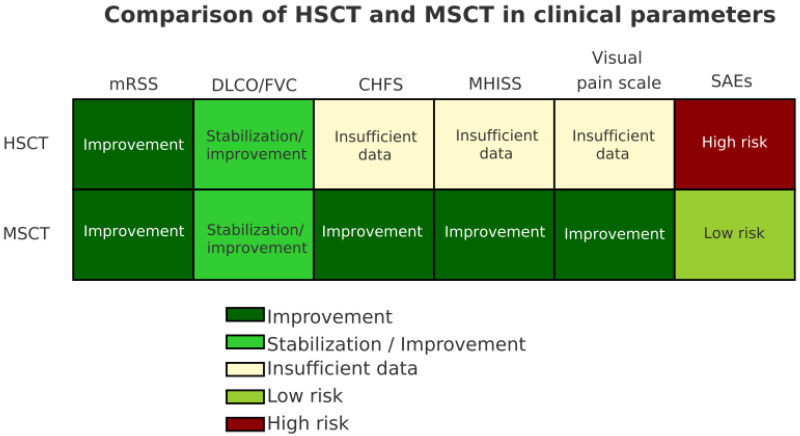 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSystemic Sclerosis and Related Diseases · Mesenchymal stem cell research · Connective Tissue Growth Factor Research
1. Introduction
Systemic sclerosis (SSc) is a chronic autoimmune rheumatic disease of unknown origin associated with environmental, hormonal and genetic factors, including epigenetic mechanisms and microRNAs [1,2,3]. The disease is characterized by damage to small vessel endothelial cells, increased vascular permeability, fibroblast activation and excessive extracellular matrix deposition [4,5]. This leads to widespread inflammation, visceral fibrosis, skin thickening and vasculopathy [6,7].
SSc is considered a rare disease, with an estimated incidence of 0.77 to 5.6 per 100,000 populations per year and a prevalence of approximately 23 per 100,000 (95% CI: 16–29) [8,9]. Mortality in this disease is significantly increased, with standardized mortality rates up to 2.72 times higher than in the general population [10].
Traditional immunosuppressive therapy (cyclophosphamide, methotrexate, mycophenolate mofetil) provides limited disease control and is often associated with significant side effects [11]. Targeted therapy, including monoclonal antibodies or tyrosine kinase inhibitors, is currently in early clinical trials, but no universal standard has been established [12,13]. Thus, the treatment of SSc remains an unsolved clinical problem.
An important step in therapy was the development of autologous hematopoietic stem cell transplantation (HSCT) in the late 1990s and early 2000s, aimed at restoring the immune system in patients with rapidly progressing, refractory disease [14,15,16]. Randomized controlled trials, including the ASSIST, ASTIS, and SCOT studies, have demonstrated the superiority of HSCT over conventional immunosuppressive therapy in selected high-risk patients, particularly those with diffuse cutaneous SSc (DCSSc) and early organ involvement [17,18,19]. However, HSCT carries significant treatment-related risks and is contraindicated in patients with advanced cardiac, pulmonary, or renal disease [20].
Recently, mesenchymal stromal cell (MSC) therapy has emerged as a potential alternative due to its immunomodulatory, anti-fibrotic, and pro-angiogenic properties [21,22,23]. MSCs can be derived from a variety of sources, including bone marrow, adipose tissue, and umbilical cord, and exert their therapeutic effects primarily through paracrine mechanisms [24]. Several early-phase studies and small clinical trials have demonstrated improvements in skin fibrosis, lung function, and quality of life after MSC [25,26,27]. Compared with HSCT, MSC is less invasive and may be more suitable for patients with contraindications to conditioning regimens [28].
Despite the growing interest in both HSCT and MSC, no head-to-head comparisons have been conducted. Furthermore, published studies are heterogeneous in design, patient selection, treatment protocols, and outcome measures [29]. To date, the relative efficacy and safety profile of these two regenerative strategies remain unclear [30]. Most existing reviews focus on one treatment modality in isolation, without systematically comparing it with other cell therapies [29,31,32,33,34].
The aim of this systematic review is to provide a comprehensive synthesis of the available evidence on hematopoietic stem cell transplantation (HSCT) and mesenchymal stromal cell therapy (MSCT) for the treatment of systemic sclerosis. Specifically, this review aims to perform a comparative qualitative synthesis of clinical outcomes, safety profiles, and strength of evidence for both treatment modalities, focusing on survival, skin fibrosis, pulmonary function, and adverse events. By systematically contrasting these outcome domains and methodological characteristics, this review seeks to clarify the current clinical role of HSCT and MSCT, identify key limitations of the existing evidence, and outline priorities for future research in systemic sclerosis.
2. Materials and Methods
The study protocol was registered in the PROSPERO International Prospective Register of Systematic Reviews of the National Institute for Health Research (ID: CRD420251114759) [35].
2.1. Search Strategy
An initial search of the PROSPERO database for registered protocols of comparable systematic reviews and meta-analyses identified no relevant registration. This systematic review was conducted and reported in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [36]. The completed PRISMA checklist (Table S1) are provided in the Supplementary Materials.
A comprehensive search was performed to identify relevant studies published between January 2015 and 1 May 2025, in order to capture current advancements in cell-based therapies for systemic sclerosis. The following databases were systematically searched: PubMed, Cochrane Library, Science Direct, and Google Scholar. Google Scholar was included as a complementary source to capture potentially relevant grey literature and recently published studies not yet indexed in major databases. Reference lists of included full-text articles and relevant reviews were also manually screened to ensure completeness of the search. All records were imported into reference management software, and duplicates were identified and removed prior to screening.
The specific search terms used included combinations of the disease (e.g., “systemic sclerosis”, “scleroderma”) and therapeutic approaches (e.g., “autologous hematopoietic stem cell transplantation”, “mesenchymal stem cells”, “auto-HSC”, “auto-MSC”). Boolean operators (AND, OR) were applied to refine the queries. The selection of search strategies was adapted to the interface of each platform. The search strategies for each database are summarized in the Supplementary Materials Table S2.
Total number of articles identified across all databases: 426. After removing duplicates and screening titles and abstracts, 54 full-text articles were assessed for eligibility. Based on the predefined inclusion and exclusion criteria (outlined in Section 2.2), only 11 studies met all inclusion criteria and were included in the final review (Figure 1).
2.2. Eligibility Criteria
This systematic review included studies based on predefined inclusion and exclusion criteria to ensure methodological consistency and relevance to the research objectives. The criteria were as follows: Studies were eligible for inclusion if they investigated either autologous hematopoietic stem cell transplantation (HSCT) or mesenchymal stromal cell therapy (MSCT) in patients with systemic sclerosis (SSc), provided that MSCT adhered to the minimum criteria established by the International Society for Cellular Therapy (ISCT). Eligible cell types included both CD34^+^-selected and unselected autologous hematopoietic stem cells, as well as cultured mesenchymal stromal cells derived from bone marrow, adipose tissue, or umbilical cord sources.
Patients had to have a confirmed diagnosis of SSc based on the ACR 1980 or ACR/EULAR 2013 classification criteria. Only adult patients (aged 18 years and older) of both sexes were included. Studies involving mixed autoimmune populations were only included if they provided a separate analysis of the SSc subgroup. The review focused on clinical studies—randomized controlled trials (RCTs), prospective or retrospective cohort studies, and open-label clinical trials. Case reports, studies with fewer than 10 participants, reviews, editorials, letters, and preclinical studies (in vitro or animal experiments) were excluded. A minimum follow-up period of 6 months’ post-transplantation or intervention was required to assess medium- to long-term clinical outcomes. Studies without clear clinical outcome reporting-such as modified Rodnan skin score (mRSS), pulmonary function tests (FVC, DLCO), survival, or patient-reported quality of life-were excluded. The complete eligibility framework is summarized in Table 1.
2.3. Selection of Studies and Data Extraction
After removal of duplicates, two independent reviewers conducted a stepwise screening of all retrieved records by evaluating titles and abstracts for relevance. Studies that met the inclusion criteria were then selected for full-text review. The final decision regarding inclusion was made after thorough examination of the full articles against the pre-defined eligibility criteria outlined in Section 2.2.
Data extraction was independently performed by two reviewers using a standardized data collection form. Any discrepancies in interpretation or data coding were resolved by consensus or, if needed, through discussion with a third senior reviewer. The following data were extracted from each eligible study: first author’s name, year of publication, country of origin, study design, type of stem cell therapy (autologous hematopoietic stem cell transplantation [HSCT] or mesenchymal stromal cell therapy [MSCT]), source and type of cells used, number and characteristics of patients (including mean age and SSc subtype), duration of follow-up, and reported clinical outcomes.
Clinical endpoints included skin involvement (mRSS), pulmonary function tests (FVC, DLCO), digital ulcers, Raynaud’s index, hand function (CHFS) and adverse events, including serious adverse events (SAEs). For MSCT studies, data on specific scoring systems such as MHISS and VAS were also collected where available. If any outcome data were missing or unclear, additional information was retrieved manually from the article text, tables, or Supplementary Files. All extracted data were reviewed for accuracy and consistency, and then compiled into structured summary tables for comparative and narrative analysis.
2.4. Risk of Bias (Quality) Assessment
The methodological quality of the included studies was evaluated using the Newcastle-Ottawa Scale (NOS), a validated tool for the assessment of non-randomized studies [37]. The NOS examines three domains: Selection of participants (maximum 4 points), Comparability of groups (maximum 2 points), and Outcome assessment (maximum 3 points), with a maximum score of 9. Higher scores indicate superior methodological quality and lower risk of bias. Two reviewers (S.T., M.A.) independently performed the assessments; disagreements were resolved by discussion and, if necessary, consultation with a third reviewer. Studies scoring ≥ 7 points were categorized as high quality, those scoring 5–6 as moderate quality, and those scoring ≤ 4 as low qualities. Detailed scoring for each study is provided in Supplementary Table S3.
We did not exclude studies based on NOS ratings, but results from those with lower quality scores were interpreted with caution. Overall, HSCT trials-particularly randomized controlled trials and large registry-based studies-consistently demonstrated high scores (8–9/9), indicating a low risk of bias, whereas most MSCT trials were retrospective, early-phase or small single-center studies, with lower scores (6–7/9), reflecting a moderate-to-high risk of bias.
Given the marked heterogeneity in study design (randomized versus observational), patient populations, disease severity, stem cell sources, conditioning regimens, follow-up duration, and outcome definitions, conducting a formal quantitative meta-analysis was not appropriate. As a result, traditional statistical approaches for evaluating publication bias, such as funnel plots or Egger’s regression, were not applicable. Nonetheless, the limited number of neutral or negative MSCT studies suggests a potential risk of selective reporting and underrepresentation of unfavorable results, which may have influenced the overall evidence profile.
To account for variability across studies, we pre-specified additional qualitative analyses. A subgroup assessment was undertaken to explore potential differences in treatment effects according to patient and disease characteristics. Furthermore, a sensitivity assessment was carried out by re-evaluating the overall conclusions after excluding smaller retrospective cohorts. These steps were intended to test the consistency and robustness of the findings in the presence of methodological heterogeneity.
3. Results
3.1. Included Study Characteristics
A total of eleven clinical studies met the inclusion criteria for this systematic review, comprising seven studies on hematopoietic stem cell transplantation (HSCT) [38,39,40,41,42,43,44] and four on mesenchymal stem cell transplantation (MSCT) [45,46,47,48]. Collectively, these studies included 504 patients diagnosed with systemic sclerosis (SSc), of whom 316 received HSCT and 188 received MSCT. All studies were published between 2015 and 2025 and met predefined quality thresholds in terms of study design, clarity of outcomes, and methodological rigor. Quality assessment using the Newcastle-Ottawa Scale indicated consistently high methodological quality among HSCT trials (8–9 points), particularly for randomized and registry-based studies, whereas MSCT studies generally scored lower (6–7 points), reflecting moderate-to-high risk of bias (Table S3).
The HSCT cohort was predominantly composed of patients with rapidly progressive diffuse cutaneous systemic sclerosis (dcSSc), most of whom were refractory to conventional immunosuppressive therapy [38,39,41,42]. In contrast, the MSCT cohort included patients with both moderate and severe forms of SSc, including those with early-stage disease or contraindications to high-intensity treatment regimens [45,46,47,48].
The duration of follow-up in HSCT studies ranged from 12 months to 15 years [38,39,40,41,42,43,44], enabling assessment of both early and long-term outcomes such as survival, disease progression, and treatment-related toxicity. MSCT studies, while more recent, offered substantial longitudinal data as well, with follow-up periods spanning 12 months to 10 years [45,46,47,48]. This allowed meaningful evaluation of sustained clinical benefits, organ-specific responses, and overall safety.
Patients in HSCT trials were generally younger, with median or mean ages ranging from 23 to 47 years [38,39,40,41,42,43,44], reflecting stringent eligibility criteria related to the risk of transplant-related complications. In MSCT studies, patient age ranged approximately from 18 to 47 years [45,46,47,48], indicating a broader age variability compared with HSCT cohorts and reflecting less restrictive inclusion criteria. Across all studies, the majority of patients were female, consistent with the known sex distribution of systemic sclerosis.
Stem cell sources and processing techniques varied between the two treatment modalities. In HSCT studies, peripheral blood CD34^+^ stem cells were commonly used, with several trials employing positive selection of CD34^+^ cells to reduce autoreactive lymphocytes [38,41,42,44]. MSCT studies utilized mesenchymal stem cells derived from allogeneic sources such as umbilical cord or bone marrow, administered without the need for myeloablative conditioning [45,46,47,48]. Notably, MSCT protocols were associated with a more favorable toxicity profile, offering a safer therapeutic alternative for patients with significant internal organ involvement or those ineligible for HSCT.
Overall, the included studies represent a clinically significant and methodologically diverse body of evidence evaluating the use of stem cell-based therapies in systemic sclerosis. Comprehensive study characteristics and individual outcomes are summarized in Table 2.
3.2. Clinical Outcomes and Comparison of Cellular Therapy
The analysis of clinical outcomes across the eleven included studies revealed consistent improvement in key parameters of systemic sclerosis (SSc) following both autologous hematopoietic stem cell transplantation (HSCT) and mesenchymal stem cell therapy (MSCT). However, the scope and magnitude of clinical benefit varied between modalities and patient populations (Table 3).
In the HSCT group, most studies focused on patients with rapidly progressive diffuse cutaneous SSc (dcSSc), refractory to conventional immunosuppressive therapy. Across studies [38,39,40,41,42,43,44], HSCT led to significant improvements in skin fibrosis, lung function, and survival. For instance, in the landmark ASTIS trial by Sullivan et al. [38], event-free survival (EFS) was significantly higher in the HSCT arm (79% vs. 50%), with a corresponding improvement in overall survival (OS: 86% vs. 51%) over 54–72 months. Similarly, the study by Henes et al. [39] demonstrated a 2-year progression-free survival of 81.8% and OS of 90% in a real-world multicenter setting. Other studies, such as those by Georges et al. [41] and Blank et al. [43], confirmed the long-term durability of the response, with 5- to 15-year survival exceeding 85%.
HSCT also yielded functional improvements. In the Brazilian study by Costa Pereira et al. [44], significant enhancement in range of motion, CHFS, DASH scores, and six-minute walk test was observed, along with a notable decrease in mRSS (mean reduction of 8.3 points, p < 0.01). However, treatment-related mortality (TRM) varied from 0% to 10% depending on conditioning regimens and patient comorbidity, particularly in those with cardiac or renal involvement [39,41,42].
MSCT studies involved more heterogeneous populations, including moderate-to-severe SSc patients and those ineligible for HSCT. Alip et al. [45] reported a significant decrease in mRSS over five years and stabilization of pulmonary arterial hypertension (PAH), with no recorded adverse events. Yuan et al. [46] demonstrated a 10-year OS benefit in the MSC group (89.4% vs. 73.4%, p = 0.002) within a propensity score–matched observational cohort, with the most pronounced effects seen in female patients and those with PAH and ILD. The combination therapy trial by Zhang et al. [47] showed a reduction in mRSS (from 20.1 to 13.8), improved CT features, and downregulation of profibrotic cytokines (TGF-β, VEGF), while the phase 1/2 study by Farge et al. [48] highlighted stabilization of lung function and a ≥25% mRSS reduction in 75% of patients.
Notably, the safety profile of MSCT was favorable across all studies [45,46,47,48], with no treatment-related deaths or severe immune complications reported. By contrast, HSCT was associated with serious adverse events in a subset of patients, particularly those with high-risk profiles, underscoring the importance of careful patient selection.
A comparative synthesis of the clinical data is presented in Table 4. Hematopoietic stem cell transplantation (HSCT) demonstrates consistently strong evidence across multiple outcomes, particularly in terms of long-term survival and disease modification. Six out of seven studies reported improved survival, with follow-up periods extending up to 15 years. Significant reductions in skin fibrosis (mRSS) and stabilization or improvement in pulmonary function (DLCO/FVC) were also consistently observed.
Secondary functional and patient-reported outcomes were reported only in a limited subset of studies and were assessed using heterogeneous instruments. Improvements in functional status and quality of life following HSCT were described by Sullivan et al. [38] and Costa Pereira et al. [44], including reductions in HAQ-DI, improvements in hand function (CHFS), range of motion, and patient-reported quality-of-life measures (SF-36, DASH). Among MSCT studies, Alip et al. [45] reported reductions in HAQ-DI, finger ulcer burden, and improved hand function, while Zhang et al. [47] described improvement in Raynaud’s index; however, these outcomes were inconsistently reported and were not primary endpoints in most studies.
In addition to the primary outcome synthesis, we performed a narrative subgroup assessment. Evidence across HSCT studies suggests that the greatest benefits are observed in younger patients with early diffuse cutaneous systemic sclerosis and preserved cardiopulmonary function [38,39,41,43]. Conversely, MSCT trials indicate potential effectiveness in women, younger individuals, and in patients with pulmonary arterial hypertension or interstitial lung disease [46]. Narrative sensitivity analysis demonstrated that excluding smaller retrospective cohorts (Dong, 2022 [40], Zhang, 2017 [47]) did not alter the overall direction of results, supporting the robustness of the main findings despite methodological heterogeneity.
To address the heterogeneity of outcome reporting across studies, we standardized the key clinical endpoints (mRSS, FVC, DLCO, survival, functional outcomes, and safety) and summarized them in Table 5. This comparative overview highlights both the variability in methodology and the consistency of trends: HSCT studies demonstrated stronger evidence for long-term survival [38,39,40,41,42,43,44], whereas MSCT studies reported more favorable safety and functional outcomes [45,46,47,48].
Mesenchymal stem cell therapy (MSCT), while supported by fewer and more heterogeneous studies, showed meaningful improvements in mRSS and pulmonary function in the majority of cases. Moreover, MSCT studies more frequently reported patient-centered outcomes, such as hand function scores and pain assessment scales, reflecting their utility in improving quality of life.
From a safety standpoint, MSCT had a considerably more favorable profile, with no reports of treatment-related mortality. In contrast, HSCT was associated with substantial early risk, including transplant-related mortality (TRM) of up to 10%, particularly in older patients or those with organ involvement.
Table 6 summarizes the methodological and structural differences between HSCT and MSCT trials. While HSCT benefits from established international guideline support and a robust base of randomized controlled trials and registries, MSCT is still emerging, with smaller-scale studies and less standardized protocols. Nonetheless, MSCT remains a promising therapeutic alternative, particularly for patient’s ineligible for HSCT due to comorbidities or disease severity.
To facilitate cross-study comparison, we generated a heatmap summarizing the relative strength of evidence for HSCT and MSCT across key clinical domains (Figure 2). Outcomes were graded according to standardized thresholds: ≥25% reduction in mRSS for skin fibrosis, ≥10% improvement in FVC or DLCO for pulmonary outcomes, and higher survival rates at 5–10 years. Adverse events and research quality were also scored. Darker shading indicates more consistent and clinically significant benefit across studies, whereas lighter shading reflects heterogeneity or weaker evidence).
4. Discussion
For patients with systemic sclerosis, particularly the diffuse cutaneous form, stem cell-based therapies provide promising alternatives to conventional immunosuppression. This review synthesized evidence from 11 clinical studies published between 2015 and 2025 [38,39,40,41,42,43,44,45,46,47,48], including 7 on hematopoietic stem cell transplantation (HSCT) and 4 on mesenchymal stem cell therapy, encompassing 504 patients.
HSCT studies [38,39,40,41,42,43,44] consistently demonstrated improvements in overall survival (OS), event-free survival (EFS), and skin fibrosis reduction, particularly in younger patients with severe, progressive disease. Randomized multicenter trials such as ASSIST [38] and ASTIS [39] provide the most robust data, further supported by registry-based studies [42,43]. However, HSCT carries substantial risks, including transplant-related mortality (TRM), infectious complications, and cardiovascular events [41,44].
Studies evaluating MSCT [45,46,47,48] reported favorable safety profiles, with no treatment-related mortality and generally reported improvements in skin involvement, pulmonary function (FVC, DLCO), and selected quality-of-life measures. In addition, longer follow-up in two observational cohorts [45,46] suggested disease stabilization and a potential association with reduced mortality, particularly among patients with pulmonary arterial hypertension or interstitial lung disease. However, these findings should be interpreted with caution, as MSCT studies were predominantly small, single-center, and non-randomized, resulting in lower methodological rigor and increased susceptibility to bias when compared with HSCT trials.
This difference in evidence quality was reflected in the formal risk-of-bias assessment. HSCT studies—especially randomized trials and national registry analyses-achieved high Newcastle-Ottawa Scale (NOS) scores (8–9/9), whereas most MSCT studies scored 6–7/9, indicating moderate-to-high risk of bias. Narrative subgroup synthesis suggested that HSCT appears to yield the greatest benefit in younger patients with early diffuse disease and preserved cardiopulmonary function, whereas MSCT may be associated with clinical improvement in selected subgroups, including women, younger patients, and those with cardiopulmonary involvement. Importantly, narrative sensitivity analyses demonstrated that exclusion of smaller retrospective cohorts did not materially change the overall direction of findings, supporting the internal consistency of the qualitative synthesis despite substantial heterogeneity. It must be emphasized that no head-to-head randomized trials directly comparing HSCT and MSCT have been conducted to date. Marked heterogeneity in study design, patient populations, baseline disease severity, outcome definitions, and duration of follow-up precluded formal meta-analytic pooling and limits direct quantitative comparison. Furthermore, the limited number of neutral or negative MSCT reports raises the possibility of publication bias, which may contribute to overestimation of treatment effects. These issues highlight the urgent need for standardized outcome definitions and harmonized reporting frameworks to enhance comparability across future studies.
Beyond whole-cell therapies, emerging research has explored alternative or adjunctive approaches, including mesenchymal stem cell-derived extracellular vesicles and exosomes [49,50,51], which may preserve immunomodulatory and antifibrotic properties while potentially reducing treatment-related risks [52,53,54,55]. In addition, combined or sequential strategies integrating cell-based therapies with immunosuppression have been proposed as potential means to improve durability of response and mitigate relapse [56,57,58,59], although clinical evidence in systemic sclerosis remains preliminary.
Taken together, the available evidence supports HSCT as the most evidence-based stem cell therapy for carefully selected younger patients with high disease activity and preserved organ function, while MSCT appears to represent a safer, investigational option for broader or more fragile patient populations [60,61,62]. Future randomized trials, prospective comparative studies, and international registries are essential to clarify relative efficacy, refine patient selection, and translate experimental promise into reliable clinical benefit.
Limitations
This review has several limitations. First, substantial heterogeneity in study design, patient characteristics, stem cell sources, conditioning regimens, and outcome definitions precluded a formal meta-analysis and limited the ability to generate pooled effect estimates. Second, although most included studies met minimum quality thresholds, many-particularly those evaluating MSCT-were non-randomized, retrospective, and limited by small sample sizes, increasing the risk of bias and residual confounding. Third, key outcomes such as mRSS, DLCO, FVC, and safety parameters were inconsistently reported, and long-term follow-up was available only in selected cohorts, potentially underestimating late adverse effects or disease relapse. Finally, publication bias cannot be excluded, as negative or neutral studies may be underrepresented, and non-English or unpublished data might have been missed. These limitations emphasize the need for larger, high-quality, and standardized clinical trials to strengthen the evidence base for both HSCT and MSCT in systemic sclerosis.
5. Conclusions
Stem cell-based therapies represent an important and evolving treatment strategy for systemic sclerosis. This systematic review demonstrates that autologous hematopoietic stem cell transplantation is supported by high-quality randomized trials and long-term registry data, showing consistent benefits in survival and disease modification in selected patients with severe diffuse cutaneous disease. However, these benefits are counterbalanced by a substantial risk of treatment-related toxicity, underscoring the importance of stringent patient selection and specialized center expertise.
Mesenchymal stem cell transplantation, while supported primarily by non-randomized and observational studies, appears to be associated with improvements in skin fibrosis, pulmonary involvement, and patient-reported outcomes with a favorable safety profile. Current evidence for MSCT should be interpreted as preliminary and hypothesis-generating, as limitations in study design, sample size, and outcome standardization preclude definitive conclusions regarding long-term efficacy or survival benefit.
In the absence of direct comparative trials, HSCT should be considered the most evidence-based option for patients with rapidly progressive disease and preserved organ function, whereas MSCT may represent a safer investigational alternative for patients with contraindications to intensive immunoablation. Future research should prioritize head-to-head comparative studies, standardized outcome reporting, and long-term safety surveillance to refine patient selection and optimize therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Volkmann E.R. Andréasson K. Smith V. Systemic sclerosis Lancet 202340130431810.1016/S 0140-6736(22)01692-036442487 PMC 9892343 · doi ↗ · pubmed ↗
- 2Pope J.E. Denton C.P. Johnson S.R. Fernandez-Codina A. Hudson M. Nevskaya T. State-of-the-art evidence in the treatment of systemic sclerosis Nat. Rev. Rheumatol.20231921222610.1038/s 41584-023-00909-536849541 PMC 9970138 · doi ↗ · pubmed ↗
- 3Rutka K. Garkowski A. Karaszewska K. Łebkowska U. Imaging in diagnosis of systemic sclerosis J. Clin. Med.20211024810.3390/jcm 1002024833445449 PMC 7827740 · doi ↗ · pubmed ↗
- 4Asano Y. The pathogenesis of systemic sclerosis: An understanding based on a common pathologic cascade across multiple organs and additional organ-specific pathologies J. Clin. Med.20209268710.3390/jcm 909268732825112 PMC 7565034 · doi ↗ · pubmed ↗
- 5Rosendahl A.H. Schönborn K. Krieg T. Pathophysiology of systemic sclerosis (scleroderma)Kaohsiung J. Med. Sci.20223818719510.1002/kjm 2.1250535234358 PMC 11896191 · doi ↗ · pubmed ↗
- 6Truchetet M.E. Brembilla N.C. Chizzolini C. Current concepts on the pathogenesis of systemic sclerosis Clin. Rev. Allergy Immunol.20236426228310.1007/s 12016-021-08889-834487318 PMC 10167130 · doi ↗ · pubmed ↗
- 7Lambova S.N. Kurteva E.K. Dzhambazova S.S. Vasilev G.H. Kyurkchiev D.S. Geneva-Popova M.G. Capillaroscopy and immunological profile in systemic sclerosis Life 20221249810.3390/life 1204049835454989 PMC 9024594 · doi ↗ · pubmed ↗
- 8Zhong L. Pope M. Shen Y. Hernandez-Muñoz J.J. Wu L. Prevalence and incidence of systemic sclerosis: A systematic review and meta-analysis Int. J. Rheum. Dis.2019222096210710.1111/1756-185X.1371631621157 · doi ↗ · pubmed ↗