Hemorrhagic Complications in Patients with Atrial Fibrillation Treated with Novel Oral Anticoagulants: Results from the CRAFT Study
Marek Styczkiewicz, Mateusz Wawrzeńczyk, Adam Sukiennik, Bartosz Krzowski, Cezary Maciejewski, Piotr Lodziński, Leszek Kraj, Grzegorz Opolski, Marcin Grabowski, Paweł Balsam, Michał Peller

TL;DR
This study identifies factors that increase bleeding risk in atrial fibrillation patients taking new anticoagulants and creates a tool to predict and manage this risk.
Contribution
The novel contribution is the development of the CRAFT bleeding score to predict hemorrhagic events in AF patients on DOACs.
Findings
17.4% of patients experienced bleeding episodes during a four-year follow-up.
Nine clinical factors were identified as predictors of bleeding complications.
The CRAFT bleeding score was developed to guide monitoring and minimize bleeding risks.
Abstract
Background/Objectives: Hemorrhagic complications are among the most common adverse events of anticoagulant therapy in patients with atrial fibrillation (AF). Non-vitamin K antagonist oral anticoagulants (DOACs) are known to be more effective than vitamin K antagonists (VKAs) in preventing thromboembolism. The aim was to identify clinical factors associated with hemorrhagic events in AF patients treated with DOACs and to develop a simple, clinically applicable bleeding risk score. Methods: Data were derived from the multicenter CRAFT trial (NCT02987062). We conducted a retrospective analysis of hospital records of 1435 AF patients (median age: 67 years; 44.8% female) treated with dabigatran or rivaroxaban. The main study endpoints were the occurrence of a bleeding episode, thromboembolic episode, or all-cause death during a mean four-year follow-up (1531 [1062–2140] days). Results: The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
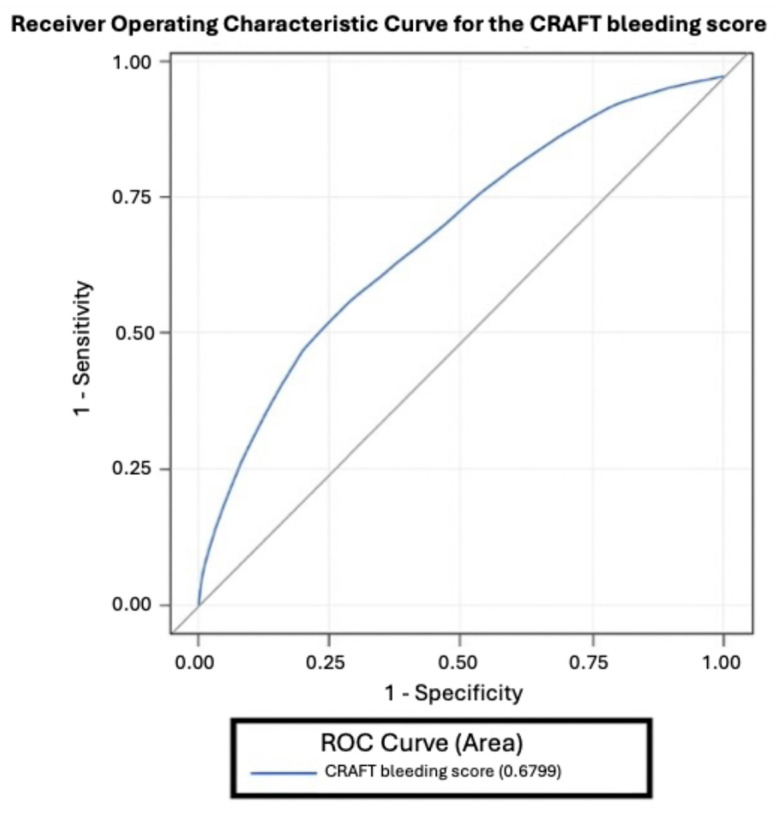 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Venous Thromboembolism Diagnosis and Management · Intracerebral and Subarachnoid Hemorrhage Research
1. Introduction
Anticoagulant therapy is essential for patients with atrial fibrillation (AF), as it prevents thrombotic complications, most importantly ischemic stroke. Except for patients at very low thrombotic risk, it is widely used [1,2,3]. However, it carries well-recognized side effects such as hemorrhagic complications.
In recent years, the management of atrial fibrillation has evolved substantially with the introduction of non-vitamin K antagonist oral anticoagulants (DOACs), including dabigatran, rivaroxaban, apixaban, and edoxaban. DOACs have been shown to provide several advantages over vitamin K antagonists (VKAs), both in preventing thromboembolic episodes and reducing the frequency of bleeding complications [4,5,6]. These agents provide predictable pharmacokinetics, fewer drug–food interactions, and do not require routine INR monitoring, which has significantly improved patient convenience. However, despite their favorable safety profile compared to warfarin, bleeding events remain a relevant clinical concern. Several bleeding risk scores have been proposed, such as HAS-BLED and, more recently, the DOAC score, but these were derived mainly from VKA-treated populations and may not fully capture risk factors specific to DOAC therapy [7,8]. Therefore, developing a DOAC-specific bleeding risk score based on real-world data is important to better individualize treatment and minimize complications.
The aim of this study was to evaluate factors influencing bleeding risk and to develop a reliable clinical score to assess the risk of hemorrhagic events in patients treated with DOACs.
2. Materials and Methods
2.1. Study Design
Data were obtained from the MultiCenter expeRience in AFib patients Treated with oral anticoagulation (CRAFT, NCT02987062) study. The CRAFT registry was designed as a retrospective, multicenter, observational cohort study involving two Polish hospitals (one academic tertiary-care center and one regional hospital).
The study included adult patients with AF hospitalized between 2011 and 2016 in one of two hospitals: one academic and one regional. Details have been reported elsewhere [9]. Patients diagnosed with valvular AF or not treated with OACs were not included in the study. Patients treated with apixaban were excluded from the study due to small group size, meanwhile edoxaban was not available in Poland during that period, therefore patients included in the study were treated with dabigatran or rivaroxaban. Baseline characteristics regarding demographics, medical history, type of AF, diagnostic tests results and pharmacotherapy were collected.
The primary endpoints were the occurrence of a bleeding episode, thromboembolic episode, or all-cause death during the mean follow-up of four years (1531 [1062–2140] days). Bleeding events were identified using diagnostic codes for gastrointestinal, intracranial, and other bleeding-related conditions. Ischemic events included ischemic stroke, transient ischemic attack, and peripheral thromboembolism. Due to the retrospective nature of the study, some parameters were not available for all patients.
2.2. Statistical Analysis
All statistical analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, USA). Continuous variables were tested for normality using the Shapiro–Wilk test and presented as mean ± standard deviation or median with interquartile range, depending on distribution. Categorical variables were reported as counts and percentages.
Comparisons between groups were performed using the chi-square or Fisher’s exact test for categorical variables, and Student’s t-test or Mann–Whitney U test for continuous variables, depending on distribution. Time-to-event outcomes were analyzed using Kaplan–Meier estimates and compared between groups using the log-rank test.
To identify independent predictors of hemorrhagic events, a multivariate Cox proportional hazards regression model was constructed. Variables with a p-value < 0.10 in univariate analysis were entered into the multivariate model. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated. A two-sided p-value < 0.05 was considered statistically significant.
Based on the multivariate model, a clinical scoring system was developed to stratify patients by bleeding risk. Predictors were assigned weighted point values reflecting their relative contributions. Discriminatory performance was assessed using receiver operating characteristic (ROC) curve analysis. Patients were categorized into low-, medium-, and high-risk groups.
All statistical tests were two-tailed and performed at a significance level of α = 0.05
3. Results
A total of 1435 patients were included (median age: 67 years; 44.8% female). Over a mean follow-up of 4.2 years, bleeding events occurred in 17.4%, thromboembolic events in 13.5%, and death in 23.9%.
Several factors significantly influenced the incidence of bleeding complications. Congestive heart failure and female sex reduced the risk of bleeding, while seven factors increased risk: history of major bleeding, history of cancer, COPD, CRT, rivaroxaban therapy, statin therapy, and age. Baseline characteristics and the number of patients analyzed for each parameter are shown in Table 1. Results and statistical data are presented in Table 2.
Among these, two factors had the most significant effect: a history of major bleeding, which increased the risk of hemorrhage more than threefold, and CRT, which increased the risk nearly fivefold. Conversely, congestive heart failure reduced the incidence of bleeding events by nearly half.
Based on these findings, the CRAFT bleeding score was developed to determine the risk of hemorrhagic complications. The scoring system is presented in Table 3.
The ROC curve (Figure 1) demonstrates good discriminatory ability of the score in predicting hemorrhagic episodes. Patients were stratified into three groups: Low risk (≤10 points), Medium risk (11–14 points), and High risk (≥15 points).
Table 4 shows the distribution of patients by risk group. The risk of bleeding was less than 7% in group 1, but reached 38% in group 3, underscoring the clinical utility of the score.
4. Discussion
Based on real-life registry data, we developed a practical score for predicting bleeding risk in patients receiving DOAC therapy for AF. Importantly, the CRAFT bleeding score relies solely on clinical history, without requiring additional laboratory tests, making its application simple and widely accessible.
Most parameters identified in this study were consistent with expectations. History of hemorrhage, older age, and cancer were clearly associated with increased bleeding risk [10,11]. CRT also emerged as a strong risk factor; however, heart failure appeared to reduce bleeding risk, which is somewhat counterintuitive. A plausible explanation is that patients with HF—particularly those with implanted cardiac devices—tend to receive more structured follow-up and closer home-based surveillance, which may limit exposure to uncontrolled hypertension or inappropriate medication use. Matteucci Et Al. demonstrated that telemonitoring in HF patients allows early identification of clinical deterioration and timely optimization of therapy [12]. In their cohort of 312 individuals, remote monitoring during the COVID-19 lockdown resulted in fewer emergency admissions for arrhythmic and HF events compared with the pre-pandemic period, despite an increased number of HF-related alerts. This supports the notion that systematic surveillance can stabilise clinical status and reduce the likelihood of acute changes in pharmacotherapy that might predispose to bleeding. Such close monitoring also facilitates regular reassessment of anticoagulant indication and dosing, as well as prompt detection of laboratory abnormalities that contribute to bleeding risk.
Findings from Ikebe Et Al. further highlight the importance of HF severity in shaping prognosis [13]. In a large PCI cohort, HF accompanied by elevated BNP levels was independently associated with higher rates of major bleeding, subsequent major adverse cardiac events, and all-cause mortality. Moreover, early post-procedural bleeding markedly amplified this risk. These results indicate that any potential attenuation of bleeding risk in HF patients is more likely a consequence of intensified clinical oversight than a reflection of HF biology. Only in settings where follow-up is rigorous and anticoagulation is closely supervised might HF appear to confer a relative reduction in bleeding events.
Taken together, available evidence suggests that HF itself is a marker of heightened vulnerability and increased bleeding risk. The apparently protective effect observed in our DOAC-treated cohort is therefore best interpreted as a “surveillance effect,” driven by more vigilant monitoring, cautious dose adjustment, and overall tighter long-term management in this patient population.
The development of a DOAC-specific prediction tool is crucial, as most existing scores were derived from VKA-treated cohorts [14] and may not accurately capture DOAC-related bleeding risk [7]. Compared with other scores, ours appears more effective, being derived exclusively from DOAC-treated patients.
The widely used HAS-BLED score was developed largely from warfarin-treated populations [7]. It does not consider factors such as CRT, rivaroxaban use, or sex. Moreover, one HAS-BLED component is labile INR, which is irrelevant for DOAC therapy. While HAS-BLED performs well in identifying bleeding risk among multimorbid patients with liver dysfunction or hypertension, it may underestimate risk in otherwise healthy patients undergoing rivaroxaban therapy or CRT, potentially leading to unexpected hemorrhagic events.
The CRAFT bleeding score incorporates several significant factors absent from the recently proposed DOAC score [8], notably CRT, which increased bleeding risk nearly fivefold in our study. For example, an elderly patient treated with rivaroxaban, undergoing CRT, and suffering from COPD would be classified as very high risk by the CRAFT score, while the DOAC score might not reach the same conclusion. However, it must be noted that the DOAC score was developed in more diverse cohorts treated with multiple DOACs (dabigatran, rivaroxaban, apixaban, edoxaban), which may make it more broadly applicable outside our population.
The CRAFT bleeding score stratifies patients into low-, medium-, and high-risk groups, with good correlation between score and bleeding incidence. This has several clinical benefits: it allows identification of high-risk patients, enabling treatment modification (e.g., dose reduction, switching to another DOAC) to reduce bleeding risk. It may also guide closer monitoring and preventive care, thereby reducing bleeding-related mortality. In particular, patients at high risk of bleeding may benefit from switching from rivaroxaban to another DOAC. Apixaban, for example, is associated with a lower bleeding risk compared to rivaroxaban [15,16], and may be a better option for such patients.
The CRAFT bleeding score has several potential clinical applications. It can serve as a practical tool for physicians to identify AF patients at increased risk of hemorrhagic events before initiating DOAC therapy, supporting personalized decision-making. In high-risk patients, clinicians may consider avoiding rivaroxaban, therefore selection of a DOAC with a lower bleeding profile, such as apixaban. Furthermore, the CRAFT score could be integrated into electronic health record systems and clinical decision-support software, enabling automated, real-time risk assessment during routine clinical visits. Ultimately, its implementation may improve patient safety, adherence to therapy, and long-term treatment outcomes in anticoagulated AF populations.
It is worth noting that non-anticoagulation strategies may also be considered for stroke prevention especially in growing population of patients diagnosed with wearable technologies and recordings from cardiovascular implantable electronic devices (CIEDs) [17]. Those strategies may include drugs such as folic acid, rosuvastatin, and candesartan in patients with low cardiovascular risk. Moreover treatment with GLP-1) receptor agonists may reduce risk of stroke in diabetic patients [18,19], while in CAD patients colchicine has stroke-preventative potential [20].
A major limitation of the CRAFT score is the absence of external validation. Future studies must evaluate the score prospectively in larger, multicenter cohorts that include patients treated with apixaban and edoxaban. This will allow proper assessment of the model’s discrimination and calibration and will position CRAFT directly against established tools such as HAS-BLED and the DOAC score.
Integrating this score into clinical decision-support systems has a potential to facilitate automatic risk stratification at the point of care. Moreover, combining bleeding and thromboembolic risk models could enable more personalized anticoagulation strategies.
5. Conclusions
Among the factors significantly increasing bleeding risk during DOAC therapy, the strongest predictors were history of bleeding and CRT. In patients with these risk factors, heightened vigilance and close monitoring should be implemented.
Based on data from the CRAFT registry, we developed the CRAFT bleeding score, which stratifies patients into three risk categories and may serve as a clinically useful tool to identify patients at increased risk of hemorrhagic events. It may guide treatment modification and closer follow-up for individuals at high risk, therefore improving patient safety and treatment outcomes. Future validation in prospective studies will determine its role in everyday clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kirchhof P. Benussi S. Kotecha D. Ahlsson A. Atar D. Casadei B. Castella M. Diener H.C. Heidbuchel H. Hendriks J. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS Europace 2016181609167810.1093/europace/euw 29527567465 · doi ↗ · pubmed ↗
- 2Lip G.Y. Lane D.A. Stroke prevention in atrial fibrillation: A systematic review JAMA 20153131950196210.1001/jama.2015.436925988464 · doi ↗ · pubmed ↗
- 3Hart R.G. Pearce L.A. Aguilar M.I. Meta-analysis: Antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation Ann. Intern. Med.200714685786710.7326/0003-4819-146-12-200706190-0000717577005 · doi ↗ · pubmed ↗
- 4Granger C.B. Alexander J.H. Mc Murray J.J. Lopes R.D. Hylek E.M. Hanna M. Al-Khalidi H.R. Ansell J. Atar D. Avezum A. Apixaban versus warfarin in patients with atrial fibrillation N. Engl. J. Med.201136598199210.1056/NEJ Moa 110703921870978 · doi ↗ · pubmed ↗
- 5Connolly S.J. Ezekowitz M.D. Yusuf S. Eikelboom J. Oldgren J. Parekh A. Pogue J. Reilly P.A. Themeles E. Varrone J. Dabigatran versus warfarin in patients with atrial fibrillation N. Engl. J. Med.20093611139115110.1056/NEJ Moa 090556119717844 · doi ↗ · pubmed ↗
- 6Ruff C.T. Giugliano R.P. Braunwald E. Hoffman E.B. Deenadayalu N. Ezekowitz M.D. Camm A.J. Weitz J.I. Lewis B.S. Parkhomenko A. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials Lancet 201438395596210.1016/S 0140-6736(13)62343-024315724 · doi ↗ · pubmed ↗
- 7Pisters R. Lane D.A. Nieuwlaat R. de Vos C.B. Crijns H.J. Lip G.Y. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: The Euro Heart Survey Chest 20101381093110010.1378/chest.10-013420299623 · doi ↗ · pubmed ↗
- 8Aggarwal R. Ruff C.T. Virdone S. Perreault S. Kakkar A.K. Palazzolo M.G. Dorais M. Kayani G. Singer D.E. Secemsky E. Development and Validation of the DOAC Score: A Novel Bleeding Risk Prediction Tool for Patients With Atrial Fibrillation on Direct-Acting Oral Anticoagulants Circulation 202314893694610.1161/CIRCULATIONAHA.123.06455637621213 PMC 10529708 · doi ↗ · pubmed ↗