Conduction System Pacing Improved Cardiac Functions, Myocardial Work and Functional Capacity in Heart Failure with Reduced Ejection Fraction and Right Bundle Branch Block
Anna Zsófia Tóth, László Nagy, Csaba Jenei, Arnold Péter Ráduly, Gábor Sándorfi, Krisztina Mária Szabó, Alexandra Kiss, László Tibor Nagy, Gergő István Szilágyi, Zoltán Csanádi

TL;DR
Conduction system pacing improves heart function and exercise capacity in heart failure patients with right bundle branch block.
Contribution
This study demonstrates that conduction system pacing improves cardiac mechanics and functional outcomes in HFrEF with RBBB.
Findings
CSP reduced QRS duration and improved left ventricular ejection fraction and strain.
Myocardial work index and work efficiency increased significantly after CSP.
Functional capacity improved as shown by increased 6-minute walk distance and better NYHA class.
Abstract
Background/Objectives: Conduction system pacing (CSP) is a potential alternative to biventricular pacing (BVP) in heart failure with reduced ejection fraction (HFrEF) and left bundle branch block (LBBB) or non-LBBB. Available data also suggest that unlike BVP, CSP may improve clinical outcome in patients with right bundle branch block (RBBB), although its effects on cardiac mechanics and energetics are ill-defined. Herein, we report on echocardiographic and clinical outcomes of CSP in this patient cohort. Methods: CSP either with His bundle pacing or LBB area pacing was attempted as a primary strategy in patients with RBBB, QRS duration ≥ 130 ms, LVEF < 35% and NYHA II-IV symptoms after optimized medical therapy for 6 months. Data on functional status, NT-proBNP and echocardiographic parameters were collected at baseline and 6 months after CSP. Results: CSP performed in 16 patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
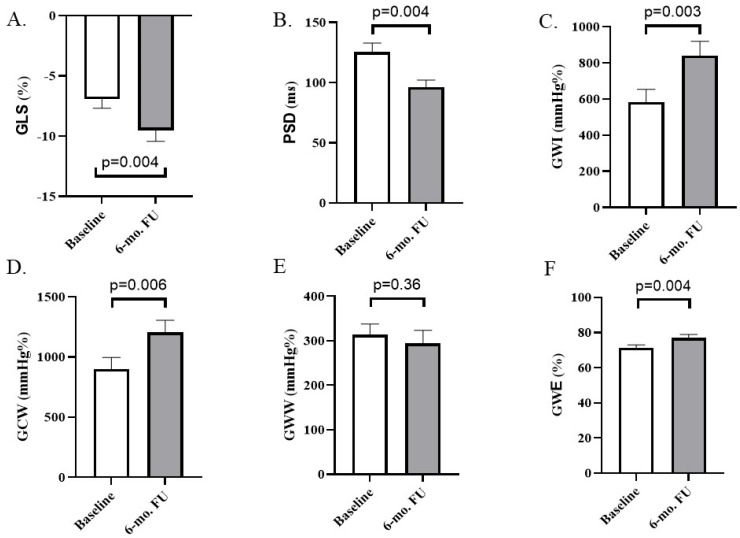 Figure 1
Figure 1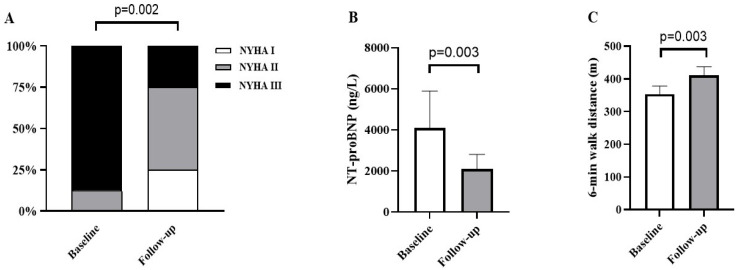 Figure 2
Figure 2- —TKP2021-EGA-18
- —Ministry of Culture and Innovation of Hungary from the National Research, Development and Innovation Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac pacing and defibrillation studies · Heart rate and cardiovascular health · Mechanical Circulatory Support Devices
1. Introduction
Cardiac resynchronization therapy (CRT) utilizing biventricular pacing (BVP) has been approved as an effective treatment for heart failure (HF) with reduced left ventricular (LV) ejection fraction (HFrEF), associated with significant intraventricular conduction delay. The most benefits after BVP can be expected in patients with a left bundle branch block (LBBB) pattern, while the improvement is less significant in the presence of a right bundle branch block (RBBB) morphology [1].
Conduction system pacing (CSP), including His bundle pacing (HBP) and left bundle branch area pacing (LBBAP), has recently emerged as an alternative to BVP to resynchronize the left ventricle (LV) in HFrEF patients with a bundle branch block (BBB) and a wide QRS complex. Unlike BVP, HBP as well as LBBAP were shown to achieve electrical resynchronization and improve clinical outcomes even in patients with RBBB and reduced LVEF [2,3]. LBBAP is a collective term for pacing strategies targeting the left bundle branch (LBB) region, including (1) direct stimulation of the main trunk of the LBB, referred to as LBB pacing (LBBP); (2) capture of the conduction system distal to the division of the main left bundle (left fascicular pacing); and (3) LV septal pacing (LVSP), capturing only the deep LV septal myocardium. In clinical practice, LBBAP has become the preferred method as opposed to HBP at many centers, considering its better long-term threshold stability and the technically less demanding implantation technique [4,5].
Reverse LV remodeling after resynchronization with BVP or with any of the CSP techniques mentioned above is assessed routinely by measuring the left ventricular ejection fraction (LVEF) using 2D echocardiography. However, recent data suggest that the evaluation of the global and regional myocardial deformation as well as myocardial work (MW) may provide a better and more comprehensive assessment of ventricular dyssynchrony and myocardial efficiency as well as further insights into the mechanism of improvement after CRT [6]. With the use of these novel and sensitive imaging techniques, the preservation of normal LV MW has been demonstrated with both HBP and LBBAP being performed for bradycardia indication in patients with a narrow QRS complex, while an improvement has been observed in those with HFrEF and LBBB [7]. However, no studies have yet investigated the effects of CSP on cardiac mechanics and energetics in HFrEF patients with RBBB.
We conducted this research to evaluate the efficacy of CSP on the LV myocardial performance, mechanical synchrony and MW in patients with advanced HF and RBBB ECG morphology.
2. Materials and Methods
2.1. Study Design and Patients’ Population
This was a single-center observational study based on a retrospective analysis of consecutive patients with CSP implantation between January 2021 and January 2024. HBP or LBBAP was attempted in patients with RBBB, QRS duration ≥ 130 ms, LVEF < 35% and NYHA class II to IVa HF symptoms despite guideline-directed medical treatment (GDMT) including beta-blockers, aldosterone antagonist, angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs)/angiotensin receptor-neprilysin inhibitors (ARNIs) and sodium-glucose co-transporter-2 (SGLT-2) inhibitors at least for 6 months. Patients with bradycardia indication for pacemaker therapy were excluded. The study protocol was approved by the ethics committee of the University of Debrecen (Registry number: BMEÜ/4388-1/2022/EKU), and the study complied with the Declaration of Helsinki.
2.2. CSP Implantation
Initially, HBP was the preferred method for CSP. Crossover to LBBAP was allowed in cases of failed HBP. However, in the last 6 patients, LBBAP became the preferred approach attempted first for CSP. HBP was performed using a Medtronic C315His sheath and SelectSecure 3830 lead (Medtronic, Minneapolis, MN, USA). His bundle (HB) region was identified by tricuspid valve angiography and then mapped with the pacing lead in unipolar fashion, recorded on an electrophysiology recording system (Schwarzer Cardiotek, Heilbronn, Germany). Once the HB potential was recorded, the lead was fixed by 4–6 clockwise rotations. The presence of HB capture, HB capture type (selective vs. non-selective HBP) and RBBB correction thresholds (detailed further in the Supplementary Materials) were assessed by decreasing the pacing output from 5V pulse amplitude and 0.4 ms pulse width as described earlier [8].
The methodology of LBBAP implantation has also been described [9]. After tricuspid valve angiography, the Medtronic C315His sheath and the SelectSecure 3830 lead were advanced 1.5–2 cm inside the right ventricle towards the apex. The target site for lead deployment was identified with unipolar pacing from the lead tip. Preferred QRS morphology was a ‘W’ pattern in V1 with discordant QRS complexes in lead II (positive or equiphasic) and III (negative or equiphasic). At this location, rapid rotation of the lead was applied, while fixation beats with RBBB morphology indicated the appropriate advancement. Rotations were then stopped, and the presence of LBB/fascicular potential, the unipolar paced QRS morphology, the myocardial current of injury and electric parameters were precisely evaluated. During LBBAP, unipolar stimulation was the preferred program setting. In case of inadequate RBBB pattern attenuation, bipolar stimulation was tested to overcome RBBB by anodal capture from the ring electrode [9].
2.3. Criteria of CSP Capture Types and Procedural Success
Selective (S-HBP) or non-selective HBP (NS-HBP) were determined based on previously published criteria. In general, in the case of S-HBP an isoelectric stimulus to QRS interval can be observed, while with NS-HBP a pseudo-delta wave following the stimulus indicates simultaneous myocardial activation in addition to the conductive tissue capture. In patients with bundle branch blocks (BBBs), both S-HBP and NS-HBP may result in partial/total BBB attenuation or the BBB may remain uncorrected (see the criterion in the Supplementary Materials) [10]. If a stable, reproducible HB capture with acceptable threshold (<3 V/0.4 ms) could not be achieved, or if the RBBB remained uncorrected, it was considered as a procedural failure.
LBBAP was confirmed when the unipolar paced QRS morphology in lead V1 demonstrated an RBBB pattern with one of the following criteria: (1) transition of the QRS morphology from either non-selective LBBP (NS-LBBP) to selective (S-LBBP) or NS-LBBP to LVSP during the unipolar threshold test by decreasing the pacing output from 5V pulse amplitude and 0.4 ms pulse width; or (2) the presence of LBB/fascicular potential with the interval of the potential to V6-R-Wave peak time (RWPT) in intrinsic rhythm equal to pacing stimulus to V6-RWPT. If none of the above criteria could be evaluated with the paced QRS complex showing Qr/QR morphology in lead V1, LVSP was confirmed. Failure of the procedure was defined as LBBAP with a high threshold, inability to penetrate the septum or failure to meet the predefined LBBAP criteria [3].
2.4. Echocardiographic Measurements
All echocardiographic measurements before and after CSP were carried out by the same cardiologist (C.J.) blinded to the clinical data of the patients to minimize any potential bias during interpretation of the echocardiographic results; however, intracardiac leads visible on echocardiographic images may be considered as a potential bias. Echocardiographic measurements including cardiac chamber quantification were performed according to the recommendations of the European Association of Cardiovascular Imaging [11]. Transthoracic echocardiographic images were recorded by using a Vivid E95 ultrasound system (GE Healthcare, Milwaukee, WI, USA), obtained for 3–5 consecutive beats for sinus rhythm, and at least 5 consecutive beats in the case of atrial fibrillation.
Left atrial diameters, LV and RV dimensions and volumes and tricuspid annulus plane excursion (TAPSE) were measured using 2D echocardiography, and LVEF was calculated by the modified biplane Simpson’s method. LV volumes were indexed on body surface area and expressed as mL/m^2^ [11]. Criteria for CSP response were defined as a ≥5% increase in the LVEF at 6 months follow-up, as used elsewhere [2,3].
Myocardial contractility and the intraventricular synchrony were further characterized by 2D speckle tracking echocardiography (2D-STE): LV global longitudinal strain (GLS) was considered as an advanced marker for the myocardial contractility, and the peak strain dispersion (PSD) implicated the LV mechanical dyssynchrony. Regional strain values were measured by 2D-STE at a frame rate of 60–100 frames/s by using images of the apical 4-, 3-, and 2-chamber views, as detailed elsewhere. GLS was calculated as an average of peak strains obtained from the 3 apical views. A bull’s-eye plot was created for peak GLS for each myocardial segment. PSD was defined as the standard deviation (SD) of the time-to-peak strain curves of different LV segments. Strain measurements were averaged from three cardiac cycles in sinus rhythm, or from 3–5 cycles in patients with atrial fibrillation [11,12].
LV MW was evaluated by the global myocardial work index (GWI), global constructive work (GCW), global wasted work (GWW) and global work efficiency (GWE), quantified by using LV pressure–strain loop (PSL) estimations paralleling non-invasive blood pressure (BP) measurements and LV GLS data. Non-invasive BP was recorded prior to the echocardiography at rest by averaging the results of three consecutive measurements; in patients with atrial fibrillation, BP average was obtained from 3–5 consecutive measurements. The area within each PSL implicated MW. The quantification of MW was carried out by automated function analysis on the software of the ultrasound system (GE Healthcare, Milwaukee, WI, USA). GWI (mmHg%) was considered as the amount of MW during systole, indicated by the area of PSLs from the mitral valve closure to mitral valve opening. GCW (mmHg%) represents the sum of positive work performed in systole (shortening) and negative work during isovolumetric relaxation (lengthening). GWW (mmHg%) was the sum of the negative work (lengthening) performed in systole and positive work (shortening) during isovolumetric relaxation. Finally, GWE was defined as the ratio of GCW to total work (GCW plus GWW), expressed as a percentage (%) [6].
2.5. Follow-Up
Patients were evaluated before the implantation and 6 months thereafter. Baseline ECG was evaluated with special care to differentiate typical and atypical RBBB patterns. Typical RBBB shows a wide S-wave in the lateral lead I and aVL, while an atypical RBBB pattern lacks an S-wave in lead I and aVL and is associated with left-axis deviation without or with PR prolongation [13]. Device interrogation, functional assessment (NYHA class evaluation and 6 min walk test), NT-proBNP level evaluation, detailed 2D echocardiography and 2D-STE were also performed. HF hospitalization and all-cause mortality data were also collected.
2.6. Statistical Analysis
GraphPad Prism 10 (GraphPad Software Inc., San Diego, CA, USA) was applied for statistical analysis. Continuous variables were depicted with the mean and SD; categorical variables were illustrated by counts and percentages. Chi-square distribution was used for evaluating the categorical variables. Paired comparisons were performed using a paired t-test if the data were normally distributed (estimated by D’Agostino and Pearson tests) and with the Wilcoxon test for nonparametric data. To account for multiple testing methods, p-values were adjusted using the Holm–Bonferroni method for the predefined outcome families.
3. Results
3.1. Patients’ Baseline Data
CSP implantation was attempted in 20 consecutive patients and concluded successfully with either HBP or LBBAP in 16, but deep septal penetration was not feasible in 4 patients. Baseline patient characteristics and comorbidities are depicted in Table 1. Briefly, male sex was overrepresented, and the underlying pathology was non-ischemic cardiomyopathy in two-thirds of the patients. The most common comorbidities were hypertension, diabetes mellitus, chronic kidney disease and atrial fibrillation.
Baseline ECG characteristics are summarized in Table 2. The mean QRS duration (QRSd) exceeded 150 ms, and only five patients had QRSd below 150 ms. The majority (12/16) of the patients had a typical RBBB pattern. Most patients also had atrioventricular (AV) conduction delay and/or a left anterior hemiblock pattern; however, none of them had advanced AV conduction disease requiring permanent cardiac pacing.
All patients were on optimized medical therapy: ACEI/ARBs and ARNI were used in 19% and 81%, respectively; beta-blockers in 100%; mineralocorticoid receptor antagonists in 93%; and SGLT-2 inhibitors in 63%, and no major changes in HF medication were introduced during the 6-month follow-up (Table S1). Additionally, no concurrent therapies including electrophysiological procedures, structural and coronary interventions were implemented during this period.
3.2. Periprocedural Data and Electrocardiographic Response
HBP, attempted primary in half of the study population, was successfully achieved in seven patients, and LBBAP was achieved in nine patients (LBBP: 6 and LVSP: 3). Periprocedural pneumothorax was observed in two patients, and pocket hematoma evacuation was needed in one patient. No other procedure-related complication was encountered. CSP lead revision due to the loss of His bundle capture was required in one patient and solved eventually with LBBAP (LVSP) shortly after the HBP lead implantation. Therefore, follow-up data were finally analyzed in 6 patients with HBP and 10 patients with LBBAP.
Table 3 summarizes the postoperative ECG features and the results of device interrogation and at 6-month follow-up. CSP resulted in a significant QRSd reduction indicated by delta QRS (25 ± 20 ms, p < 0.001). A complete elimination of RBBB was achieved by NS-HBP in all six patients, especially when higher pacing outputs were applied. In some patients, lower pacing output resulted in partial resolution of the RBBB pattern, while S-HBP resulted in no QRS correction in any patients. A marked decrease (20–40 ms) in QRSd with an incomplete attenuation of the RBBB pattern (reduction in R′ duration and amplitude) was observed in 6 out of 10 patients after LBBAP. QRSd increased in two patients after LBBAP. S-LBBP was intentionally not programmed, and pacing was delivered using NS-LBBP or LVSP. Anodal capture from the LBBAP lead during bipolar stimulation was used in 30% of patients during LBBAP.
3.3. Echocardiographic Response
Overall LVEF improved significantly from 27 ± 7% to 33 ± 9% (adjusted p = 0.01), and no change was observed in the RV function and diameter. Based on the echocardiographic criterion, 10/16 (62.5%) patients were classified as CSP responders, exhibiting almost a 10% increase in the LVEF. Improvement in LV function was in line with the echocardiographic changes indicating reverse LV remodeling. CSP resulted in a significant decrease in LV end-diastolic diameter (EDD, adjusted p = 0.01), end-systolic diameter (ESD, adjusted p = 0.001), as well as end-systolic volume (ESV, adjusted p = 0.02) and end-systolic volume index (ESVi, adjusted p = 0.02). After Holm–Bonferroni correction, no significant improvement was shown either in LV end-diastolic volume (EDV) and end-diastolic volume index (EDVi) or in stroke volume (SV) and stroke volume index (SVi; for further details, see Table 4).
3.4. LV Mechanical Outcomes
LV mechanical performance was characterized by assessing GLS, myocardial dyssynchrony and MW parameters. LV GLS improved significantly from −7 ± 3% to −10 ± 4% (adjusted p = 0.004; Figure 1A). Myocardial dyssynchrony was characterized by PSD, which decreased from 126 ± 28 ms to 96 ± 23 ms (adjusted p = 0.004, Figure 1B). CSP resulted in significant improvement in GWI (840 ± 306 mmHg%) as compared with the baseline (582 ± 277 mmHg%; adjusted p = 0.003, Figure 1C). GCW also increased significantly from 900 ± 374 mmHg% to 1203 ± 393 mmHg% (adjusted p = 0.006, Figure 1D). Additionally, GWW demonstrated a numerical decrease (from 313 ± 94 mmHg% to 294 ± 114 mmHg%) at 6 months without reaching the level of statistical significance (adjusted p = 0.36, Figure 1E). GWE improved significantly from 71 ± 7% to 77 ± 8% (adjusted p = 0.004; Figure 1F).
3.5. Clinical Outcomes
No HF hospitalization was required in any of the 16 patients during 6-month follow-up, and one patient was treated with electric cardioversion because of new-onset AF. An improvement of ≥1 NYHA functional class was demonstrated in 13 patients, while there was no change in 3 patients. Prior to the CSP, 12.5% of the patients were classified as NYHA II and 87.5% as NYHA III, while 25% were classified with NYHA I, 50% with NYHA II and 25% with NYHA III at 6 months (Figure 2A; adjusted p = 0.002). NT-proBNP level decreased significantly at the 6-month follow-up compared with the preoperative level (4093 ± 7215 ng/L at the baseline and 2087 ± 2082 ng/L at 6-month FU; adjusted p = 0.003; Figure 2B). Extremely elevated NT-proBNP (~35.000 ng/L) in one patient has disproportionately influenced variability. The 6 min walk distance increased significantly by an average of nearly 60 m (from 354 ± 88 m to 411 ± 95 m, adjusted p = 0.003; Figure 2C).
3.6. Subgroup Analysis
A subgroup analysis was performed between the patients’ cohorts treated with HBP versus with LBBAP (Table S2). Total procedure duration and fluoroscopy times, mean pacing threshold and R-wave sensing seemed to be more favorable with LBBAP as compared with HBP; however, after adjustment for multiple testing using the Holm–Bonferroni method, only the difference in the mean pacing threshold remained statistically significant (adjusted p-value = 0.019). No other between-group differences were found, either in the clinical outcomes or in the echocardiographic parameters; however, these comparisons were statistically underpowered owing to the limited sample size.
Additionally, baseline characteristics and perioperative data were comparable between CSP responders and non-responders; however, none of the above parameters reliably characterized these patient cohorts due to the small sample size within both groups.
4. Discussion
This was a single-center study on patients with HFrEF and RBBB ECG morphology undergoing CSP as a primary strategy for CRT. The main findings were as follows: (1) The significant reduction in QRSd after CSP was paralleled by signs of reverse cardiac remodeling and improved LV function. (2) CSP decreased the extent of LV dyssynchrony and improved LV MW. (3) CSP was associated with improved functional capacity, a lower NYHA functional class and reduced NT-proBNP levels.
Significant correlation has been demonstrated between the baseline ECG morphology and the long-term benefit after BVP. QRS width exceeding 150 ms and a typical LBBB pattern are considered the strongest predictor of resynchronization effect, while less benefit or even an increased mortality was reported in patients with RBBB [1,14]. A plausible explanation proposed for this finding could be that in patients with RBBB, the conduction delay is mainly present in the RV free wall and septum, leaving no room for significant improvement from LV free wall pre-excitation with BVP [15]. Additionally, recent studies suggest that RBBB is also associated with LV mechanical dyssynchrony in majority of the patients, although to a lesser degree than LBBB [16,17]. These findings are also supported by our data: significant LV mechanical dyssynchrony was indeed present in our patient cohort; however, no direct comparison with LBBB was available. In the present study, all patients fulfilled the guideline-based criteria (class IIa and b) for CRT implantation based on solely the QRSd and not the QRS morphology. However, considering the limited efficacy of BVP in RBBB [14] and emerging evidence supporting CSP as a more physiological alternative [18], CSP was selected here as the preferred resynchronization strategy over BVP. However, the present study is not intended to demonstrate superiority of CSP over BVP, but rather to characterize the effects of CSP in this specific patient cohort.
Correction or at least mitigation of the RBBB conduction delay pattern are considered signs of electrical resynchronization in patients with RBBB, although the mechanism is still not fully understood. In a recent report, permanent HBP applied as a primary strategy in patients with advanced HFrEF and RBBB was associated with significant narrowing in the QRSd and RBBB correction in 78% of patients (S-HBP in 34% and NS-HBP in 66%) [2]. In another study on patients with RBBB and preserved LVEF, NS-HBP resulted in a voltage-dependent attenuation of the RBBB pattern, which was not observed with S-HBP [19]. These results are in line with our observations: NS-HBP resulted in a voltage-dependent, complete QRS correction; however, no resolution of the RBBB pattern was associated during S-HBP. These findings may implicate the potential mechanism related to the modification of the RBBB pattern during HBP. The attenuation or correction of the RBBB pattern with NS-HBP but not with S-HBP may suggest a conduction block distal to the site of HBP and voltage-dependent capture of the right ventricular free wall myocardium or recruitment of parallel pathways resulting in pre-excitation of the area beyond the block. Even with no recruitment of RBB, the fusion between conduction over the His bundle (with RBBB pattern) and septal myocardial activation of the RV may still reduce the RV-LV activation delay [2,19,20].
HBP was performed in 6 of our patients, while LBBAP was performed in 10 of our patients. More than a 10 ms decrease in the QRSd with RBBB pattern attenuation was achieved in 60% of our patients who underwent successful LBBAP; however, QRSd increased in two patients. Both had apparent left-sided conduction system disease (left anterior hemiblock), and only LVSP was achieved. This phenomenon likely reflected LV septum activation with no effective recruitment of the conduction system leading to non-physiological ventricular activation. Comparable electrocardiographic response was demonstrated in the International LBBAP Collaborative Study [3]. Indeed, the magnitude of the QRS duration reduction observed in the present study is consistent with findings from recent reports [21,22]. This pattern of electric resynchronization was mainly achieved by either NS-LBBP or LVSP but less likely with S-LBBP, which might even be deleterious by inducing or preserving interventricular dyssynchrony and complete RBBB pattern. In contrast to S-LBBP, direct capture of the RV septal myocardium simultaneously with recruitment of the LBB conduction system observed both with NS-LBBP and LVSP might reduce the RV conduction delay. Nevertheless, LVSP was reported on worse clinical outcomes compared with LBBP, especially in those with reduced LVEF and wide QRS duration. While the magnitude of the interventricular dyssynchrony was comparable between these pacing strategies, NS-LBBP resulted in superior LV electrical and mechanical synchrony than LVSP [23]. These observations still warrant further validations in prospective randomized studies. Although CSP was associated with a significant reduction in LV mechanical dyssynchrony in our patient population, the limited sample size precluded robust subgroup analyses comparing HBP with LBBAP, as well as LVSP with LBBP. Further QRSd reduction could be achieved by anodal capture of the RV septum from the ring electrode with bipolar stimulation, which was present in 30% of our patients and in 48% of patients in the International LBBAP Collaborative study [24,25,26,27].
In addition to the RBBB, most of our patients had apparent left-sided conduction system disease (left anterior or posterior hemiblock) and prolonged AV conduction times (for further details see Table 2), which was similar to that reported in previous studies [2,3]. In the case of prolonged baseline PR interval, AV time optimization in addition to the correction of the RBBB pattern may contribute to the clinical improvement, as suggested by the findings of the HOPE-HF and a sub-analysis of the MADIT-CRT study [14,28,29]. Atypical RBBB, also referred to as masked LBBB, was found in 25% of our patients. The size of our patient cohort did not allow us to assess the impact of the above ECG features; however, the International LBBAP Collaborative Study found neither the baseline left-sided conduction delay nor the RBBB pattern normalization predictive for clinical response after LBBAP. Reduction in the paced QRS duration as compared with the baseline was the only independent predictor of the echocardiographic response [3].
Global and regional myocardial deformation and myocardial work (MW) was used to gain further insight into the mechanism of improvement after CRT, providing a loading-independent evaluation of myocardial performance and myocardial efficiency. Electro-mechanical synchronization of the chambers was reported to improve cardiac efficiency and energetics translating into an improvement in myocardial function and better outcomes, and both was achieved in our patient cohort [30]. A significant correlation was described between the global LV MW and the long-term prognosis in patients with various cardiac diseases [31]. Furthermore, both HBP and LBBAP have been associated with favorable changes in the cardiac energetics and MW parameters implemented in a wide range of pacing indications [7,32]. In our patient cohort, CSP increased GWI, GCW and GWE, which might be hypothesized as a potential link between improved mechanical synchrony and better echocardiographic and clinical outcomes. Nevertheless, the absence of any control group (e.g., optimal medical therapy alone or conventional BVP) represents a significant limitation in the interpretation of these findings, and hence, clear causality cannot be inferred.
5. Conclusions
To the best of our knowledge, this is the first study providing a detailed analysis of the mechanical synchrony and myocardial work after CSP in HFrEF patients with RBBB. We demonstrated that CSP with either HBP or LBBAP decreased LV mechanical dyssynchrony, which might lead to improved myocardial work and efficiency. Furthermore, CSP resulted in reverse cardiac remodeling and better clinical outcomes, which may support its use for cardiac resynchronization in this patient cohort. However, these data should be viewed as hypothesis-generating until being validated by a randomized trial including an adequate number of patients.
6. Limitations
This was a single-center, observational, non-randomized study including a limited number of patients. Such a limited sample may restrict statistical power, making it particularly challenging to perform subgroup analyses comparing HBP and LBBAP. In line with this, no baseline and postoperative parameters reliably discriminated CSP responders from non-responders due to the limited sample size. Another limitation is the lack of any control group or a direct comparison of CSP with the conventional BVP. Based on these limitations, any extrapolation from our data should be interpreted with caution before being validated in a prospective, randomized trial including a sufficient number of patients receiving optimized medical therapy alone or conventional BVP. Changes in HF symptoms, functional status and echocardiographic outcomes were used as the primary endpoint in our research with no results on long-term survival. Spontaneous fluctuations in HF status and delayed effects of medical therapy optimization cannot be fully excluded.
Although patients were treated with stable, optimized GDMT, medication adherence and other unmeasured concurrent interventions could not be formally assessed and may have contributed to the observed outcomes. Despite standardized, blinded image acquisition and analysis, inter- and intra-observer variability of advanced echocardiographic parameters (GLS, PSD, myocardial work) were not formally evaluated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Friedman D.J. Al-Khatib S.M. Dalgaard F. Fudim M. Abraham W.T. Cleland J.G.F. Curtis A.B. Gold M.R. Kutyifa V. Linde C. Cardiac Resynchronization Therapy Improves Outcomes in Patients With Intraventricular Conduction Delay But Not Right Bundle Branch Block: A Patient-Level Meta-Analysis of Randomized Controlled Trials Circulation 202314781282310.1161/CIRCULATIONAHA.122.06212436700426 PMC 10243743 · doi ↗ · pubmed ↗
- 2Sharma P.S. Naperkowski A. Bauch T.D. Chan J.Y.S. Arnold A.D. Whinnett Z.I. Ellenbogen K.A. Vijayaraman P. Permanent His Bundle Pacing for Cardiac Resynchronization Therapy in Patients With Heart Failure and Right Bundle Branch Block Circ. Arrhythm. Electrophysiol.201811 e 00661310.1161/CIRCEP.118.00661330354292 · doi ↗ · pubmed ↗
- 3Vijayaraman P. Cano O. Ponnusamy S.S. Molina-Lerma M. Chan J.Y.S. Padala S.K. Sharma P.S. Whinnett Z.I. Herweg B. Upadhyay G.A. Left bundle branch area pacing in patients with heart failure and right bundle branch block: Results from International LBBAP Collaborative-Study Group Heart Rhythm O 22022335836710.1016/j.hroo.2022.05.00436097454 PMC 9463705 · doi ↗ · pubmed ↗
- 4Jastrzebski M. Kielbasa G. Cano O. Curila K. Heckman L. De Pooter J. Chovanec M. Rademakers L. Huybrechts W. Grieco D. Left bundle branch area pacing outcomes: The multicentre European MELOS study Eur. Heart J.2022434161417310.1093/eurheartj/ehac 44535979843 PMC 9584750 · doi ↗ · pubmed ↗
- 5Leventopoulos G. Nastouli K.M. Bozika M. Papastavrou E. Apostolos A. Koros R. Perperis A. Koniari I. Vlassopoulou N. Chronopoulos P. Understanding LOT-CRT: Current Insights, Limitations, and Our Center’s Experience J. Clin. Med.202514302510.3390/jcm 1409302540364057 PMC 12072401 · doi ↗ · pubmed ↗
- 6Marzlin N. Hays A.G. Peters M. Kaminski A. Roemer S. O’Leary P. Kroboth S. Harland D.R. Khandheria B.K. Tajik A.J. Myocardial Work in Echocardiography Circ. Cardiovasc. Imaging 202316 e 01441910.1161/CIRCIMAGING.122.01441936734221 · doi ↗ · pubmed ↗
- 7Azzolini G. Bianchi N. Vitali F. Malagu M. Balla C. De Raffele M. Bertini M. A Comparative Assessment of Myocardial Work Performance during Spontaneous Rhythm, His Bundle Pacing, and Left Bundle Branch Area Pacing: Insights from the EMPATHY Study J. Cardiovasc. Dev. Dis.20231044410.3390/jcdd 1011044437998502 PMC 10672524 · doi ↗ · pubmed ↗
- 8Vijayaraman P. Chung M.K. Dandamudi G. Upadhyay G.A. Krishnan K. Crossley G. Bova Campbell K. Lee B.K. Refaat M.M. Saksena S. His Bundle Pacing J. Am. Coll. Cardiol.20187292794710.1016/j.jacc.2018.06.01730115232 · doi ↗ · pubmed ↗