The Role of Biological Effective Dose in Gamma Knife Radiosurgery: A Systematic Review Across Multiple Indications
Hao Deng, Xinyuejia Huang, Qian Wang, Yuan Gao, Mengqi Wang, Yang Wu, Xiaoman Shi, Maoyu Wang, Wei Pan, Senlin Yin, Wei Wang

TL;DR
This review explores how biological effective dose (BED) can improve Gamma Knife radiosurgery outcomes for various brain disorders.
Contribution
The paper systematically evaluates BED's role across multiple intracranial indications for the first time.
Findings
BED showed strong correlation with AVM obliteration rates.
BED improved prediction of hypopituitarism in pituitary adenomas.
Most evidence for BED comes from retrospective studies.
Abstract
Background: Gamma Knife radiosurgery (GKS) is widely used for the management of intracranial disorders. Emerging evidence suggests that incorporating the biological effective dose (BED) into GKS planning may improve the prediction of treatment efficacy and toxicity. This review aims to evaluate the role of BED in GKS across multiple intracranial indications. Methods: A qualitative review of published clinical studies was performed to assess the application of BED models in GKS for pituitary adenomas, vestibular schwannomas, meningiomas, arteriovenous malformations (AVMs), trigeminal neuralgia, and other disorders. The relationships between BED, treatment outcomes, and adverse effects were compared across indications. Results: The association between BED and clinical outcomes was most consistent in AVMs, where higher BED correlated closely with obliteration rates. In other diseases,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
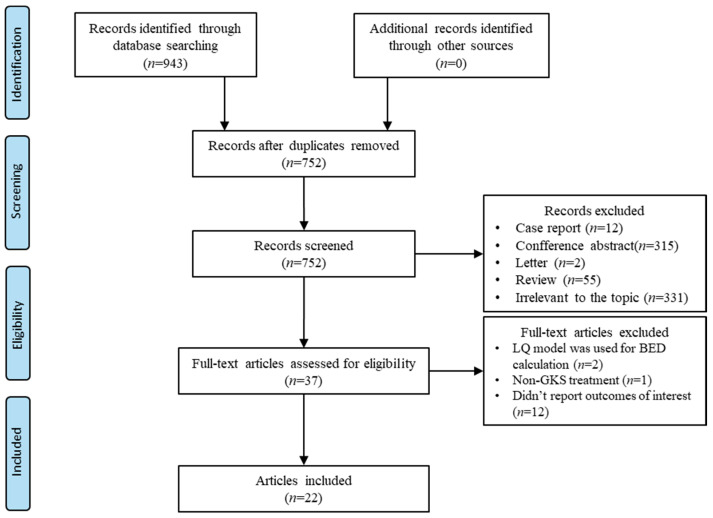 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Trigeminal Neuralgia and Treatments · Vascular Malformations Diagnosis and Treatment
1. Introduction
Gamma knife radiosurgery (GKS) is a widely used radiotherapy technique for treating intracranial disorders. It is now indicated for a large variety of diseases, including pituitary tumors, vestibular schwannomas, arteriovenous malformations (AVMs), meningiomas, metastases, and functional disorders [1,2,3,4,5]. GKS delivers a single, high-dose radiation treatment with submillimeter precision, which minimizes damage to adjacent healthy tissue [1]. Although previous studies have identified the recommended range of physical doses for various indications, determining the optimal radiation dose to maximize treatment efficacy while minimizing adverse effects remains a significant challenge.
Increasing evidence suggests that incorporating the biological effective dose (BED) into GKS treatment plans may enhance outcomes [6,7]. The concept of BED, introduced in 1989, quantifies the biological effectiveness of radiotherapy treatments [8], accounting for cellular DNA repair during radiation exposure [9]. While BED has been widely used in conventional fractionated radiotherapy, a model suitable for BED calculations in GKS was not proposed until recent years [10]. Moreover, rising interest in dose-rate modeling, the early integration of radiobiological parameters into contemporary treatment-planning systems, and the increasing availability of longitudinal outcome datasets have collectively renewed attention to BED-based approaches in GKS. These developments provide an opportunity to reassess how biological dose modeling may enhance treatment. Interest in integrating BED into radiosurgery planning has grown, with several studies examining its effects on GKS across various diseases [11,12,13]. However, no prior work has systematically summarized the evidence on BED across multiple GKS indications using a consistent radiobiological framework. To address this gap, we conducted a comprehensive literature review to evaluate the relationship between BED and treatment outcomes across diverse GKS applications, aiming to clarify the current evidence base and identify future directions for integrating BED into radiosurgery practice.
2. Methods
The PubMed-Medline, Ovid-Embase, and Cochrane Library databases were searched on 23 September 2025. The search strategy used the following terms: [“Gamma Knife” OR “GKS” OR “radiosurgery”] AND [“biological effective dose” OR “BED” OR “biologically effective dose”]. Only literature published in English was included.
The inclusion criteria were as follows: (a) GKS was performed for neurosurgical or neurofunctional diseases, (b) the effects of BED on the efficacy and/or safety outcomes of GKS were reported, and (c) BED calculation was based on the biexponential DNA repair model. While the traditional linear-quadratic (LQ) model is commonly used to estimate BED, it assumes a single exponential repair process and neglects sublethal damage repair during irradiation [14]. This simplification may not be suitable for GKS, where high-dose radiation is delivered over extended time periods [15]. In contrast, the biexponential DNA repair model accounts for both fast and slow repair kinetics, offering a more accurate representation of biological response by considering ongoing DNA repair during treatment [16]. Therefore, only studies that employed the biexponential model for BED estimation were included in this review. The BED formulation was presented in Supplementary Materials.
The exclusion criteria were: (a) full text was unavailable, (b) reviews, meta-analyses, conference abstracts, or commentary letters were excluded, and (c) studies that did not describe the BED model were excluded.
Literature selection and data extraction were performed independently by two reviewers (H.D., Q.W.). The reviewers screened the initial literature by reading the titles and abstracts. Eligible studies were then further evaluated through full-text reading by the same two reviewers. Discrepancies were first addressed through structured discussion to reach consensus; if disagreements persisted, a senior author (W.W. or S.Y.) served as an adjudicator to provide the final decision. The senior authors (W.W., S.Y.) were consulted when any inconsistencies and conflicts emerging. For each included study, the following data were extracted: the first author’s name, publication year, study type, baseline patient characteristics, disease type, GKS techniques, physical dose, BED, and other relevant data. Based on the GKS indications covered in the included studies, we collected all research findings related to the efficacy and safety of GKS, including but not limited to biochemical remission of pituitary tumors, changes in tumor volume, AVM obliteration, relief of trigeminal neuralgia, new-onset hypopituitarism, hearing loss, radiation-induced brain edema, and facial sensory loss. To assess the methodological quality and risk of bias of the included observational studies, we applied an adapted version of the Newcastle–Ottawa Scale (NOS), evaluating study selection, comparability, and outcome ascertainment. The results of this assessment are summarized in Supplementary Table S1. A total of 22 studies were included in this review. The selection process is depicted in the flow chart in Figure 1. The diseases covered in these studies included pituitary adenoma (n = 6) [12,17,18,19,20,21], meningioma (n = 3) [22,23,24], vestibular schwannomas (n = 4) [13,25,26,27], arteriovenous malformations (AVM) (n = 3) [7,11,28], melanoma brain metastases (n = 1) [29], trigeminal neuralgia (n = 4) [6,30,31,32], and essential tremor (n = 1) [33]. The characteristics of included studies are listed in Table 1. The Effects of BED and physical dose on treatment outcomes are presented in Table 2. This review was not registered in PROSPERO or other systematic review registries, which should be considered a methodological limitation. Table S3: PRISMA 2020 Checklist see the Supplementary Materials.
3. Results
3.1. Pituitary Adenoma
Among the studies that included pituitary adenoma, three focused on acromegaly, two on Cushing’s disease, and one on multiple pituitary adenomas. For acromegaly, the results from different centers were generally consistent. Two studies identified BED as a significant predictor of biochemical remission after GKS. Dumot et al. reported that the probability of biochemical remission in patients receiving a BED > 170 Gy_2.47_ was twice that of those receiving a lower BED (HR: 2.02, 95% CI: 1.06–3.86, p = 0.03) [21]. In a study by Graffeo et al., BED was significant for biochemical remission both as a continuous variable (HR: 1.01, 95% CI: 1.00–1.02, p = 0.02) and as a binary variable (BED > 200 Gy_2.47_, HR: 2.72, 95% CI: 1.36–5.13, p < 0.01) [17]. Another study showed that the higher BED group tended to have better endocrine remission at 9 years (70.2% vs. 48.2%, p > 0.05) [18]. Although the difference did not reach statistical significance, this qualitative trend aligned with the findings of the other two studies. Neither BED nor physical dose was significantly associated with post-GKS hypopituitarism.
For Cushing’s disease, both studies had rather limited sample sizes. Our center reported a significantly higher endocrine remission rate in the higher BED group (>205 Gy_2.47_) at 2 years after GKS (72.7% vs. 35.1%, p = 0.04) [12]. Balossier et al. presented a similar trend, though the difference was not statistically significant [19]. Graffeo et al. included a cohort with both secreting and non-secreting tumors. Their results indicated that mean gland BED, rather than BED alone, was significantly associated with post-GKS hypopituitarism (HR: 1.03, 95% CI: 1.02–1.05, p < 0.001) [20]. However, neither physical dose nor BED nor mean gland BED were associated with treatment success. Additionally, although mean gland dose was a predictor of post-GKS hypopituitarism (HR: 1.31, 95% CI: 1.16–1.47, p < 0.001), the BED-based model demonstrated better predictive efficacy compared to physical dose-based models.
3.2. Meningioma
Huo et al. reported the largest meningioma cohort (n = 336) among the included studies [23]. The effects of BED on local tumor control varied across different WHO grades. In a cohort of 354 grade I lesions, a BED > 50 Gy_2.47_ was significantly associated with a lower incidence of local failure (p < 0.01). Similarly, another study involving 91 cases of parasellar meningioma (WHO grade I or presumed grade I) also found that BED was a significant predictor of local control (HR: 0.96, 95% CI: 0.92–1.00, p = 0.03) [24]. However, Dedeciusova et al. reported mixed results, finding no significant association between BED and clinical improvement or tumor control [22]. Their study, which included only 46 cases, may have lacked sufficient statistical power to detect a significant effect. Notably, none of the included studies addressed the impact of BED on the safety of GKS.
3.3. Vestibular Schwannomas
The studies on vestibular schwannomas showed heterogeneous results. The largest cohort study failed to find a significant association between BED and either tumor control or symptomatic edema [25]. However, Tuleasca et al. reported a significantly positive association between BED and tumor volume changes (β = −0.17, p < 0.01) [13]. Additionally, Tuleasca et al. explored the relationship between BED at specific sites and hearing decline. Both tumor BED and mean cochlea BED were significantly related to hearing decline at various time points [26,27]. Interestingly, mean cochlea dose, rather than tumor dose, was significantly associated with hearing decline at 24 months.
3.4. Arteriovenous Malformation
All three included studies indicated that BED was a significant predictor of AVM obliteration after GKS. Nesvick et al. reported that the probability of obliteration in patients with a BED > 133 Gy_2.47_ increased by 52% compared to those receiving a lower BED (HR: 1.52, 95% CI: 1.19–1.95, p < 0.01) [11]. In another study, patients with a BED > 180 Gy_2.47_ had more than twice the probability of obliteration (HR: 2.11, 95% CI: 1.30–3.40, p < 0.01) [28]. Tuleasca et al. developed a predictive model for AVM obliteration after GKS, which showed that BED was the strongest predictor of obliteration in unruptured AVMs (HR: 1.015, 95% CI: 1.001–1.029, p = 0.03) [7]. Additionally, they found that BED had greater predictive power than physical dose. Although Nesvick et al. reported on the largest cohort, their study did not address the effects of BED on the safety of GKS. The other two studies showed that neither BED nor physical dose were significantly associated with post-GKS complications.
3.5. Trigeminal Neuralgia and Other Indications
Tuleasca et al. reported the earliest results of BED on TN. They observed a trend of increasing hypoesthesia with higher BED, but did not find a definitive relationship between BED and pain relief [30]. The following studies showed that effects of BED on TN may vary for different trigeminal nerve target. A multicenter cohort including 871 cases of type 1 TN showed that a BED ≥ 2100 Gy_2.47_ was significantly associated with initial pain relief for the distal target (HR: 1.46, 95% CI: 1.05–2.03, p = 0.03) [6]. For the proximal target, physical dose rather than BED was a significant predictor of initial pain relief (HR: 1.79, 95% CI: 1.05–3.05, p = 0.03). However, neither BED nor maximal dose was associated with post-GKS sensory dysfunction for either proximal or distal target. Similarly, results of our center also showed target heterogeneity of BED [32]. For patients with distal targets, BED was a significant predictor of treatment failure (OR: 0.996, 95% CI: 0.992–0.999, p = 0.02) and post-GKS complications (OR: 1.002, 95% CI: 1.000–1.004, p = 0.01). BED did not significantly influence outcomes in the proximal target subgroup, either for treatment failure or complications. Tang et al. combined BED with target volumes to explore the association between BED coverage and treatment outcomes [31]. The results indicated that V%CN V-BED1000, rather than BED alone, was a significant predictor of pain relief (OR: 1.05, 95% CI: 1.04–1.07, p < 0.01), quality of life (OR: 1.05, 95% CI: 1.04–1.07, p < 0.01), and medication withdrawal (OR: 1.05, 95% CI: 1.04–1.05, p < 0.01). Additionally, the maximal BED received by the brainstem was a significant predictor of post-GKS complications (OR: 1.06, 95% CI: 1.05–1.06, p < 0.01).
Only one study reported results on essential tremor (ET) [33]. Increasing BED was associated with improvement in the ET rating scale (β = −0.029, p = 0.04). Adverse radiation events tended to occur in cases receiving high BED (>4500 Gy_2.47_). Zubatkina et al. used multiple α/β ratios (3, 5, 10, 15) to calculate BED in melanoma brain metastases [29]. BED, based on various α/β ratios, was significantly associated with local control after GKS. Furthermore, BED calculated with an α/β ratio of 15 demonstrated better predictive efficacy for local control compared to the margin dose (AUC: 0.85 vs. 0.79). Neither BED nor margin dose was significantly associated with radiation necrosis. The interpretive strength of findings for essential tremor and melanoma brain metastases is limited, as each indication was represented by only a single eligible study. Consequently, conclusions for these categories should be regarded as preliminary, and additional standardized, high-quality investigations are required to validate these observations.
4. Discussion
Our review indicates that BED may play a meaningful role in influencing clinical outcomes across a variety of GKS indications. The most consistent findings were observed for AVMs, where all studies identified BED as a significant predictor of obliteration. Results for pituitary adenomas also showed a relatively coherent pattern, with multiple studies demonstrating associations or trends between BED and endocrine remission, while mean gland BED emerged as a predictor of post-GKS hypopituitarism. In contrast, for indications such as TN, meningioma, and VS, study findings were more variable, likely reflecting differences in target selection, coverage metrics, and study methodology. The limited evidence available for essential tremor and melanoma brain metastases should be interpreted cautiously, as each was represented by a single study. We have summarized the indication-specific BED thresholds in the Supplementary Table S2.
Early radiobiological work quickly recognized that treatment outcomes depend not only on the physical dose but also on its biological effectiveness [14]. Currently, BED is widely applied in conventional fractionated radiotherapy, where numerous clinical series have linked higher BED values to improved tumor control and survival across various diseases [34,35,36]. However, unlike conventional radiotherapy, GKS delivers a very high dose through single or multiple isocenters over a long period of time. This generates steep intracranial dose gradients, allowing DNA repair to begin during—rather than after—irradiation. A variety of studies suggest that the administration of a single, high dose of radiation in vivo has a much greater effect than that which would be predicted from the LQ model using the coefficients calculated from conventional in vitro dose/fractions [15]. Modeling studies have shown that the LQ-based BED can misestimate biological effects in GKS [37,38]. To address this, Jones et al. introduced a biexponential, time-corrected BED framework for GKS, which explicitly accounts for both fast and slow DNA repair kinetics during protracted single-session treatments [10]. All studies included adopted this BED model, which helped reduce bias and heterogeneity.
The physical dose used in GKS varied substantially across indications, and dose selection is still largely empirical. Due to the varying dose rate of Co^60^, the delivery time for a given physical dose can differ considerably. Sublethal DNA damage begins to repair while irradiation is still ongoing [10]. Therefore, the same prescribed dose in GKS may produce different biological effects, especially when the dose rate varies widely. Some studies have explored the impact of dose rate. Lee et al. and Barzaghi et al. reported that a higher dose rate was associated with a lower likelihood of recurrence for TN [39,40]. Huo et al. found that meningioma patients treated with lower dose rates had a higher incidence of local failure compared to those treated with higher dose rates. However, Tuleasca et al. found no significant association between dose rate and AVM obliteration or post-SRS complications [7]. The introduction of BED in GKS allows for dose–time compensation that physical dosimetry fails to account for. Notably, three studies directly compared BED with physical dose and showed that BED provided superior predictive performance for hypopituitarism, AVM obliteration, and local control in melanoma brain metastases [7,20,29]. This potential advantage suggests that clinicians may benefit from consciously incorporating BED into GKS planning. Some low-level evidence even suggested a specific BED range for certain indications, though these BED ranges require further validation [21,33]. Additionally, BED may offer personalized dose constraints for organs at risk. For example, incorporating BED into planning has been shown to refine cochlear and brainstem limits and correlate more closely with hearing preservation outcomes after vestibular schwannoma GKS than physical dose alone [27].
Several studies highlighted that BED-derived parameters such as volume-based BED coverage and mean gland BED, may better characterize the biological distribution of dose than gross BED [20,31]. For instance, the use of mean gland BED rather than gross lesion BED underscores the differing radiosensitivities of surrounding anatomical structures and reinforces the importance of sparing critical tissues during GKS planning. Likewise, volume-based BED coverage reflects not only the existence of an effective BED threshold but also the necessity of achieving adequate biological dose coverage across the target, combining both dose adequacy and spatial distribution into a single metric. Together, these multidimensional BED-derived parameters may offer a potentially more predictive framework than gross BED alone, although further validation is still required. Current commercial GKS planning systems do not natively compute BED, but BED-based corrections can be implemented via exported dose-rate data, custom calculation modules, or research-grade plugins. Incorporating BED requires familiarity with radiobiological modeling, which introduces a learning curve for clinicians. However, the increasing availability of automated BED calculators and scripting interfaces makes that practical implementation is feasible.
One of the limitations is that the same radiobiological parameters were used for BED estimation across different histological types. For instance, the α/β ratio for normal brain tissue was assumed to be 2.47 Gy [41], and all studies, except for that on melanoma brain metastases, used 2.47 Gy as the α/β ratio. While this approach serves as a compromise due to the current lack of histology-specific parameters, it introduces potential systematic errors when applying BED in GKS. According to the BED formulation, Underspecifying α/β leads to an overestimation of BED, whereas overspecifying it causes underestimation. Using a uniform α/β ratio of 2.47 Gy across diverse histologies may distort the magnitude of BED, alter BED–outcome correlations, and destabilize disease-specific BED thresholds, underscoring the importance of deriving histology-specific radiobiological parameters. Zubatkina et al. explored various α/β ratios in BED estimation and found that α/β ratios of 10 Gy and 15 Gy might be more appropriate for melanoma brain metastases based on clinical outcomes [29]. Reverse outcome-based modeling may therefore offer a feasible and informative strategy for establishing histology-specific radiobiological parameters. However, such analyses require large, well-characterized cohorts with standardized definitions of endpoints and harmonized dose-time reporting, necessitating multi-center collaboration. Importantly, clinically derived α/β ratios should ideally be cross-validated with parameters obtained from biological experiments, which may help refine BED estimation and improve the robustness of radiobiological modeling in GKS. Finally, substantial heterogeneity existed across studies. Variability in study design (single-center vs. multicenter cohorts), inconsistency in outcome definitions and the use of different GKS platforms across institutions may all introduce methodological inconsistency. Moreover, marked variation in follow-up duration and baseline characteristics, including age distribution and sex ratio, further complicates direct comparison. These differences may partially explain the inconsistency of findings for certain indications.
Overall, BED appears to be a significant factor across a wide range of GKS indications. This observation suggests that BED-driven optimization could serve as a unifying framework for GKS planning. While integrating BED into treatment planning offers valuable biological insights and may complement traditional physical dose parameters, whether BED can ultimately replace physical dose as the primary planning metric remains uncertain. All of the supporting evidence is retrospective and rarely incorporates prospectively collected data on toxicity or treatment efficacy endpoints. Prospective studies are essential to determine whether BED-optimized plans improve outcomes compared to standard physical dose prescriptions.
5. Conclusions
Our review suggests that BED may play a meaningful role in influencing clinical outcomes across a range of GKS indications. Among these, the association between BED and treatment efficacy is most consistent in AVMs, where BED aligns closely with obliteration rates. For other indications, including vestibular schwannoma and meningioma, these results remain more variable, though several studies support the potential utility of BED. While integrating BED into treatment planning offers valuable biological insights and may complement traditional physical dose parameters, whether BED can ultimately replace physical dose as the primary planning metric remains uncertain. Further research is needed to determine histology-specific radiobiological parameters for more precise BED estimation and to validate the routine clinical utility of BED through prospective studies especially those incorporating standardized toxicity endpoints, functional outcome measures, and harmonized radiobiological reporting.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leksell L. Stereotactic radiosurgery J. Neurol. Neurosurg. Psychiatry 19834679780310.1136/jnnp.46.9.7976352865 PMC 1027560 · doi ↗ · pubmed ↗
- 2Tuleasca C. Régis J. Sahgal A. De Salles A. Hayashi M. Ma L. Martínez-Álvarez R. Paddick I. Ryu S. Slotman B.J. Stereotactic radiosurgery for trigeminal neuralgia: A systematic review J. Neurosurg.201913073375710.3171/2017.9.JNS 1754529701555 · doi ↗ · pubmed ↗
- 3Mahajan U.V. Desai A. Shost M.D. Cai Y. Anthony A. Labak C.M. Herring E.Z. Wijesekera O. Mukherjee D. Sloan A.E. Stereotactic radiosurgery and resection for treatment of multiple brain metastases: A systematic review and analysis Neurosurg. Focus 202253 E 910.3171/2022.8.FOCUS 2236936321293 · doi ↗ · pubmed ↗
- 4Kondziolka D. Functional radiosurgery Neurosurgery 199944122012–20; discussion 20–1210.1097/00006123-199901000-000059894959 · doi ↗ · pubmed ↗
- 5Marchetti M. Sahgal A. De Salles A.A.F. Levivier M. Ma L. Paddick I. Pollock B.E. Regis J. Sheehan J. Suh J.H. Stereotactic Radiosurgery for Intracranial Noncavernous Sinus Benign Meningioma: International Stereotactic Radiosurgery Society Systematic Review, Meta-Analysis and Practice Guideline Neurosurgery 20208787989010.1093/neuros/nyaa 16932463867 PMC 7566438 · doi ↗ · pubmed ↗
- 6Warnick R.E. Paddick I. Mathieu D. Adam E. Iorio-Morin C. Leduc W. Hamel A. Johnson S.E. Bydon M. Niranjan A. The relevance of biologically effective dose for pain relief and sensory dysfunction after Gamma Knife radiosurgery for trigeminal neuralgia: An 871-patient multicenter study J. Neurosurg.202414146147310.3171/2023.12.JNS 23156938364220 · doi ↗ · pubmed ↗
- 7Tuleasca C. Peciu-Florianu I. Leroy H.A. Vermandel M. Faouzi M. Reyns N. Biologically effective dose and prediction of obliteration of unruptured arteriovenous malformations treated by upfront Gamma Knife radiosurgery: A series of 149 consecutive cases J. Neurosurg.20211341901191110.3171/2020.4.JNS 20125032707557 · doi ↗ · pubmed ↗
- 8Fowler J.F. 21 years of biologically effective dose Br. J. Radiol.20108355456810.1259/bjr/3137214920603408 PMC 3473681 · doi ↗ · pubmed ↗