Sex Differences in Preoperative Risk Profiles and 1-Year Mortality Following Elective Cardiac Surgery: A Retrospective Single-Centre Cohort Study
Caitlin Bozic, Magnus Strypet, Floor J. Mansvelder, Evert K. Jansen, Jennifer S. Breel, Henning Hermanns, Susanne Eberl

TL;DR
This study finds that women and men have different pre-surgery risk factors that affect their chances of surviving one year after heart surgery.
Contribution
The study identifies sex-specific preoperative risk profiles that influence postoperative mortality in cardiac surgery patients.
Findings
Female non-survivors had higher rates of systemic diseases like kidney dysfunction and pulmonary hypertension.
Male non-survivors were more likely to have direct cardiac issues like severe left ventricular dysfunction and myocardial infarction.
The study highlights the need for sex-specific approaches in perioperative risk assessment and management.
Abstract
Background: Sex-related differences in outcomes following cardiac surgery are well documented, with females generally experiencing higher postoperative mortality rates than males. However, the underlying factors driving this disparity remain incompletely understood. This study aimed to compare the preoperative risk characteristics of female and male patients who died within one year after elective cardiac surgery with those who survived, in order to identify sex-specific risk profiles associated with postoperative mortality. Methods: In this retrospective single-centre cohort study, data were derived from a prospective quality assurance database at Amsterdam University Medical Centres (Amsterdam UMC), The Netherlands, covering January 2001 to December 2020. All adult patients (≥18 years) undergoing elective cardiac surgery were included. Descriptive and comparative analyses were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
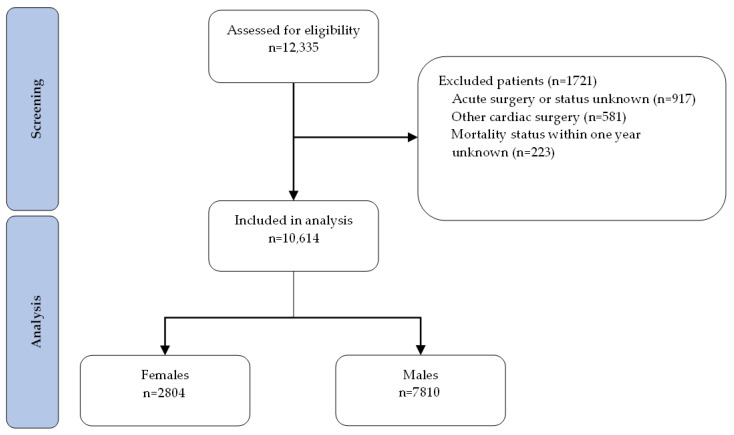 Figure 1
Figure 1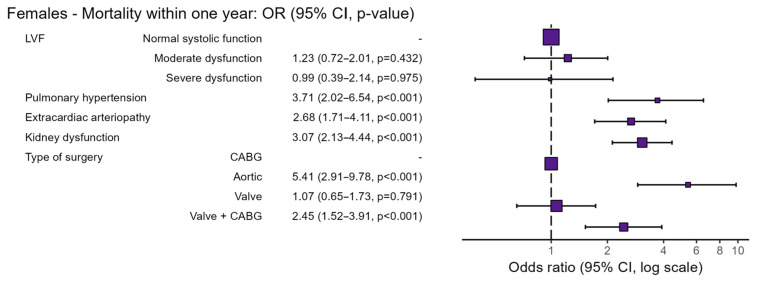 Figure 2
Figure 2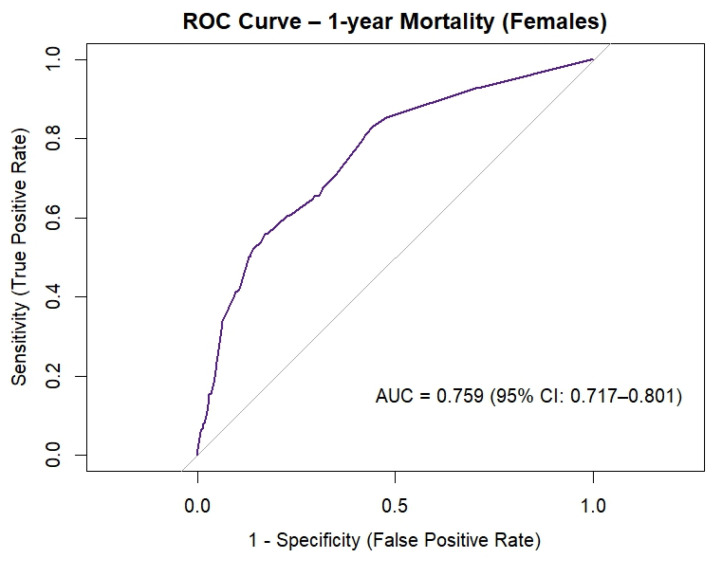 Figure 3
Figure 3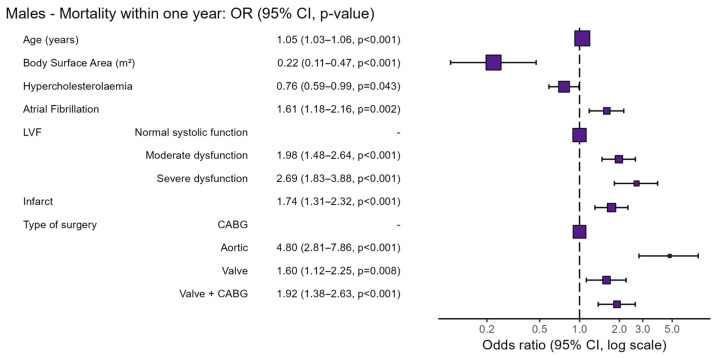 Figure 4
Figure 4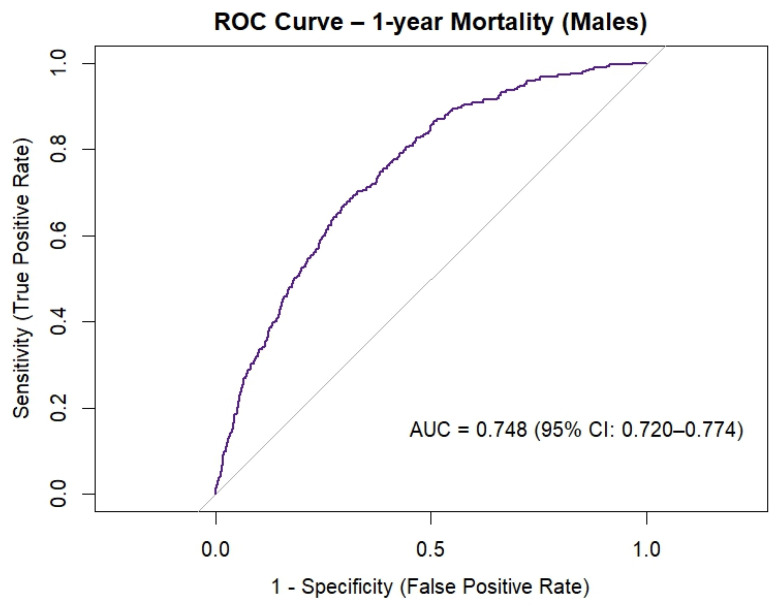 Figure 5
Figure 5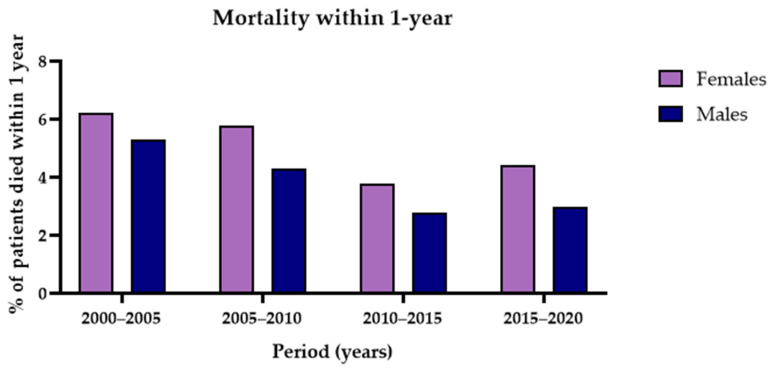 Figure 6
Figure 6- —BJA ESAIC
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Cardiac, Anesthesia and Surgical Outcomes · Cardiac Valve Diseases and Treatments
1. Introduction
Existing research consistently demonstrates that females undergoing cardiac surgery face a higher risk of mortality than males, both in the short and long term [1,2,3]. However, existing research often provides descriptive accounts of this disparity without clearly defining the preoperative causal factors that drive it. Commonly used preoperative risk prediction models, such as the EuroSCORE II, estimate surgical risk and support clinical decision-making before surgery [4]. Yet the inclusion of female sex as an independent risk factor in the EuroSCORE is problematic, as it reflects historical treatment differences rather than inherent biological susceptibility. Historically, female patients were older, referred later for intervention, and presented with smaller body size or more complex valve pathology, which collectively inflated their observed mortality rates. As a result, these models may encode a systemic bias that overestimates risk in contemporary cardiac surgery in female patients, potentially reinforcing inequities in access to appropriate surgical interventions. In essence, sex is treated as a static causal determinant and as a binary risk factor, with females assigned a higher baseline risk. This approach may obscure clinically relevant differences and limit opportunities for targeted optimisation in both sexes.
While age, comorbidities, and previous cardiac surgery [2,4,5,6] are recognised predictors of mortality, it remains unclear how the profile of these factors differ between surviving and non-surviving patients, specifically if stratified by sex. In particular, the specific preoperative characteristics of female and male patients who do not survive the first year after surgery are largely unknown. Identifying these patterns is crucial for refining risk assessment and guiding more personalised perioperative strategies.
Therefore, we conducted this retrospective cohort study at a Dutch academic medical centre and aimed to define and compare the preoperative risk profiles of female and male patients who died within one year of elective cardiac surgery. Secondary analyses aimed to develop sex-specific association models using logistic regression to identify key predictors of mortality in each group.
2. Materials and Methods
2.1. Study Design
This retrospective, single-centre, observational study analysed prospectively collected quality assurance data from all adult (≥18 years) patients who underwent elective cardiac surgery (coronary artery bypass grafting (CABG), aortic, valve or combined CABG/valve surgery) in the Amsterdam University Medical Centres (Amsterdam UMC), the Netherlands, between January 2001 and December 2020.
2.2. Ethical Considerations
On 10 February 2022, the Institutional Review Board of Amsterdam UMC confirmed that this study did not fall under the Medical Research involving Human Subjects Act and waived the need for individual patient consent (W22_050#22.081). This study was registered on ClinicalTrials.gov on 10 March 2022 (NCT06554925). This analysis adhered to the principles outlined in the Declaration of Helsinki (Helsinki, 2024) [7]. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines were used in writing of this report [8].
2.3. Study Outcomes
The primary outcome was to characterise and compare the preoperative risk profile of female and male patients who died within one year following elective cardiac surgery with those of survivors. Secondary outcomes included developing sex-specific association models using logistic regression.
To evaluate one-year mortality, preoperative variables were analysed as potential risk factors if they showed differences between survivors and non-survivors within each sex. Variables demonstrating such differences were first identified and subsequently checked for sex-specificity. Variables unique to either sex were then included in the respective sex-specific risk profile. This stepwise approach allowed for the identification of preoperative factors associated with one-year mortality that were unique to females and males. Secondary analyses were performed to construct sex-specific logistic regression models. All preoperative variables identified as unique to either sex were considered candidates for inclusion. Model performance was evaluated using ROC curves, and the area under the curve (AUC) was calculated to assess the discriminative ability of each sex-specific model.
2.4. Data Sources and Measurements
All data were prospectively collected as part of a mandatory institutional quality assurance database. Data were verified after discharge by the same cardiac surgeon (EKJ) for the entire study period to ensure accuracy and completeness. Vital status was obtained through annual linkage to the national civil registry, which is linked to social security numbers, enabling reliable assessment of all-cause mortality within one year of surgery.
2.5. Definitions and Variables
All-cause mortality was defined as death from any cause, assessed cumulatively over the entire study period. One-year mortality referred to death within one year of the index surgery. Mortality within one year-after surgery was chosen as the primary outcome to include both early and intermediate deaths plausibly related to the surgical procedure and preoperative risk profile and allowing for comparison with previous studies.
Elective cardiac surgery included admissions for isolated or combined procedures involving CABG, valve, or aortic surgery.
A critical preoperative state was defined as hemodynamic instability requiring support such as inotropes, mechanical ventilation, or intra-aortic balloon pump. Reoperation was defined as surgery in patients with a history of previous cardiac surgery. A familial medical history referred to a documented family history of cardiovascular disease.
Left ventricular function (LVF) was categorised as normal: preserved systolic function; moderate dysfunction: moderately reduced ejection fraction; and severe dysfunction: severely reduced ejection fraction.
Infarct referred to myocardial infarction (MI), classified as ongoing: acute MI at the time of surgery or past 90 days: MI occurring within three months before surgery.
Pulmonary hypertension indicated elevated pulmonary arterial pressures (>25 mmHg). Extracardiac arteriopathy indicated the presence of clinically significant atherosclerotic disease in arteries outside the heart.
Neurological dysfunction referred to motor, sensory, or cognitive impairment. Kidney dysfunction was defined as an estimated glomerular filtration rate (eGFR) below 55 mL/min/1.73 m^2^.
2.6. Sample Size
No formal sample size calculation was performed. The study population comprised all patients who underwent elective cardiac surgery at Amsterdam UMC between January 2001 and December 2020. The total number of eligible patients during this period defined the sample size.
2.7. Statistical Analysis
Prior to analysis, data were checked for accuracy, missing data, outliers, and normality. The normality of continuous data was assessed by visual inspection of histograms, Q-Q plots, and boxplots. Statistical analysis was performed using R Studio version 4.4.3 (2025-02-28 ucrt).
Patient characteristics were presented using descriptive statistics. Normally distributed continuous data were presented as mean and standard deviation (SD). Non-normally distributed continuous data were presented as the median and interquartile range (IQR). Categorical variables were presented as numbers and percentages.
Sex-specific logistic regression models were used to determine the association of several preoperative variables and all-cause mortality within one year. All sex-specific variables were first entered into univariable logistic regression analyses, and those remaining significant were subsequently included in multivariable logistic regression models. Analyses were conducted separately for females and males. A p-value ≤ 0.05 was considered statistically significant.
3. Results
3.1. Study Population
Between January 2001 and December 2020, a total of 12,335 patients who underwent cardiac surgery at Amsterdam UMC were assessed for eligibility (Figure 1). Of these, 917 patients were excluded due to acute surgical indication or because the status was unknown, 581 because they had procedures outside the scope of interest (i.e., other than CABG, valve, valve + CABG or aortic surgery), and 223 due to unknown one-year postoperative mortality status. The final study cohort consisted of 10,614 patients, comprising 2804 females and 7810 males.
3.2. Patient Characteristics
3.2.1. Females
Preoperative characteristics of female patients are presented in Table 1. Among the 2804 females included, 5.1% (n = 143) died within one year of surgery. The median age was 72 years [IQR 65–77], and the mean Body Surface Area (BSA) was 1.80 m^2^ (SD ± 0.17).
Compared with female survivors, female non-survivors more frequently had a history of reoperation (9% vs. 3%), atrial fibrillation (21% vs. 13%), moderate LVF (16% vs. 11%), pulmonary hypertension (12% vs. 3%), extracardiac arteriopathy (25% vs. 9%), chronic obstructive pulmonary disease (COPD) (18% vs. 10%), cerebrovascular accident/transient ischemic attack (CVA/TIA) (18% vs. 9%), and kidney dysfunction (46% vs. 21%). Non-survivors also had lower haemoglobin (median 7.8 mmol/L [IQR 7.1–8.4] vs. 8.1 mmol/L [7.6–8.6]). Surgical procedure type also differed; AVR was more common among non-survivors (50% vs. 38%).
3.2.2. Males
Preoperative characteristics of male cardiac surgery patients are presented in Table 2. Of the 7810 males included, 3.8% (n = 299) died within one year of surgery. The median age was 67 years [IQR 59–73], and the mean BSA was 2.01 m^2^ (SD ± 0.18).
Compared with male survivors, male non-survivors were older (median age 73 years [IQR 66–77] vs. 67 years [59–73]) and had a smaller mean BSA (mean 1.96 m^2^ ± 0.19 vs. 2.02 ± 0.18 m^2^). They more frequently had a history of reoperation (10% vs. 4%), atrial fibrillation (23% vs. 11%), severe LVF (14% vs. 6%), myocardial infarction (31% vs. 22%), pulmonary hypertension (7% vs. 2%), COPD (17% vs. 8%), CVA/TIA (17% vs. 8%), and kidney dysfunction (35% vs. 9%).
Male non-survivors had lower median haemoglobin levels (median 8.2 mmol/L [IQR 7.3–8.9] vs. 8.9 mmol/L [8.3–9.4]) and were less likely to have a familial history of cardiovascular disease (23% vs. 30%). Procedural differences were also observed; AVR was more frequent among non-survivors (30% vs. 24%), whereas LIMA use was less common (61% vs. 73%).
3.3. Sex-Specific Preoperative Risk Profile
In total, 143 of 2804 females (5.1%) and 299 of 7810 males (3.8%) died within one year of elective cardiac surgery. Several risk factors were shared by both female and male non-survivors, including reoperation, smoking, COPD, CVA/TIA, and lower haemoglobin levels. These common factors were excluded from the sex-specific risk profiles. Given that the type of surgery is known preoperatively, we incorporated the distinct outcome profiles for each surgical type into the preoperative risk assessment.
3.3.1. Females
Preoperative risk factors specific for female patients undergoing cardiac surgery are shown in Table 3 and Figure 2. In non-surviving females, moderate LVF was more prevalent (16% vs. 11%; OR 1.23, 95% CI 0.72–2.01, p = 0.432). Pulmonary hypertension was also more prevalent (12% vs. 3%; OR 3.71; 95% CI 2.02–6.54, p < 0.001), as were extracardiac arteriopathy (25% vs. 9%; OR 2.68; 95% CI 1.71–4.11, p < 0.001) and kidney dysfunction (46% vs. 21%; OR 3.07; 95% CI 2.13–4.44, p < 0.001). The type of surgery was another key determinant of mortality; non-surviving females more frequently underwent combined valve and CABG surgery (29% vs. 15%; OR 2.45; 95% CI 1.52–3.91, p < 0.001) and aortic surgery (14% vs. 4%; OR 5.41; 95% CI 2.91–9.78, p < 0.001).
Figure 3 shows the goodness of fit of the preoperative risk profile of female patients undergoing cardiac surgery, measured with the ROC curve. The AUC for the female risk profile was 0.759 (95% CI 0.717–0.801) and was considered acceptable.
3.3.2. Males
Preoperative risk factors specific for male patients undergoing cardiac surgery are shown in Table 4 and Figure 4. Non-surviving males were older (median [IQR] 73 [66–77] vs. 67 [59–73]; OR 1.05; 95% CI 1.03–1.06, p < 0.001) and had lower BSA (1.96 m^2^ ± 0.19 vs. 2.02 m^2^ ± 0.18; OR 0.22; 95% CI 0.11–0.47, p < 0.001). Moreover, severe LVF was more prevalent among non-surviving males (14% vs. 6%; OR 2.69; 95% CI 1.83–3.88, p < 0.001), as was a history of myocardial infarction (31% vs. 22%; OR 1.74; 95% CI 1.31–2.32, p < 0.001). Conversely, hypercholesterolaemia was less prevalent in non-surviving males (35% vs. 44%; OR 0.76; 95% CI 0.59–0.99, p = 0.043).
Also, the type of surgery played a significant role as a risk factor; non-surviving males more frequently underwent a combination of valve and CABG surgery (22% vs. 12%; OR 1.92; 95% CI 1.38–2.63, p < 0.001) and aortic surgery (9% vs. 3%; OR 4.80; 95% CI 2.81–7.86, p < 0.001).
Figure 5 shows the goodness of fit of the preoperative risk profile of male patients undergoing cardiac surgery, measured with the ROC curve. The AUC for the male preoperative risk profile was 0.748 (95% CI 0.720–0.774) and was considered acceptable.
3.4. Mortality over Time
This study was conducted between January 2001 and December 2020. Figure 6 illustrates the proportion of patients who died within one year of surgery, stratified by sex. Over the 20-year study period, one-year postoperative mortality decreased in both females and males.
4. Discussion
In this large, single-centre retrospective cohort study, we aimed to move beyond treating sex as a monolithic risk factor and instead characterise the distinct preoperative profiles associated with one-year mortality in females and males undergoing elective cardiac surgery. Our primary finding was that the risk factors for mortality differ significantly between the sexes. For female patients, one-year mortality was independently associated with a profile of systemic vascular and end-organ dysfunction, specifically pulmonary hypertension, extracardiac arteriopathy, and kidney dysfunction, as well as undergoing more complex procedures (combined valve/CABG or aortic surgery). In contrast, mortality in male patients was predominantly associated with older age, lower BSA, and markers of more advanced cardiac-specific damage, such as severe left ventricular dysfunction and a history of myocardial infarction. Both sex-specific models demonstrated acceptable discriminative ability, with AUCs of 0.759 for females and 0.748 for males, reinforcing the validity of a sex-differentiated approach to risk stratification.
Our findings in female patients contextualise and extend the existing literature, consistently reporting higher mortality for females after cardiac surgery [1,2,3]. While previous studies typically adjusted for sex as a binary covariate, our analysis reveals that these disparities stem from distinct underlying risk phenotypes. The female mortality profile, marked by moderate left ventricular function, pulmonary hypertension, extracardiac arteriopathy and kidney dysfunction, suggests advanced, systemic vasculopathy and multi-organ compromise. This aligns closely with modern evidence that females are more likely to present with coronary microvascular disease (CMD), particularly those with chronic comorbidities and heart failure with preserved ejection fraction (HFpEF), where CMD is highly prevalent and leads to increased mortality and hospitalisation risk [9]. Recent large studies show up to 75% of HFpEF patients, most of whom are female, exhibit CMD, often accompanied by pulmonary hypertension and systemic endothelial impairment, echoing the constellation we observed [10,11]. Additionally, CMD in these patients is linked with diastolic dysfunction and adverse outcomes, reinforcing the interdependence between microvascular disease, end-organ compromise, and increased surgical risk [10,11,12].
The male mortality profile, driven by older age, atrial fibrillation, severe LV dysfunction, and prior myocardial infarction, reflects a more “classic” ischemic cardiomyopathy pathway, which is well-documented in the cardiac surgery literature [2,5,6]. The association of lower BSA with higher mortality in males is also a key finding, likely serving as a proxy for frailty or sarcopenia, which are increasingly recognised as powerful independent predictors of poor postoperative outcomes [13]. Interestingly, our model identified hypercholesterolemia as a protective factor in males. This seemingly paradoxical finding has been observed in other large cohort studies and is often attributed to confounding by indication, wherein patients diagnosed with hypercholesterolaemia receive aggressive, long-term statin therapy, whose pleiotropic anti-inflammatory and plaque-stabilising effects confer a survival benefit that outweighs the risk of the diagnosis itself [14].
While prior studies have investigated preoperative risk profiles for patients undergoing cardiac surgery, most models pool males and females and apply a single coefficient for sex rather than deriving separate, sex-specific profiles. For instance, EuroSCORE II incorporates sex as a binary variable and assigns higher baseline risk to female patients [4]. Similarly, the Society of Thoracic Surgeons (STS)’ risk calculator treats sex dichotomously, attributing higher operative and postoperative mortality risk to females [15]. While these models acknowledge sex differences, they do not account for sex-specific variations in the prevalence, interactions, or effect sizes of individual predictors. The present findings demonstrate that several preoperative factors exert differential associations with one-year mortality in females versus males, underscoring a key limitation of existing models and supporting the development of sex-specific preoperative risk assessment that moves beyond a uniform “female penalty”.
4.1. Limitations
The study has important limitations. Its retrospective, single-centre design makes the findings descriptive and susceptible to selection bias and unmeasured confounding, reducing generalizability to other populations and health systems. Only preoperative variables were analysed, so intraoperative and postoperative factors that materially affect outcomes were not captured. Although surgical teams were largely consistent, advances in surgical technique, perioperative care, and technology over the 20-year period likely influenced mortality and complication rates. Exclusion of acute (urgent/emergent) cases further narrows applicability. Key confounders—socioeconomic status, medication adherence, and detailed frailty metrics—were unavailable, and the database lacked granular echocardiographic measures (notably left ventricular diastolic function and right ventricular function), which may partly account for the observed sex differences, especially in females. Given the known relevance in postoperative outcome in case of diastolic dysfunction and heart failure with preserved ejection fraction (HFpEF) particularly in females, this lack of detailed functional data may have led to residual confounding [16]. Finally, emphasising sex-specific rather than shared risk factors highlights disparities but may underrepresent an individual patient’s total risk burden.
4.2. Strengths
This study demonstrates several key strengths that support its validity and relevance. By including all patients undergoing cardiac surgery at a single tertiary care centre over a 20-year period, it provides a large, representative sample while reducing the risk of selection bias. Data collection was standardised, and thorough post-discharge review by the same surgeon (EKJ) throughout the study ensured consistency and accuracy. Mortality outcomes were confirmed using the Dutch database for registers of persons (Basisregistratie Personen) as of 1 November 2023, guaranteeing complete follow-up and minimising the risk of missing data. These careful procedures contributed to a robust dataset with very few errors or omissions.
4.3. Future Perspectives
Looking forward, these findings advocate for a shift toward more personalised, sex-aware perioperative risk assessment. Clinicians should be particularly vigilant for markers of systemic end-organ damage (pulmonary hypertension, extracardiac arteriopathy, kidney dysfunction) when evaluating female patients, as these may signal a higher-risk phenotype that is not fully captured by traditional cardiac-focused scores. Future research should focus on validating these sex-specific risk models in multicentre, external cohorts. Prospective studies are also warranted to investigate the underlying mechanisms of these distinct risk profiles, potentially incorporating biomarkers of inflammation, fibrosis, and detailed assessments of frailty and microvascular function. It is equally important to integrate sex-specific considerations into clinical decision-making and guideline development. Tailored preoperative assessment tools, targeted risk mitigation strategies, and heightened awareness of sex-related vulnerabilities may improve outcomes for both female and male patients. Moreover, incorporating sex-specific reporting standards, similar to the Sex and Gender Equity in Research (SAGER) guidelines in research, could enhance transparency and reproducibility, fostering a more nuanced understanding of how sex influences surgical risk and recovery in cardiac surgery.
5. Conclusions
In conclusion, our study demonstrates that one-year mortality following elective cardiac surgery is driven by distinct preoperative risk profiles in females and males. Recognising that mortality in females is associated with systemic disease and in males with direct cardiac damage is a critical step toward developing more equitable, precise, and effective perioperative management strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chang F.-C. Chen S.-W. Chan Y. Lin C.-P. Wu V.C.-C. Cheng Y.-T. Chen D.-Y. Hung K.-C. Chu P.-H. Chou A.-H. Sex differences in risks of in-hospital and late outcomes after cardiac surgery: A nationwide population-based cohort study BMJ Open 202212 e 05853810.1136/bmjopen-2021-05853835110325 PMC 8811586 · doi ↗ · pubmed ↗
- 2Johnston A. Mesana T.G. Lee D.S. Eddeen A.B. Sun L.Y. Sex Differences in Long-Term Survival After Major Cardiac Surgery: A Population-Based Cohort Study J. Am. Heart Assoc.20198 e 01326010.1161/JAHA.119.01326031438770 PMC 6755832 · doi ↗ · pubmed ↗
- 3Bradley S. White R.S. Jiang S.Y. Ma X. Hoyler M.M. Muehlschlegel J.D. Karamnov S. Tangel V.E. Lanahan J. Rong L.Q. Sex Differences in In-Hospital Mortality After Open Cardiac Valve Surgery Anesth. Analg.202213594495310.1213/ANE.000000000000607636029223 PMC 9588500 · doi ↗ · pubmed ↗
- 4Nashef S.A. Roques F. Sharples L.D. Nilsson J. Smith C. Goldstone A.R. Lockowandt U. Euro SCORE II Eur. J. Cardiothorac. Surg.201241734–744; discussion 44–4510.1093/ejcts/ezs 04322378855 · doi ↗ · pubmed ↗
- 5Afilalo J. Steele R. Manning W.J. Khabbaz K.R. Rudski L.G. Langlois Y. Morin J.-F. Picard M.H. Derivation and Validation of Prognosis-Based Age Cutoffs to Define Elderly in Cardiac Surgery Circ. Cardiovasc. Qual. Outcomes 2016942443110.1161/CIRCOUTCOMES.115.00240927407052 · doi ↗ · pubmed ↗
- 6Bianco V. Kilic A. Gleason T.G. Aranda-Michel E. Habertheuer A. Wang Y. Navid F. Kacin A. Sultan I. Reoperative Cardiac Surgery Is a Risk Factor for Long-Term Mortality Ann. Thorac. Surg.20201101235124210.1016/j.athoracsur.2020.02.02832199823 · doi ↗ · pubmed ↗
- 7Association W.M. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Participants JAMA 2025333717410.1001/jama.2024.2197239425955 · doi ↗ · pubmed ↗
- 8Von Elm E. Altman D.G. Egger M. Pocock S.J. Gotzsche P.C. Vandenbroucke J.P. Strobe Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies J. Clin. Epidemiol.20086134434910.1016/j.jclinepi.2007.11.00818313558 · doi ↗ · pubmed ↗