Tips and Pitfalls of Surgical Techniques for Scoliotic Deformities in Neurofibromatosis Type 1
Angelos Kaspiris, Ioanna Lianou, Vasileios Marouglianis, Roberta-Spyridoula Afrati, Evangelos Sakellariou, Andreas Morakis, Panagiotis Karampinas, Elias S. Vasilisadis, Spiros G. Pneumaticos

TL;DR
This review discusses surgical techniques and challenges for treating scoliosis in Neurofibromatosis Type 1 patients, highlighting recent advances and effective methods.
Contribution
The paper provides updated insights into surgical strategies and guidance methods for managing dystrophic scoliosis in Neurofibromatosis Type 1.
Findings
Posterior-only methods show encouraging results by avoiding plexiform tumours.
Growing rod systems help preserve spinal growth in early-onset cases.
O-arm and t-EMG improve pedicle screw placement accuracy.
Abstract
Background: Neurofibromatosis 1 is an autosomal dominant disorder accompanied by extensive early-onset spinal manifestations, with or without dystrophic scoliotic features. While non-dystrophic subtypes can often be treated similarly to idiopathic scoliosis, dystrophic scoliosis typically requires more aggressive intervention, often involving instrumentation in severely compromised pedicles or vertebrae. Purpose: This review aims to present recent advances in the surgical treatment of Neurofibromatosis 1-associated scoliosis, including surgical techniques and emerging guidance methods. Methods: An electronic literature search was conducted in Web of Science and PubMed to identify surgical techniques for scoliosis in patients with Neurofibromatosis 1. Results: Forty-one studies on the operative treatment of dystrophic scoliosis or both subtypes were retrieved. Although aggressive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
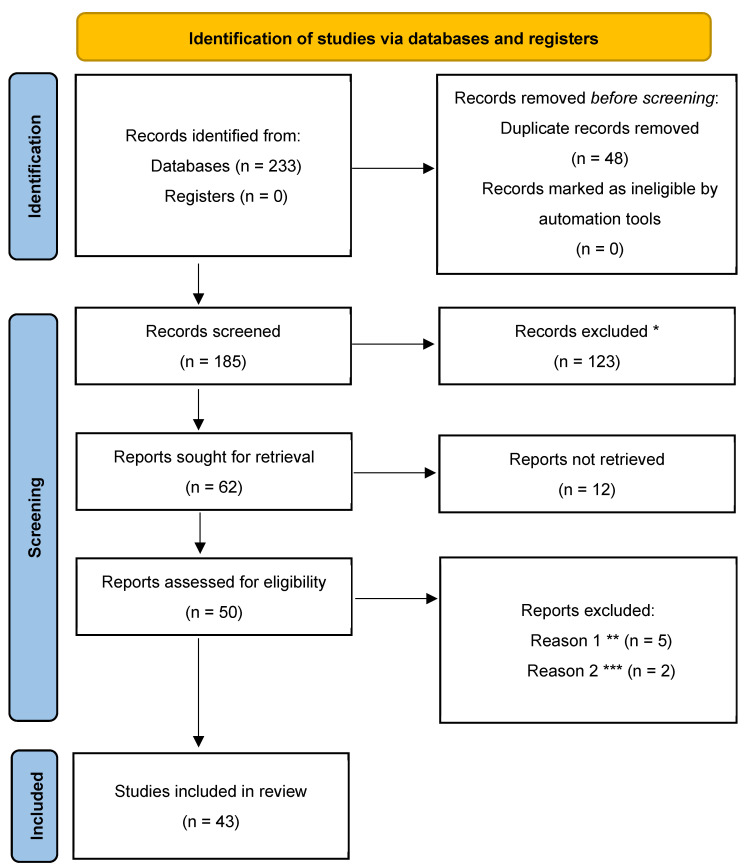 Figure 1
Figure 1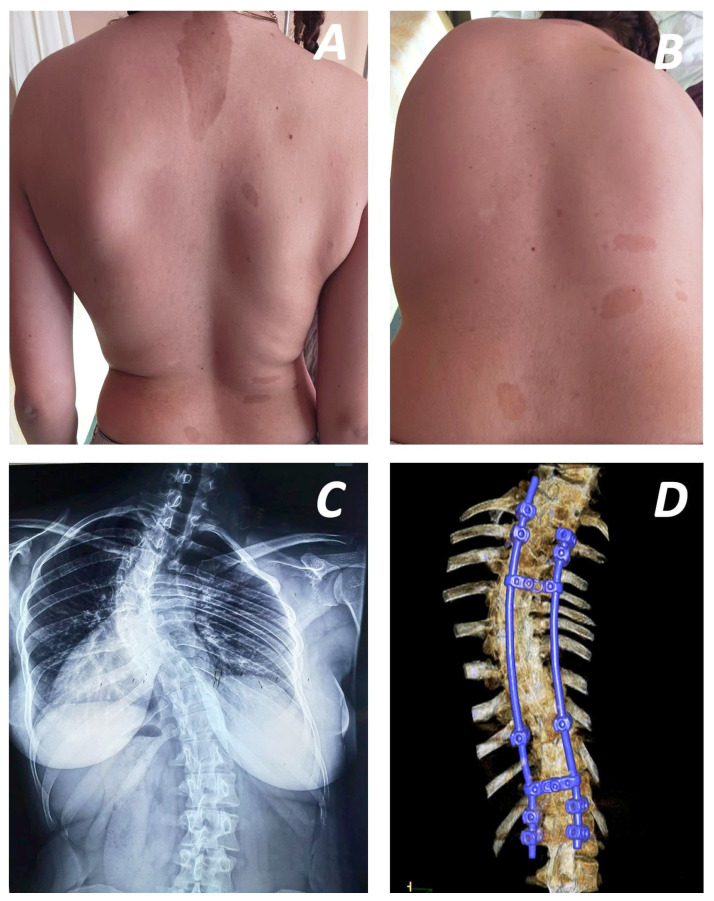 Figure 2
Figure 2 Figure 3
Figure 3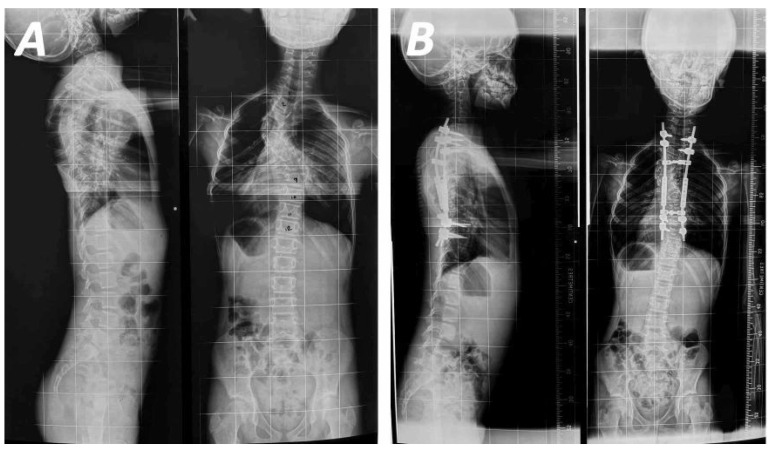 Figure 4
Figure 4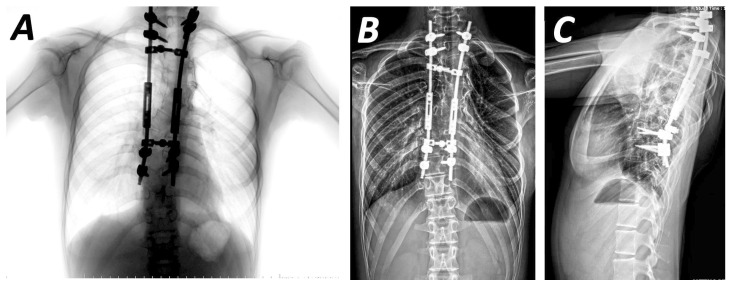 Figure 5
Figure 5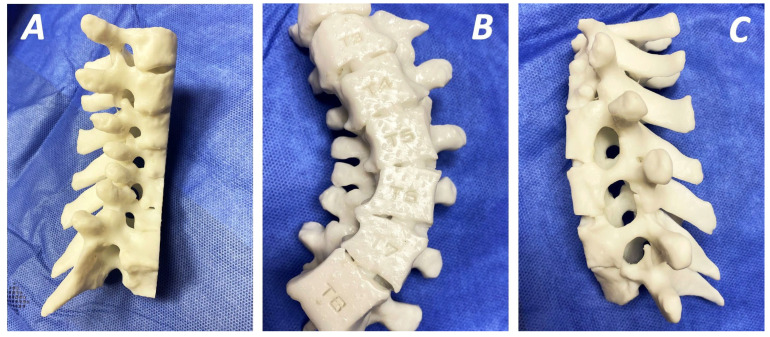 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Scoliosis diagnosis and treatment · Intraoperative Neuromonitoring and Anesthetic Effects
1. Introduction
Neurofibromatosis is classified into two subtypes: Neurofibromatosis type 1 (NF1) or peripheral subtype, which affects the vestibular nerve, and Neurofibromatosis type 2 (NF 2), known as central neurofibromatosis [1]. NF1, first described in 1882 by von Recklinghausen, is an autosomal dominant disorder, caused by mutations in the NF1 gene located on chromosome 17q11.2 [2]. This mutation causes loss of function of the tumour suppressor gene NF1, which is expressed in a wide variety of cells. The NF1 gene encodes neurofibromin, a cytoplasmic protein that downregulates cellular proliferation, differentiation, and growth through inactivation of the Ras-GTPase protein and accumulation of cyclic adenosine monophosphate (cAMP). Aberrant activation of the Ras pathway leads to upregulation of Ras-Raf-MEK-ERK and cross-talk with the phosphatidylinositol-3-kinase (PI3K) pathway [3,4]. Given the extensive expression of NF1 in various cell types, the disease exhibits heterogeneous penetrance and unpredictable manifestations (Figure 1) in different systems [5]. Its estimated incidence is approximately 1 in 2500 to 3000 individuals, who typically present with a variety of clinical manifestations including nerve-related complications such as non-malignant cutaneous or plexiform neurofibromas, freckles and café-au-lait spots (Figure 2A), optic gliomas, various skeletal disorders, most notably, spinal deformities (Figure 2B), and even malignant peripheral nerve sheath tumours in some cases [2,6].
Spinal deformity is the most common osseous manifestation of NF1, occurring in approximately 10–60% of affected individuals [7]. NF1-related scoliosis (Figure 2C) accounts for approximately 3% of all scoliosis cases [8]. The deformity is typically classified as either dystrophic or non-dystrophic, based on the presence of characteristic osseous dystrophic features. Dystrophic scoliosis is defined by the presence of vertebral dysplasia, commonly presenting with dural ectasia, paravertebral neurofibromas, vertebral scalloping, and rib pencilling, among other features. Non-dystrophic curves generally follow a more benign course and share similarities with idiopathic scoliosis. In contrast, dystrophic scoliosis presents at an earlier age and tends to be more aggressive. This type of scoliosis consists of a short-segmented curvature with sharp angulation and wedged vertebrae, intraspinal or paraspinal soft tissue masses accompanied by severe rotation of the vertebral column and an enlarged intervertebral foramen [9]. Additional findings may include rib dislocation, the “pencil sign”, and, in rare cases, rib head protrusion into the spinal canal—a complication documented in only 22 cases in the literature [1].
The presence of intraspinal ribs can be identified through MRI (Magnetic Resonance Imaging) and CT (Computed Tomography) scanning, although most patients are asymptomatic. However, cases of spinal cord compression with concomitant hemiplegia and paraplegia have been reported in the context of pre- or postoperative complications [10]. Conservative treatment with bracing is typically ineffective, and the severity of these deformities often necessitates early and usually aggressive surgical intervention [6]. Treatment strategies have traditionally focused on spinal fusion interventions with pedicle screw or hook instrumentation via posterior or anterior approaches. However, early-onset spinal deformities necessitate growth-friendly procedures, such as the use of growing rods, which allow more normal truncal and chest growth [11].
The aim of this review is to present the most recent updates on tips and pitfalls in the surgical management of scoliotic deformities associated with NF1, with a focus on both dystrophic and non-dystrophic subtypes. A range of instrumentation methods, surgical approaches, preoperative planning tools and intraoperative guidance systems are analysed, reflecting the complexity inherent in surgical management for patients with NF1. To our knowledge, this the first comprehensive literature review addressing surgical techniques and instrumentation employed in the treatment of NF1-related scoliosis.
2. Materials and Methods
2.1. Systematic Literature Review
A computer-based literature review was conducted on 10 July 2025 in accordance with the latest PRISMA (Preferred Reporting Items for Systematic Reviews Meta-Analyses) guidelines (Supplementary Materials). The results were presented in a PRISMA flow chart (Figure 1). The databases searched were PubMed (1947 to present) and Web of Science (1900 to present). All studies were retrieved following a comprehensive search methodology using the combination of the terms and phrases “neurofibromatosis type 1 [All fields]”, “surgery [All fields]”, “scoliosis [All fields]” and “spinal deformities [All fields]”.
The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251107808 with full public access available.
2.2. Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (a) full texts only, (b) original articles, (c) case reports or case series, (d) comparative studies regarding the use of different methods of treatment of both dystrophic and non-dystrophic subtypes of NF1-associated scoliosis, (e) studies focusing on all instrumentation methods, surgical approaches, treatment options (fusion procedure or growth-friendly methods), preoperative planning or intraoperative imaging tools. No restrictions were applied regarding patient age or publication date.
Exclusion criteria were as follows: (a) laboratory studies or studies based on in vitro or in vivo models, (b) letters to the editor, editorials, technical notes, book chapters, and expert opinions, (c) studies without sufficient data regarding the exact type of spinal deformity in patients with confirmed diagnosis of NF1, with insufficient data regarding the neurofibromatosis subtype and the exact type of surgical intervention, (d) studies incorporating population with kyphotic, or population with mixed features; kyphosis and kyphoscoliosis, (e) studies in languages other than English.
According to Lykissas et al. and Duranni et al., scoliotic deformity is characterised as dystrophic when three of the following criteria are present: (a) depth of vertebral scalloping greater than 3 and 4 mm in the thoracic and lumbar spine, respectively, (b) pencilling of rib, (c) transverse processes spindling, (d) rotation of vertebrae (grade 3 or more, according to the Moe–Nash method), (e) short segmented curvature (six or fewer vertebrae), (f) paraspinal tumours or plexiform neurofibromas, (g) dural ectasia, (h) wedged vertebrae, (i) dysplasia of the pedicles, (j) widening of the interpediculate distances, and (k) widening of the intervertebral foramina [12,13]. All studies were further categorised accordingly and the subtypes of the deformity included was stated (Table 1).
2.3. Data Extraction and Quality Assessment
The literature search and data extraction were independently performed by two reviewers and a librarian. Based on the inclusion and exclusion criteria, titles and abstracts from relevant articles were screened and eligible data were recorded in a Microsoft Excel spreadsheet (Microsoft Office 365, Redmond, WA, USA). Disagreements regarding study inclusion or data extraction were resolved by the senior author. This study was conducted according to the principles of systematic reviews.
2.4. Evaluation of Study Quality
The methodology of the selected studies was independently evaluated using the Newcastle–Ottawa quality assessment scale. With the exception of review articles, studies were categorised into three quality levels: scores of 0–3 were classified as poor, scores of 4–6 as fair, and scores of 7–9 as good.
3. Results
A total of 43 studies concerning the surgical management of scoliosis in patients diagnosed with NF1 were retrieved. These are presented in two tables. Table 1 presents articles evaluating various surgical treatment methods (either spinal fusion or growth-friendly methods) or studies on preoperative or perioperative correction techniques, including use of preoperative halo-gravity traction [11,14,15,16,17,19,20,21,22,24,25,27,28,30,31,32,33,34,35,36,37,38,40,42,44,49,50,51,52]. Among these, four are review articles and four are case series. Three studies analyse outcomes of correction on non-dystrophic cases (combined or not with dystrophic) [14,17,26]. The intraoperative guidance methods are presented in Table 2, while the use of growth-friendly systems is presented in 13 studies (Table 3); with one them focusing on the role of magnetically controlled growing rods [11,23,25,28,30,31,35,37,42,43,50].
Table 2 presents results from four studies focusing on the use of intraoperative assistance methods, including navigation and monitoring techniques [53,54,55,56]. Two of these studies are comparative analyses evaluating the use of O-arm navigation versus the free-hand technique for pedicle screw insertion [53,54]. Outcomes related with on the use of intraoperative neurophysiological monitoring are further analysed by Qiu et al., while results from surgical interventions assisted by the combined use of O-arm navigation and triggered electromyography (t-EMG) have also been reported [55,56].
Various postoperative complications related with the treatment of NF1 scoliosis have been reported. According to Neifert et al., the incidence of immediate postoperative complications is estimated at 2.1%, with 1.5% resulting in permanent deficits. Revision surgery was deemed necessary in 21.5% of all cases [42]. In contrast, Cai et al. reported no neurological or respiratory complications, although their study involved a smaller sample size and employed screw-based instrumentation [23,33]. Similar results were observed in patients treated with growth-friendly procedures [31]. However, several complications (mainly rod breakage) related with growth-friendly methods were presented by Carbone et al. [11]. Finally, no revision surgeries were required among sixteen patients with NF1 scoliosis who underwent single-stage posterior pedicle screw fixation, as reported by Wang et al. [21].
Correction of curvature varies among the studies retrieved. In non-dystrophic cases, curvature correction was estimated at 62.9%, whereas correction rates in dystrophic cases differed depending on curve location—thoracic versus combined thoracolumbar and lumbar curves [14]. In cases managed with growing rods until definitive fusion, the correction rate at final follow up was 50.1%, while T1-S1 (thoracic 1-sacral 1) growth was estimated at approximately 11.2 mm per year [25]. For cases treated with screw-based instrumentation, major curve angles improved from a preoperative mean of 66.1° ± 16.2° to 31.1° ± 14.6° postoperatively [32]. Similarly, Mladenov et al. reported a mean curvature correction of 54%, while annual thoracic growth appeared to be preserved [35].
4. Discussion
4.1. Treatment of Non-Dystrophic Scoliosis
The presence or absence of bone dystrophic features in patients with NF1 scoliotic deformities classifies the curvature as either dystrophic or non-dystrophic, respectively. Although non-dystrophic scoliosis often resembles idiopathic scoliosis, these curves may still demonstrate progression over time and, in some cases, evolve into dystrophic patterns, which usually necessitate surgical treatment. According to current literature, relatively few studies specifically address the outcomes of surgical treatment for non-dystrophic scoliosis in the NF1 population. The largest study to date was conducted by Lyu et al., who compared outcomes of single-stage, posterior-only pedicle screw instrumentation between patients with NF1-associated non-dystrophic scoliosis and those with adolescent idiopathic scoliosis. Comparable postoperative clinical outcomes and complication rates in both groups supported the efficacy of this surgical approach, even in patients with differing spinal flexibility. Nevertheless, anatomical challenges such as thin pedicles or dural ectasia in patients with non-dystrophic NF1 scoliosis may complicate pedicle screw placement [26].
Li et al. [17] reported three cases of non-dystrophic NF1 scoliosis treated with posterior instrumented fusion, while Halmai et al. [14] described one additional case. In Halmai’s case, a 16-year-old patient underwent posterior fusion for a non-dystrophic curve, achieving a 69.2% correction, with no pseudarthrosis [14]. No pseudarthrosis was noted and correction loss was 5° in the frontal plane and 4° in the sagittal, upon achieving final fusion. Similarly, mean postoperative coronal curve correction in non-dystrophic patients was 61.3%, with 3° correction loss in the sagittal plane and 6° in the frontal, as estimated during follow-up, respectively [17]. One of these cases involved a curve exceeding 90°, yet effective correction (60%) was achieved. This success was attributed to good preoperative bending flexibility and the use of halo vest and Cotrel gravity traction, which facilitated soft tissue relaxation. Ultimately, this patient was managed successfully with posterior-only fusion.
4.2. Treatment of Dystrophic Scoliosis
4.2.1. Spinal Fusion Techniques
Spinal fusion achieved with bone grafts or instrumentation (anterior and posterior approaches) was described in 24 studies [17,18,19,21,22,23,24,26,28,29,31,32,33,35,36,37,38,42,44,45,51,57]. No consensus regarding the type or time of intervention has been established. However, due to the progressive nature of NF1-associated deformities, early treatment, which involves early definitive fusion or growing rod methods, is required. Early fusion is usually performed in patients with short and sharp curves or patients over 10 years old with long curves [28]. A posterior-only approach has been suggested for less severe deformities [15]. Outcomes on the use of this approach have been reported by various studies. Wang et al. used a single-stage pedicle screw instrument system, achieving satisfactory coronal and sagittal balance, without requiring revision surgery (Figure 2D). However, global spinal balance remained an area for improvement (Figure 3A,B) [21]. Similarly, the use of multiple anchor point systems (third-generation instrumentation systems) in posterior-only fusion procedures resulted in significant correction of the mean coronal Cobb angle (58.7%) and apical vertebral rotation, with only 2.3% loss of Cobb angle correction at final follow-up [24]. These systems enhance correction stabilisation, avoiding extended correction attempts and concomitant neurological complications. The impact of implant density in the posterior surgical approach has been evaluated in relation to immediate postoperative coronal correction and loss of correction at follow-up. Both parameters presented statistically significant improvement in short-term follow-up when a higher level of implant insertion was used [54]. However, research assessing mid- and long-term outcomes of posterior-only fusion have reported that, despite good initial coronal curve correction, a higher rate of correction loss and alignment complications may occur over time. The incidence of neurological complications was lower, and when short fusion segments were selected, lung function was generally preserved [31].
A two-stage procedure, combining ring anterior release and fusion followed by posterior correction and fusion, was carried out in 32 patients with severe rigid deformities, who were treated with multisegmental instrumentation systems [18]. No implant failure and only two cases of pseudarthrosis were described, while correction rate and loss of correction were greater in large kyphotic curves, consistent with recent literature findings [17,18,58]. Various instrumentation systems have been used in dual-approach procedures, including hooks, pedicle screws, all-hook systems, or hybrids. Comparative studies evaluating pedicle screws versus hybrid systems revealed no statistically significant differences in coronal or sagittal correction rates or in loss of sagittal alignment. However, a statistically significant difference in coronal correction loss was observed at long-term follow-up, with less correction loss at 9.5 years postoperatively in patients treated with pedicle screw instrumentation [27]. Long-term results in a cohort of 11 patients who underwent anteroposterior fusion for dystrophic curves, with subtotal tumour resection of the concave area in seven of them, demonstrated a trend toward shorter final height compared to the general population and progression of the deformity in all cases [36]. Finally, the inclusion of neutral and stable vertebrae (in both the coronal and sagittal planes) and coronal curves exceeding 40° in long segmental posterior-only fusion yielded similar results with combined anterior and posterior approaches in patients with NF1 and scoliotic curves between 40° and 90° [17]. Both the correction rate and postoperative correction loss was comparable with results from current literature. However, the study highlights the need for dual fusion procedures in patients younger than 10 years, as this population may suffer from the crankshaft phenomenon when treated with posterior-only fusion [13].
4.2.2. Growth-Friendly Methods
Clinical outcomes following use of growth-friendly methods (Figure 4A,B) have been discussed in 13 studies (Table 3) [11,23,25,28,30,33,35,37,39,42,43,47,50]. These methods have demonstrated acceptable correction with maintenance of trunk growth (Figure 5A–C). The first study, focusing exclusively on a cohort with NF1-associated scoliosis, reported similar correction rates and T1-S1 growth with other studies on the use of growing rods for early-onset scoliosis [25]. Moreover, a significant complication of this technique was proximal junctional kyphosis, attributed to low bone mineral density and dystrophic changes in patients with NF1 scoliosis, leading to poor fixation points. According to Carbone et al., Cobb angle correction improved by up to 43.4% at last follow-up, with concurrent improvement in coronal balance [11]. The best results were observed immediately after lengthening procedures, performed annually. The decrease in lengthening gain, commonly referred to as the “law of diminishing returns”, typically observed after each lengthening procedure, was not confirmed in this case, where lengthening was performed annually, in contrast to other studies. The combined use of a dual growing rod system and preoperative halo-gravity traction has been shown to facilitate the treatment of rigid deformities, achieving a Cobb angle correction of approximately 41.6% after halo-gravity traction and 53.3% at final follow-up and, without neurological disorders or autofusion [30]. Finally, only a few studies have assessed the use of magnetically controlled growing rods (MCGR) for the treatment of NF1-associated scoliosis. Although this system has demonstrated improvements in major curve correction and spinal height, its application is limited by reduced imaging visibility, particularly in patients with intraspinal tumours [47].
Tauchi et al. were the first to compare surgical results between early fusion methods (posterior-only and combined approach) versus growth-friendly methods [37]. Greater curvature correction with fewer surgical interventions was achieved in the population treated with early fusion. However, although growth-friendly methods achieved better spine and thorax growth, the final absolute height showed no statistically significant difference. Similarly, complication rates did not differ significantly. However, growth-friendly methods were associated with a higher incidence of complications and lower curve correction, as compared to fusion methods [37].
4.2.3. Preoperative Planning—Three-Dimensional Printing Technology
Treatment of spinal deformities in dystrophic NF1 remains a challenge, as the complex morphology of pedicles may affect the identification of insertion points for screw placement. Therefore, defective manual insertion of the screws may result in neurological side effects and damage to vascular tissues or vital organs [59]. Furthermore, the vertebral pedicles in these patients can be narrowed, hypoplastic (concave site) or even absent, being accompanied by vertebral body rotation, which directly affects surgical outcomes, leading to pedicle root fractures and nerve root or spinal cord injuries [60].
The use of three-dimensional printing (3DP) templates for navigation (Figure 6) in these types of scoliosis correction surgeries assist in optimising preoperative planning as they enhance the accuracy of screw placement and shorten surgical time and blood loss [60]. Furthermore, 3DP navigation systems optimise the surgeons’ learning curve, as they can be used for better understanding of anatomical structures, or even surgical rehearsal [61]. Especially, in cases with a Cobb angle greater than 50°, their application as accurate templating systems results in optimised intraoperative approaches, less radiation, fewer complications, and a decreased rate of revision surgeries in paediatric patients [62]. Furthermore, the combination of 3DP and pedicle guider, which is based on a drill template, can aid in precise screw placement and limited surgical time [63]. Finally, a five-point navigation template using a point-contact system has been demonstrated to reduce blood loss and prevent stripping of the posterior structures, while its segmented design helps to mitigate incompatibility issues arising from changes in body positioning [60].
4.2.4. Intraoperative Assistant Methods
Several intraoperative guidance systems, including O-arm navigation and intraoperative neurophysiological monitoring, have been shown to assist in more accurate pedicle screw insertion and higher implant density. According to Li et al., increased implant density leads to higher coronal correction rate (immediate) with lower correction loss and better clinical scores [54]. This implant density, reflecting safer and more accurate pedicle screw insertion in severe deformities, was achieved with the use of the O-arm. Similarly, higher implant density, better curvature correction with lower incidence of median screw perforation was feasible with the guidance of O-arm navigation, when compared to a free-hand technique [53]. Use of intraoperative neurophysiological monitoring can be safely applied even in patients with preoperative dystrophic features. However, the presence of preoperative dystrophy and neurologic deficits can lead to higher rates of failed intraoperative neurophysiological monitoring. The overall success rate of somatosensory evoked potentials and motor evoked potentials is estimated approximately 87% and 94.6%, respectively [55]. Careful assessment of preoperative neurological status assists in safer monitoring and, consequently, safer and more accurate surgical intervention. Finally, the combination of methods (t-EMG with O-arm-assisted pedicle screw placement) used in treatment of NF1 scoliosis has already been studied and appears to present 100% sensitivity, 66.7% positive predictive value, and 96.2% specificity [56].
4.2.5. Post-Operative Management
Surgical interventions for the treatment of spinal deformities in patients with NF1 have already been analysed and remain the standard of care in dystrophic cases. However, it seems critical to evaluate the clinical characteristics and special needs of these patients in order to optimise their final interventional outcomes by reducing the rate of pseudarthrosis and revision surgeries. According to the literature, postoperative pseudarthrosis presents in approximately 25% of all cases and a clinically robust fusion is noted in as few as 7% of them [64]. Taking these data into account, many studies investigated the impact of several pharmacological agents on the postoperative outcomes of NF1 spinal deformities, reporting promising results. In specific, Mitogen-activated protein kinase (MEK) inhibitors presented increased activity in the reduction in spinal neurofibroma burden, or bone healing and successful spinal fusion [65]. Biphosphonates, asfotase alfa, and bone morphogenic proteins have contributed to solid spinal arthrodesis, when they are used as supplementary therapy with deformities related with NF1 in vivo [66]. Moreover, the administration of asfotase alfa and bisphosphonates in combination with surgical intervention and rhBMP-2 (recombinant human Bone Morphogenetic Protein-2) resulted in solid arthrodesis and enhanced bone healing in a patient with NF1-related dystrophic scoliosis, suggesting that enhanced bone formation, resorption, and mineralisation may be associated with better outcomes [67]. Good clinical results related with the use of off-label BMPs and bisphosphonates in clinical case series with tibial pseudarthrosis could support their use for better outcomes regarding fusion, especially in cases of such surgeries [67,68]. Although their application needs further study, measurements of bone mineral density (BMD) in cases of NF1 scoliosis may also assist in the final treatment strategy by the evaluation of serum biomarkers, vitamin D, and bone turnover when combined with biomechanical finite 3D element modelling of both the concave and the convex area of vertebral bodies [64,65]. The use of this tool can provide a future theoretical background for the improvement of surgical spinal fixation devices and the analysis of specific of scoliotic deformities.
4.3. Strengths and Limitations
To our knowledge, this the most recent review to focus exclusively on the operative treatment of NF1-associated scoliosis. In addition to evaluating surgical methods and instrumentation, this review includes analysis of intraoperative navigation techniques.
However, our study has several limitations. Considering the inclusion criteria, which cover only NF1-associated scoliosis, most of the studies reviewed include relatively small sample sizes, which limits both comparability and the predictive value of the findings. Furthermore, the inclusion of only English-language publications introduces the risk of language bias.
5. Conclusions
Dystrophic features and a tendency for rapid progression make NF1-associated scoliosis a significant surgical challenge. No consensus on a specific treatment has been achieved so far. Although no clear genotype–phenotype correlation has been established in patients with NF1-associated scoliosis [43], additional studies regarding this may facilitate the development of personalised and widely accepted surgical management strategies for this rare disease. Further investigation into preoperative radiological examination, informed by current findings, and intraoperative guidance [40], can contribute to more accurate instrument insertion, reduce intraoperative and postoperative complications, and lead to improved clinical scores.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delucia T.A. Yohay K. Widmann R.F. Orthopaedic Aspects of Neurofibromatosis: Update Curr. Opin. Pediatr.201123465210.1097/MOP.0b 013e 32834230 ce 21150444 · doi ↗ · pubmed ↗
- 2Barxer D. Wright E. Nguyen K. Cannon L. Fain P. Goldgar D. Bishop D.T. Carey J. Baty B. Kivlin J. Gene for von Recklinghausen Neurofibromatosis Is in the Pericentromeric Region of Chromosome Science 19872361100110210.1126/science.31071303107130 · doi ↗ · pubmed ↗
- 3Krygowska A.A. Castellano E. PI 3K: A Crucial Piece in the RAS Signaling Puzzle Cold Spring Harb. Perspect. Med.20188 a 03145010.1101/cshperspect.a 03145028847905 PMC 5983164 · doi ↗ · pubmed ↗
- 4Kaspiris A. Savvidou O.D. Vasiliadis E.S. Hadjimichael A.C. Melissaridou D. Iliopoulou-Kosmadaki S. Iliopoulos I.D. Papadimitriou E. Chronopoulos E. Current Aspects on the Pathophysiology of Bone Metabolic Defects during Progression of Scoliosis in Neurofibromatosis Type 1J. Clin. Med.20221144410.3390/jcm 1102044435054138 PMC 8781800 · doi ↗ · pubmed ↗
- 5Young H. Hyman S. North K. Neurofibromatosis 1: Clinical Review and Exceptions to the Rules J. Child Neurol.20021761362110.1177/08830738020170081212403560 · doi ↗ · pubmed ↗
- 6Jett K. Friedman J.M. Clinical and Genetic Aspects of Neurofibromatosis 1Genet. Med.20101211110.1097/GIM.0b 013e 3181 bf 15e 320027112 · doi ↗ · pubmed ↗
- 7Akbarnia B. Gabriel K. Beckmann E. Chalk D. Prevalence of Scoliosis in Neurofibromatosis Spine 19921724424810.1097/00007632-199208001-000051523507 · doi ↗ · pubmed ↗
- 8Gutmann D.H. Ferner R.E. Listernick R.H. Korf B.R. Wolters P.L. Johnson K.J. Neurofibromatosis Type 1Nat. Publ. Gr.201731700410.1038/nrdp.2017.428230061 · doi ↗ · pubmed ↗