NGR1 Pretreatment Enhances the Therapeutic Efficacy of Transplanting Cardiomyocytes Derived from Human Induced Pluripotent Stem Cells for Myocardial Infarction
Hao Cai, Meng-Ying Huang, Fang-Fang Mou, Qiang-Li Wang, Zhi-Rong Luo, Ping-Ping Lu, Bao-Nian Liu, Liang Hu, Hai-Dong Guo

TL;DR
Pretreating heart cells with NGR1 improves their survival and effectiveness when transplanted into damaged heart tissue.
Contribution
NGR1 pretreatment enhances the therapeutic potential of hiPSC-derived cardiomyocytes for myocardial infarction.
Findings
NGR1 pretreatment increases ejection fraction and fractional shortening in treated mice.
NGR1 reduces infarct size and collagen deposition while promoting angiogenesis and lymphangiogenesis.
NGR1-treated cells show higher survival and reduced apoptosis in the heart tissue.
Abstract
Human induced pluripotent stem cells (hiPSCs) offer significant potential for differentiation and research applications in cardiovascular diseases. When induced differentiated hiPSC-derived cardiomyocytes (hiPSC-CMs) are transplanted into the infarcted myocardial region, they exhibit extremely low survival rates and unsatisfactory therapeutic effects due to ischemia, hypoxia, and immune inflammation in the surrounding environment. To address this issue, we used Panax notoginseng saponin R1 (NGR1), which has demonstrated significant protective effects in prior research, to pretreat hiPSC-CMs before transplantation. Utilizing an in vitro H2O2 oxidative stress model and a nude mouse myocardial infarction (MI) model, we investigated the mechanism through which NGR1 pretreatment enhances the therapeutic efficacy of hiPSC-CM transplantation. The results revealed that the hiPSC-CMs expressed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
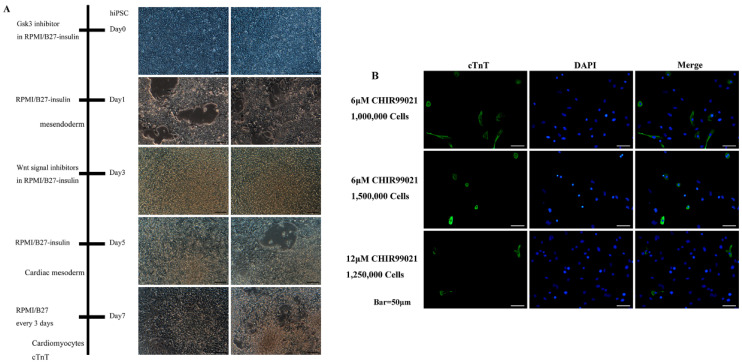 Figure 1
Figure 1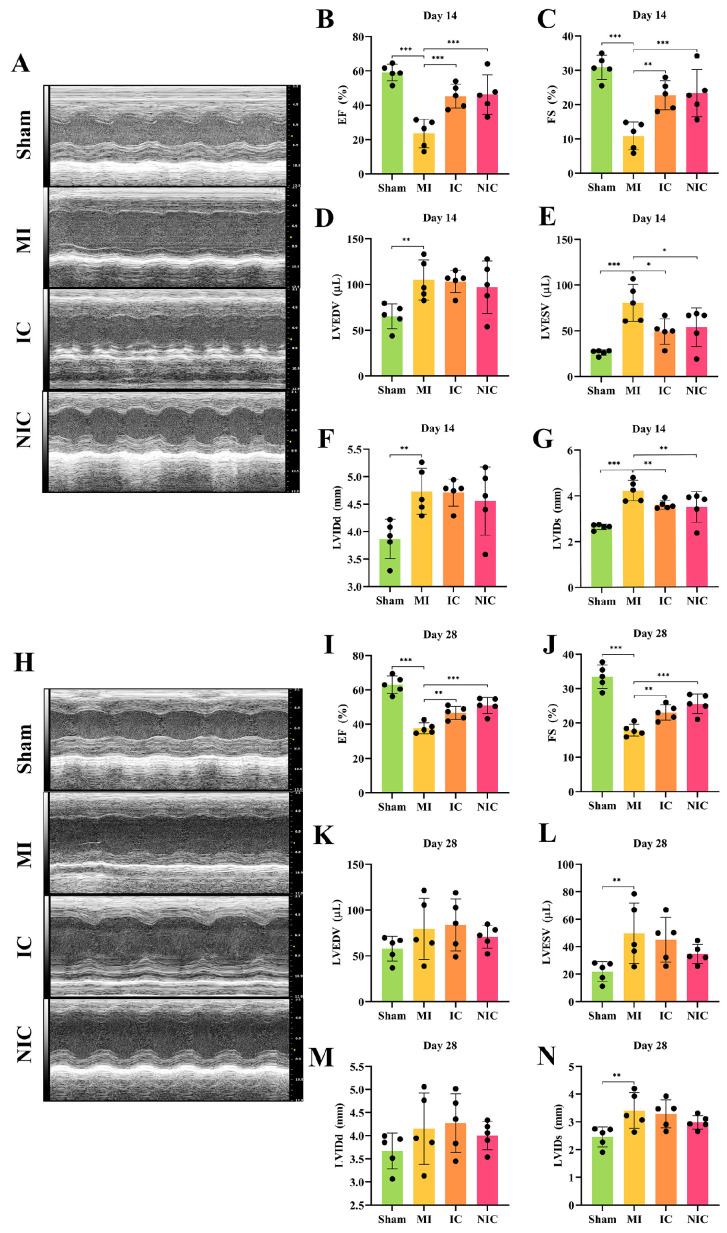 Figure 2
Figure 2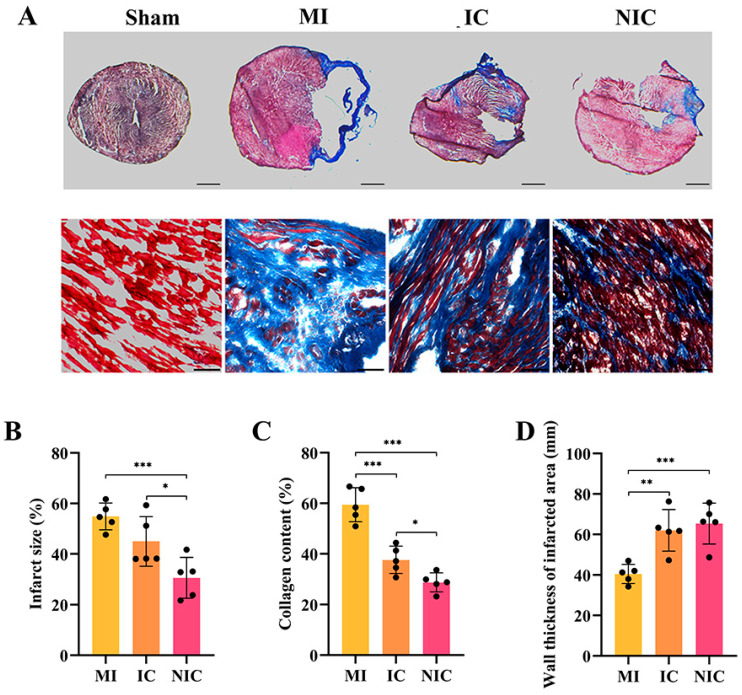 Figure 3
Figure 3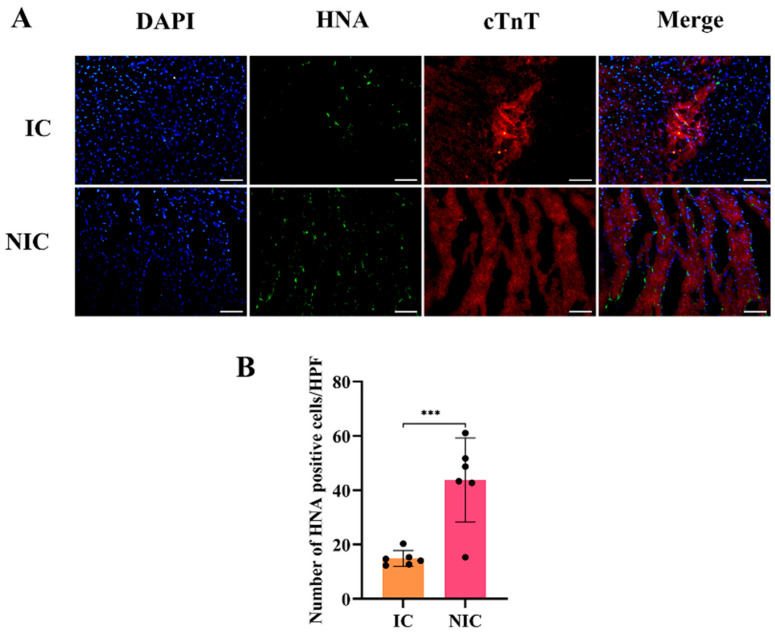 Figure 4
Figure 4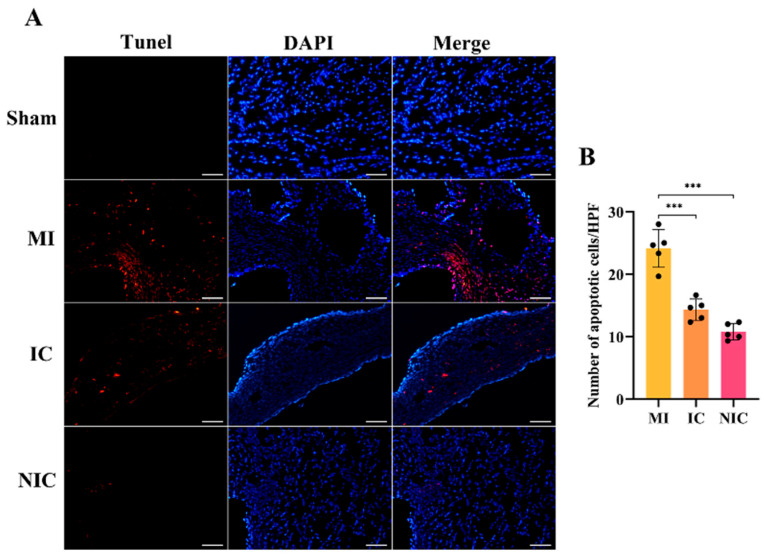 Figure 5
Figure 5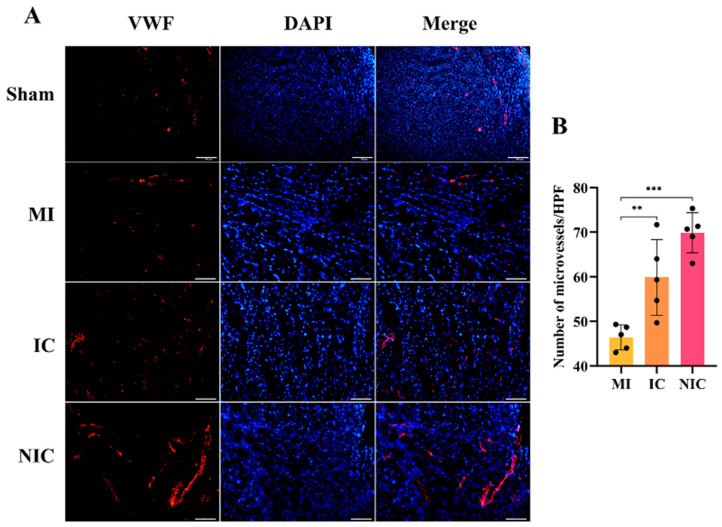 Figure 6
Figure 6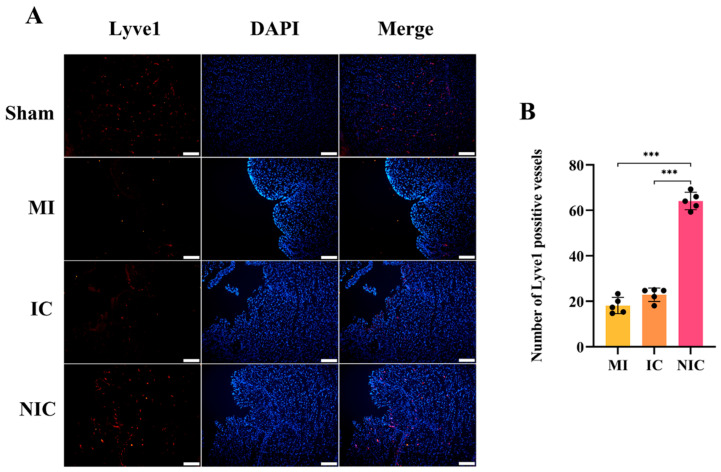 Figure 7
Figure 7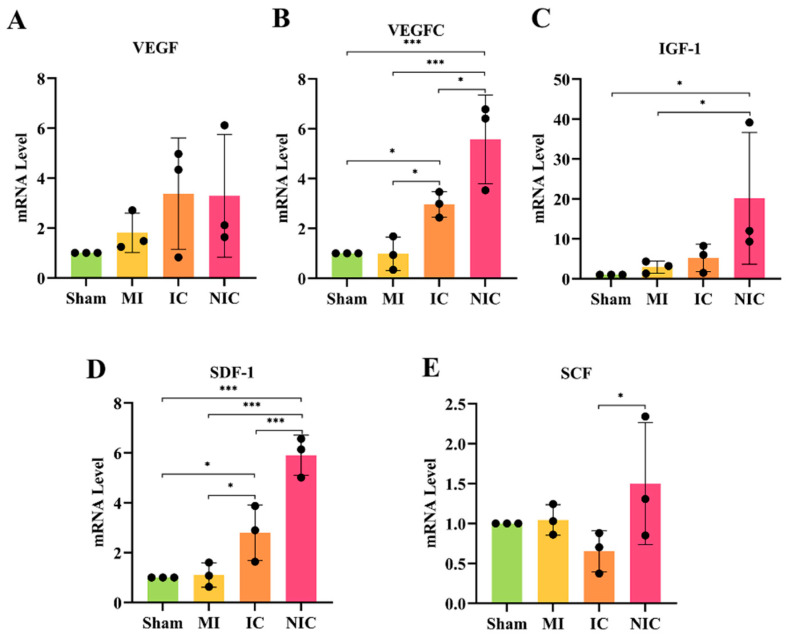 Figure 8
Figure 8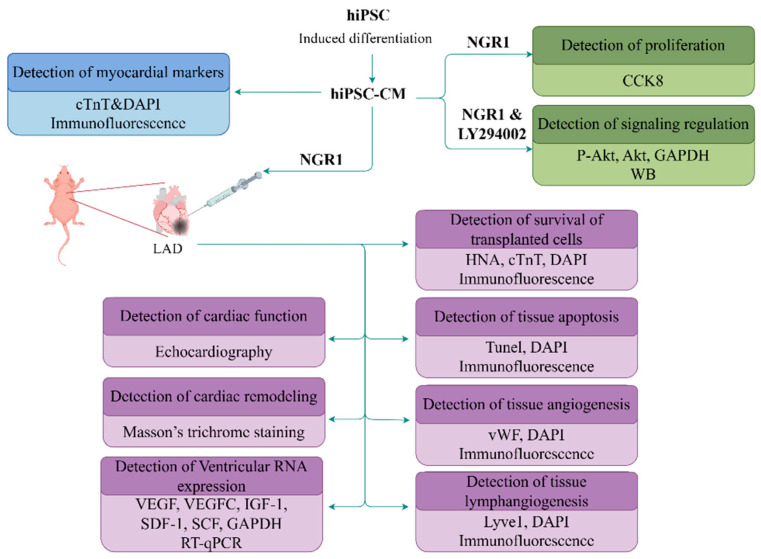 Figure 9
Figure 9- —National Natural Science Foundations of China
- —Traditional Chinese Medicine Research Project of Shanghai Municipal Health Commission
- —Natural Science Foundation of Shanghai
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPluripotent Stem Cells Research · Tissue Engineering and Regenerative Medicine · Mesenchymal stem cell research
1. Introduction
Myocardial infarction (MI), as one of the leading causes of mortality worldwide, is a severe disease characterized by myocardial ischemic necrosis, resulting from coronary artery obstruction and severe, persistent ischemia in the myocardial region [1]. Clinical treatments typically involve intravenous thrombolysis, percutaneous coronary intervention (PCI), and other methods aimed at promptly restoring blood supply and minimizing damage. However, issues such as microvascular obstruction and dysfunction, distal embolism, and myocardial ischemia–reperfusion injury (MIRI) following intervention remain unresolved [2]. Furthermore, the irreversible necrosis of myocardial cells after MI leads to alterations in myocardial structure and function, subsequently triggering cardiac remodeling and heart failure.
In recent years, various fields have conducted extensive foundational research on treatments related to MI. Stem cells, including mesenchymal stem cells (MSCs) and human induced pluripotent stem cells (hiPSCs), have garnered significant attention due to their potential for myocardial repair [3]. Among these, hiPSCs stand out because of their ability to proliferate and differentiate in multiple directions, particularly into cardiomyocytes [4]. HiPSCs are sourced from a variety of tissues, which helps avoid ethical concerns and reduces the risk of immune rejection, making them highly valuable for both basic research and clinical applications [5]. When cultured in vitro, hiPSC-CMs typically form a population of rhythmically beating cells but lack the structure of actual cardiac tissue. The harsh environment in transplantation settings, however, limits their survival and functional integration [6]. As a result, improving the survival rate of transplanted hiPSC-CMs and enhancing their integration into cardiac tissue has become a key focus of current research [7].
Traditional pharmacological and interventional approaches struggle to reverse the aforementioned process of myocardial function deterioration after MI [8]. Traditional Chinese medicine and its bioactive compounds have demonstrated significant advances in the prevention and treatment of MI. Notably, NGR1, a principal active component of Panax ginseng, exhibits cardioprotective properties, including anti-inflammatory, antioxidant, and anti-apoptotic effects. Previous studies have indicated that NGR1 can markedly ameliorate MIRI, reduce cardiomyocyte apoptosis, and facilitate the recovery of cardiac function [9]. Its mechanisms involve modulation of multiple signaling pathways, such as activation of the Wnt/β-catenin and JAK2/STAT3 pathways, as well as inhibition of the TAK1-JNK/p38 signaling cascade, thereby regulating cardiomyocyte apoptosis and inflammatory responses [10]. Furthermore, combining NGR1 with other pharmacological agents or nanocarriers has been shown to enhance its cardioprotective efficacy [11]. In our prior work, we observed that NGR1 pretreatment augmented the therapeutic effect of MSC transplantation in MI [12]. In addition, we also found that MSC pretreated with salvianolic acid B improved cardiac function through angiogenesis and paracrine mechanisms after MI [13].
The present study aimed to evaluate whether NGR1 pretreatment could enhance the efficacy of hiPSC-CM transplantation for MI. Specifically, we investigated the effects of NGR1 pretreatment on hiPSC-CM survival and explored the underlying mechanisms, including promoting angiogenesis, lymphangiogenesis and paracrine secretion, with the goal of providing both theoretical and experimental foundations for its potential clinical application.
2. Results
2.1. Induction of hiPSC Differentiation and Detection of Myocardial Markers
Differentiation conditions were optimized by modulating cell density and inhibiting the GSK3 and Wnt signaling pathways. The results indicate that treatment with 6 μM CHIR99021 and seeding at a density of 1 × 10^6^ cells per well efficiently induced differentiation into cardiomyocytes. On the first day of induction, inhibition of signaling pathways led to partial cell death and a reduction in cell density. By the second day, cell density had increased, and by day five, it had stabilized. By day seven, cells exhibited morphology reminiscent of H9c2 cardiomyocytes, and they began spontaneous contractions within seven to ten days, which persisted for approximately one month (Figure 1A). Following differentiation into cardiomyocytes, the cells were transferred to confocal culture dishes and cultured for an additional two days. Immunofluorescence staining revealed robust expression of cTnT, with a substantial proportion of cells exhibiting positive fluorescence under confocal microscopy (Figure 1B).
2.2. Transplantation of hiPSC-CMs with NGR1 Pretreatment Improves Cardiac Function
Nude mice were administered hiPSC-CMs immediately after inducing MI by ligating the anterior descending branches of the left coronary artery. Echocardiograms taken at 2 and 4 weeks post-transplantation, as shown in Figure 2, revealed significant improvements in various cardiac function parameters. In comparison to the Sham group, the MI group exhibited significant increases in EF, FS, LVESV, and LVIDs (Figure 2B–N). In the IC group, EF and FS were notably improved at 2 weeks compared to the MI group, while LVEDV and LVIDd were higher than both the Sham and MI groups. Furthermore, LVESV and LVIDs were reduced in the IC group relative to the MI group. In the NIC group, both EF and FS were significantly enhanced compared to the MI group, with trends suggesting even better recovery than in the IC group. Additionally, the recovery of LVEDV, LVIDd, LVESV, and LVIDs in the NIC group was superior to that observed in the IC group (Figure 2B–G). LVESV and LVIDs in the IC and NIC groups were significantly lower than those in the MI group, indicating that hiPSC-CM injection effectively alleviated or delayed ventricular remodeling in the early stage of MI. While some compensatory ventricular dilation after MI or transient effects occurred following cell injection, at 4 weeks, cardiac function parameters, including EF and FS in the NIC group, were still significantly improved compared to the MI group, and the trend of recovery was more pronounced than that in the IC group (Figure 2I–N).
2.3. NGR1-Pretreated hiPSC-CM Transplantation Reduces Infarct Area and Collagen Deposition
Masson’s trichrome staining demonstrated that both hiPSC-CM transplantation and NGR1-pretreated hiPSC-CM transplantation reduced the infarct area and collagen deposition. The infarct area and collagen fiber deposition were notably lower in the NGR1-pretreated hiPSC-CM transplantation group compared to the model and IC groups (Figure 3A–C). Additionally, the thickness of the ventricular wall in the infarct zone was significantly reduced in the model group. However, both hiPSC-CM and NGR1-pretreated hiPSC-CM transplantation promoted increases in the ventricular wall thickness (Figure 3D).
2.4. NGR1 Pretreatment Enhances Survival of Transplanted hiPSC-CMs
As the transplanted cells were human-derived, their survival and engraftment were determined through immunofluorescence staining of human nuclear antigen (HNA). HNA and cTnT staining indicated that the survival rate of the transplanted hiPSC-CMs in the NIC group was significantly higher than that in the IC group (Figure 4A,B). The NGR1 pretreatment further increased the survival of the transplanted hiPSC-CMs.
2.5. NGR1 Pretreatment Reduces Apoptosis in Cardiac Tissue
DAPI and TUNEL staining results revealed a significant increase in apoptotic cells following infarction. Transplantation of hiPSC-CMs reduced the number of apoptotic cells, while the transplantation of NGR1-pretreated hiPSC-CMs led to a more pronounced reduction in apoptosis compared to the hiPSC-CMs-only group (Figure 5A,B).
2.6. NGR1-Pretreated hiPSC-CM Transplantation Promotes Angiogenesis
von Willebrand Factor (vWF) staining demonstrated that transplantation of hiPSC-CMs significantly increased the number of vWF-positive vessels. The NIC group exhibited a larger number of vWF-positive vessels than the IC group, indicating that transplantation of NGR1-pretreated hiPSC-CMs more effectively promoted angiogenesis in the infarcted region (Figure 6A,B). Angiogenesis can reduce the degree of MI, decrease cardiomyocyte apoptosis and necrosis, improve cardiac remodeling, and also improve the living environment of stem cells.
2.7. NGR1-Pretreated hiPSC-CM Transplantation Enhances Lymphangiogenesis
Lyve1 staining showed a significant increase in the number of Lyve1-positive vessels following hiPSC-CM transplantation, with the NIC group exhibiting a greater number of Lyve1-positive vessels than the IC group. This suggests that NGR1 pretreatment enhanced the ability of hiPSC-CMs to promote lymphangiogenesis in the infarcted area (Figure 7A,B). Lymphoneogenesis can reduce myocardial edema and interstitial pressure, regulate the immune response, promote the clearance of necrotic tissue, and inhibit cardiac remodeling and fibrosis.
2.8. NGR1-Pretreated hiPSC-CM Transplantation Stimulates Paracrine Secretion
Quantitative RT-PCR analysis of mRNA levels for SCF, VEGF, IGF-1, SDF-1, and VEGFC in myocardial tissue from the infarcted region of nude mice showed that, compared to the MI group, transplantation of hiPSC-CMs increased the expression of SDF-1. Notably, the levels of VEGFC, IGF-1, and SDF-1 were significantly higher in the NGR1-pretreated hiPSC-CM transplantation group compared to both the hiPSC-CMs-only and MI groups, with statistically significant differences observed (Figure 8A–E).
2.9. Regulation of PI3K/Akt Signaling Pathway in hiPSC-CMs by NGR1
To clarify the protective mechanism of NGR1 on hiPSC-CMs, the level of Akt was detected in vitro. Treatment of hiPSC-CMs with 0.1 μM NGR1 resulted in a significant increase in p-Akt levels between 24 and 48 h (Figure S1A). The addition of the PI3K inhibitor LY294002 led to a reduction in p-Akt levels (Figure S1B). However, none of the NGR1 concentrations tested had a significant impact on the proliferation of the hiPSC-CMs (Figure S1C).
3. Discussion
Myocardial differentiation of hiPSCs is typically achieved by recapitulating the regulation of key transcription factors and signaling pathways involved in embryonic heart development [14]. Notably, transcription factors such as GATA4 and NKX2.5 are tightly regulated, and the temporal activation and inhibition of the Wnt/β-catenin signaling pathway constitutes a critical determinant for efficient myocardial regeneration [15]. Direct transplantation of allogeneic hiPSCs, however, may elicit severe immune rejection. Gene-editing strategies, including B2M knockout and HLA-E overexpression, can generate hiPSCs and their derivatives with reduced immunogenicity, thereby enhancing transplant survival [16]. In vitro-directed differentiation of hiPSCs can produce substantial numbers of hiPSC-CMs exhibiting characteristic myocardial markers and contractile function [17]. Preclinical studies have demonstrated that transplanted hiPSC-CMs can integrate into host myocardial tissue, improve cardiac contractility, and mitigate myocardial fibrosis, although these effects are often limited [18]. Beyond immunogenicity, the ischemic, hypoxic, and immunologically stressful environment at the transplantation site contributes to significant loss of transplanted cells. To enhance the therapeutic efficacy of hiPSC and hiPSC-CM transplantation, combination strategies have emerged as a key research focus. Incorporation of collagen-based scaffolds to simulate the myocardial extracellular matrix can facilitate the colonization and functional integration of hiPSC-CMs [19]. Gene-edited hiPSC-CMs can further improve transplanted cell survival and myocardial repair by promoting angiogenesis and ameliorating hypoxic conditions [20]. Additionally, pharmacological co-treatment with stem cell transplantation has shown promise in multiple preclinical studies. Our previous work demonstrated that NGR1 combined with MSC transplantation significantly enhances both the survival and therapeutic efficacy of transplanted cells [12,13].
As a diterpenoid saponin primarily derived from Panax notoginseng, NGR1 exhibits anti-inflammatory and antioxidant properties, making it a promising candidate for combinatory therapeutic applications [21]. Our preliminary investigations demonstrated that NGR1 enhances the therapeutic efficacy of MSC transplantation in MI through activation of the PI3K/Akt signaling pathway. This pathway functions as a critical regulatory hub for cell survival, proliferation, immune response, and metabolism, modulating cellular responses to extracellular stimuli and intracellular environmental changes [22]. Phosphatidylinositol 3-kinase (PI3K) is a key signal transduction molecule that is activated by receptor tyrosine kinases (RTKs) and other membrane receptors. Upon activation, PI3K catalyzes the conversion of membrane phosphatidylinositol 4,5-bisphosphate (PIP2) into phosphatidylinositol 3,4,5-triphosphate (PIP3). The production of PIP3 recruits protein kinase B (Akt) to the cell membrane, promoting its phosphorylation and conformational activation [23]. Activated Akt phosphorylates downstream targets such as forkhead box protein O1 (FoxO1), thereby inhibiting pro-apoptotic proteins, enhancing cell survival, reducing the secretion of pro-inflammatory cytokines (e.g., TNF-α and IL-6), and regulating glucose metabolism and protein synthesis [24]. Activation of the PI3K/Akt pathway also upregulates intracellular antioxidant enzymes, including superoxide dismutase and catalase, and mitigates inflammation by cross-regulating pathways such as NF-κB and MAPK, ultimately suppressing oxidative stress- and inflammation-induced apoptosis [25]. Our data indicate that NGR1 pretreatment did not significantly enhance the proliferation of hiPSC-CMs but markedly increased Akt phosphorylation. The PI3K inhibitor LY294002 effectively suppressed this phosphorylation. Compared to direct hiPSC-CM transplantation, NGR1-pretreated hiPSC-CMs exhibited improved survival in cardiac tissue, reduced myocardial apoptosis, enhanced cardiac function, and decreased infarct size and collagen deposition. These findings possibly suggest that NGR1 pretreatment promotes hiPSC-CM survival post-transplantation and improves the therapeutic efficacy of hiPSC-CM transplantation in MI via PI3K/Akt pathway activation.
The cardiac microvascular system, comprising capillaries, arterioles, and venules, is essential for myocardial perfusion, and its reconstruction is critical for tissue survival and functional recovery [26]. Physiologically, microvessels regulate blood flow, ensuring adequate oxygen and nutrient delivery to the myocardium [27]. Following MI, angiogenesis—mediated by endothelial cell proliferation, migration, and lumen formation—is crucial for tissue repair and is regulated by diverse growth factors [28]. This study found that NGR1 pretreatment promoted hiPSC-CM angiogenesis and increased the expression of related factors.
Cardiac lymphatic vessels, distributed throughout the myocardium and epicardium, are vital for fluid clearance and modulation of inflammatory responses [29]. Promoting lymphangiogenesis accelerates the removal of inflammatory cells, mitigates myocardial fibrosis, inhibits pathological remodeling, and improves cardiac function [30]. Lymphatic endothelial cells, which express the marker Lyve1, are essential for lymphatic vessel formation and functional maintenance [31]. The VEGFC/VEGFR-3 axis is a central signaling pathway that regulates cardiac lymphangiogenesis, facilitating lymphatic neogenesis and protecting cardiac function by modulating intracellular signaling and reducing cardiomyocyte apoptosis and inflammation [32]. We observed that transplantation of NGR1-pretreated hiPSC-CMs significantly increased VEGFC expression and the density of Lyve1-positive lymphatic vessels, indicating that this strategy promotes lymphangiogenesis and improves cardiac function via VEGFC regulation.
Angiogenesis and lymphangiogenesis are interconnected processes in cardiac repair, sharing overlapping molecular mechanisms. Following myocardial injury, microvascular growth coincides with chronic inflammation and fibrosis, whereas lymphatic dysfunction exacerbates tissue edema and inflammation [33]. Endothelial injury and endothelial-to-mesenchymal transition reduce vascular density and function, while TGF-β secretion activates cardiac fibroblasts [34]. Lymphatic impairment hinders the clearance of pro-inflammatory factors and necrotic cells, perpetuating inflammation and extracellular matrix accumulation [35]. Therefore, coordinated regulation of vascular and lymphatic networks is essential for effective myocardial repair. VEGFC, through VEGFR-3 activation, promotes lymphangiogenesis and also contributes to angiogenesis via VEGFR-2, highlighting the dual vascular and lymphatic remodeling facilitated by NGR1 in myocardial tissue repair [36].
SDF-1 is a chemokine that directs stem cell recruitment, migration, and engraftment in ischemic regions via chemotactic gradients [37,38]. SDF-1 mediates the PI3K/Akt pathway, reducing apoptosis while promoting cell migration and differentiation [39]. Additionally, SDF-1 stimulates the secretion of reparative factors, including IGF-1 and SCF, to enhance myocardial repair [40]. IGF-1 inhibits cardiomyocyte apoptosis through regulation of anti-apoptotic proteins such as Bcl-2, promotes angiogenesis and lymphangiogenesis via VEGFR-3, activates the PI3K/Akt/mTOR axis, and stimulates lymphatic endothelial progenitor proliferation, thereby improving cardiac function [41,42]. IGF-1 also interacts with NF-κB signaling to reduce inflammation and attenuate ischemic injury [43]. In our study, transplantation of NGR1-pretreated hiPSC-CMs significantly elevated myocardial expression of VEGFC, SDF-1, and IGF-1, collectively promoting myocardial repair through anti-apoptotic, antioxidant, and pro-regenerative mechanisms. However, the specific mechanism by which NGR1 pretreatment promotes the effects of hiPSC-CM against myocardial injury still needs further study.
Our research demonstrates that the transplantation of hiPSC-CMs pre-treated with NGR1 effectively mitigates MI-induced ventricular remodeling, preserves cardiac function, and enhances the resistance of the transplanted stem cells to oxidative stress-induced apoptosis. NGR1 pretreatment is a simple and feasible method with good clinical translation prospects. Although this study is in its preliminary stages, focusing on animal and cellular models, it provides valuable insights for the development of drug–stem cell combination therapies with potential clinical translational relevance. It is also necessary to improve the maturity of hiPSC-CMs, avoid the risk of arrhythmia, and optimize the dosage of NGR1. We aim to further explore and refine this system by improving the resistance of transplanted stem cells to oxidative stress, immune modulation, and other challenges [44]. This will help address electrophysiological issues, such as the integration of myocardial tissue post-transplantation [45]. Additionally, it is crucial to optimize the drug dosing and stem cell differentiation protocols for various transplantation contexts, conduct safety assessments during the translational process, and refine the overall methodology to ensure the biological integrity of the product, compliance with current Good Manufacturing Practices (cGMP), and patient safety [46]. We believe that emerging omics technologies and interdisciplinary materials have the potential to accelerate progress in the exploration and treatment of cardiovascular diseases [47,48].
4. Materials and Methods
4.1. hiPSC Cultivation
Frozen cells (National Collection of Authenticated Cell Cultures, Shanghai, China) were quickly thawed in a 37 °C water bath and transferred to 5 mL of mTeSR1 culture medium (STEMCELL Technologies, 85857, Vancouver, BC, Canada). The cells were centrifuged at 200× g for 5 min to remove the supernatant. Then, the cells were resuspended in 6 mL of mTeSR1 culture medium containing 5 mM Y27632 (Tocris, 1254, Bristol, UK) and transferred to a 6-well plate with matrix gel. After 24 h, the cell culture medium was replaced with mTeSR1 culture medium without Y27632. The culture medium was changed daily. When the cells reached 80–90% confluence, they were digested in a 37 °C incubator with Versene (Thermo Fisher, 15040066, Waltham, MA, USA) for 4 min. Digestion was stopped with 3 mL of mTeSR1 culture medium containing 5 mM Y27632. After centrifugation and resuspension, the cells were cultured in 9 mL of mTeSR1 culture medium containing 5 mM Y27632. The ratio was 1:6.
4.2. Induced Differentiation of hiPSC
The cells in the 6-well plate were digested with 1 mL Accutase (Thermo Fisher, 00-4555-56) for 8 min, centrifuged at 200× g for 5 min, resuspended in mTeSR1 culture medium and counted. The cells were then resuspended in Y27632 and mTeSR1 culture medium at a concentration of 2 million/mL. Then, 0.5, 0.75, 1 million, 1.25 million, and 1.5 million cells were added to each well of a 12-well plate, and the culture medium was supplemented to 1 mL with Y27632 and mTeSR1. The time point was −4 days. During the following 3 days, the culture medium was replaced every day. On day 0, each well was replaced with 2 mL of RPMI (Thermo Fisher, 11875093)/B27 (Thermo Fisher, 17504044) insulin culture medium containing 12 μM CHIR99021 (Selleckchem, S1263, Houston, TX, USA). On the first day, it was switched to RPMI/B27 insulin culture medium. On the third day, it was replaced with 2 mL of combined medium, which consisted of 1 mL of culture medium, 1 mL of RPMI/B27 insulin culture medium, and 5 μM IWP2 (Merck, I0536, Darmstadt, Germany). Then, it was replaced with 2 mL of RPMI/B27 insulin culture medium at 5 days. The culture medium was replaced with RPMI/B27 every 7 days and every 3 days thereafter. The above scheme is based on verified relevant papers [49].
4.3. Detection of Cardiac Cell Markers in hiPSC-CM
The cells in each well were washed with PBS, digested with 0.5 mL of 0.25% Trypsin EDTA (Corning Cellgro 25-051-CI, Corning, NY, USA) at 37 °C for 5 min. Then, 2 mL of RPMI20 culture medium was added. The cells were centrifuged at 200× g for 5 min and resuspended in Y27632 and mTeSR1 culture medium at a concentration of 100,000/mL. Subsequently, 1 mL of 0.1% gelatin was added to each well. Two days later, the cells were fixed with 4% formaldehyde at room temperature for 15 min, followed by two washes with PBS. They were then permeabilized with 0.4% Tritonx-100 for 5 min. Subsequently, the cells were incubated at room temperature for 1 h with anti-cardiac troponin T (cTnT) primary antibody (Abcam, ab209813, Cambridge, UK), washed three times with PBS, and incubated in the dark for 30 min with secondary antibody. After three additional PBS washes, the cells were photographed.
4.4. CCK8 Testing
A total of 10,000 cells were seeded into each well of a 96-well plate and cultured in RPMI/B27 culture medium containing the corresponding concentration of NGR1. After 24 h, the culture medium was discarded from each well and replaced with RPMI/B27 culture medium containing 10% CCK8. The cells were incubated in the incubator for 1 h and the absorbance in each well was measured at 450 nm. The concentration and duration of all NGR1-related treatments in this study were based on our previous exploration [12].
4.5. Western Blot
After treatment with corresponding concentrations of LY294002 (Selleck.cn, S1105, Shanghai, China) and NGR1, proteins were digested and extracted using RIPA (Beyotine, P0013B, Shanghai, China. The concentration was balanced using the BCA method. LDS was added and denatured at 70 °C for 10 min, followed by 200 V electrophoresis for 25 min and 100 V membrane transfer for 90 min. The primary antibodies p-Akt (Ser473) (CST, 4060, Danvers, MA, USA), Akt (C67E7) (CST, 4691), and GAPDH (14C10) (CST, 2118) were incubated at 1:1000 at 4 °C overnight, and the secondary antibodies were incubated at room temperature for 1 h before exposure and photography.
4.6. Nude Mouse Model and Cell Transplantation
Adult nude mice weighing 19–21 g were divided into a sham surgery group (Sham, injected an equal volume of physiological saline solution) with 8 mice, a model group (MI) with 12 mice, an hiPSC-CM injection group (IC) with 12 mice, and an NGR1-pretreated hiPSC-CM injection group (NIC) with 12 mice, with NGR1 pretreatment for 24 h. The MI, IC, and NIC groups of nude mice were anesthetized with isoflurane and fixed. A 1cm incision was made near the third and fourth intercostal spaces on the left side of the sternum, and the skin was bluntly separated from the intercostal spaces to squeeze out the heart. The left anterior descending branch (LAD) of the coronary artery was ligated 1mm below the left atrial appendage. After ligation, 500,000 hiPSC-CM or NGR1-pretreated hiPSC-CM were injected into the left ventricular infarction zone at 3 sites of nude mice in the IC and NIC groups. The hearts of the nude mice were returned to the chest cavity, and the skin was sutured. The mortality rate was about 40%, with a total of 11 deaths, including 4 in the MI group, 4 in the IC group, and 3 in the NIC group. The mice were humanely euthanized by an overdose of carbon dioxide inhalation.
4.7. Echocardiography
At 2 and 4 weeks of modeling, the nude mice were anesthetized with isoflurane and fixed. A probe was placed on the left chest wall, and a 30 MHz probe was used to obtain left ventricular M-echocardiography. Then, ejection fraction (EF), left ventricular short axis fractional shortening (FS), left ventricular end diastolic volume (LVEDV), left ventricular end systolic volume (LVESV), left ventricular diastolic diameter (LVIDd), and left ventricular systolic diameter (LVIDs) were measured and calculated.
4.8. Masson’s Trichrome Staining
After the heart was fixed and dehydrated, it was embedded and frozen with OCT, and then sliced. The frozen slices were dried at room temperature for 10 min, washed three times with PBS, and stained overnight with Bouin at room temperature. Subsequently, Masson’s trichrome staining was performed according to the manufacturer’s instructions. For morphometric parameters, the percentage of infarct area was obtained by dividing the blue collagen area by the left ventricular area in the 8 bit mode of ImageJ (2.1.0).
4.9. Immunofluorescence Staining
The frozen sections were dried at room temperature for 10 min, washed three times with PBS, and the 0.5% TritonX-100 membrane was broken at room temperature for 15 min. Sections were blocked with goat serum at 37 °C for 30 min and then incubated with primary antibody overnight at 4 °C and washed three times with PBS. Subsequently, the sections were incubated with secondary antibody at room temperature in the dark for 1 h. After being washed with PBS again, the cell nucleus was co-stained with DAPI in the dark for 10 min. After sealing, the slices were photographed.
4.10. RT-qPCR Detection
Total RNA was extracted from ventricular samples, and the concentration was measured. cDNA was obtained through reverse transcription using the Adamas life 5 × Reverse Transcription Mix kit (Adamas life, G8041-0010, Shanghai, China). A 20 μL reverse transcription system was prepared at 42 °C for 15 min and 95 °C for 30 s. The cDNA was diluted 5 times. An RT-qPCR system of 20 μL was prepared with qPCR SYBR Master Mix. The reaction procedure involved pre-denaturation at 95 °C for 15 min, followed by fluorescence collection at 60 °C for 30 s after 10 s at 95 °C for 40 cycles of denaturation. The dissolution curve was adapted using a machine program. The primer sequence of vascular endothelial growth factor A (VEGF), vascular endothelial growth factor C (VEGFC), insulin-like growth factor-1 (IGF-1), stromal cell-derived factor-1 (SDF-1), stem cell factor (SCF), and glyceraldehyde-3-phosphate dehydrogenase (GAPDH) are shown in Table 1.
4.11. Statistical Analysis
All statistical analyses were performed using IBM SPSS 27. Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data or median (interquartile range) for non-normally distributed data. The normality of data distribution was assessed using the Shapiro–Wilk test. Group comparisons for continuous variables were conducted using Student’s t-test (for normally distributed data) or the Mann–Whitney U test (for non-normally distributed data). For comparisons among more than two groups, one-way ANOVA was performed, followed by Bonferroni’s post hoc test for multiple comparisons. Correlation analysis was performed using Pearson’s correlation coefficient for normally distributed data or Spearman’s rank correlation coefficient for non-normally distributed data. Univariate and multivariate Cox proportional hazards models were employed to estimate hazard ratios (HRs) and their 95% confidence intervals (CIs). A two-sided p-value < 0.05 was considered statistically significant. The sample size was determined based on a power analysis with an α of 0.05 and β of 0.20 (power of 80%).
4.12. Experimental Flowchart
To facilitate a quick understanding of the design of this study, all the schemes presented in this study can be seen in the figure below (Figure 9).
5. Conclusions
hiPSC can be efficiently differentiated into cardiomyocytes through modulation of GSK3 and Wnt signaling and optimization of cell density. NGR1 enhances p-Akt levels in hiPSC-CMs and, when used as a pretreatment, improves the therapeutic efficacy of hiPSC-CM transplantation in MI by promoting graft survival and activating paracrine repair mechanisms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rao S.V. O’Donoghue M.L. Ruel M. Rab T. Tamis-Holland J.E. Alexander J.H. Baber U. Baker H. Cohen M.G. Cruz-Ruiz M. 2025 ACC/AHA/ACEP/NAEMSP/SCAI Guideline for the Management of Patients With Acute Coronary Syndromes: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines J. Am. Coll. Cardiol.20258521352237 Correction in J. Am. Coll. Cardiol. 2025, 85, 1800. Correction in J. Am. Coll. Cardiol. 2025, 86, 272310.1016/j.jacc.2024.11.0094001374 · doi ↗ · pubmed ↗
- 2Nicolau A.M. Silva P.G. Mejia H.P.G. Granada J.F. Kaluza G.L. Burkhoff D. Abizaid T. Pileggi B. Freire A.F.D. Godinho R.R. Molecular Mechanisms of Microvascular Obstruction and Dysfunction in Percutaneous Coronary Interventions: From Pathophysiology to Therapeutics-A Comprehensive Review Int. J. Mol. Sci.202526683510.3390/ijms 2614683540725082 PMC 12295318 · doi ↗ · pubmed ↗
- 3Wang Y. Xue Y. Guo H.D. Intervention effects of traditional Chinese medicine on stem cell therapy of myocardial infarction Front. Pharmacol.202213101374010.3389/fphar.2022.101374036330092 PMC 9622800 · doi ↗ · pubmed ↗
- 4Han L. Mich-Basso J. Kuhn B. Generation of Human Induced Pluripotent Stem Cells and Differentiation into Cardiomyocytes Methods Mol. Biol.2021215812513910.1007/978-1-0716-0668-1_1032857370 PMC 8221246 · doi ↗ · pubmed ↗
- 5Sugiura T. Shahannaz D.C. Ferrell B.E. Current Status of Cardiac Regenerative Therapy Using Induced Pluripotent Stem Cells Int. J. Mol. Sci.202425577210.3390/ijms 2511577238891960 PMC 11171475 · doi ↗ · pubmed ↗
- 6Ai X. Yan B. Witman N. Gong Y. Yang L. Tan Y. Chen Y. Liu M. Lu T. Luo R. Transient secretion of VEGF protein from transplanted hi PSC-C Ms enhances engraftment and improves rat heart function post MI Mol. Ther.20233121122910.1016/j.ymthe.2022.08.01235982619 PMC 9840120 · doi ↗ · pubmed ↗
- 7Cheng Y.C. Hsieh M.L. Lin C.J. Chang C.M.C. Huang C.Y. Puntney R. Wu Moy A. Ting C.Y. Herr Chan D.Z. Nicholson M.W. Combined Treatment of Human Induced Pluripotent Stem Cell-Derived Cardiomyocytes and Endothelial Cells Regenerate the Infarcted Heart in Mice and Non-Human Primates Circulation 20231481395140910.1161/CIRCULATIONAHA.122.06173637732466 PMC 10683868 · doi ↗ · pubmed ↗
- 8Sun B. Wang L. Guo W. Chen S. Ma Y. Wang D. New treatment methods for myocardial infarction Front. Cardiovasc. Med.202310125166910.3389/fcvm.2023.125166937840964 PMC 10569499 · doi ↗ · pubmed ↗