Colchicine Use in Acute Coronary Syndrome: A Systematic Review and Meta-Analysis
Huey Chiat Cheong, Meng Hsuan Kuo, Chih-Wei Tseng, Yi-Da Li

TL;DR
This study reviews whether colchicine helps reduce heart-related risks after acute coronary syndrome, finding mixed results and common side effects.
Contribution
A systematic review and meta-analysis of colchicine's efficacy in acute coronary syndrome patients, focusing on MACE and safety.
Findings
Colchicine marginally reduces major adverse cardiovascular events (MACE) risk.
Gastrointestinal side effects, especially diarrhea, are most common with colchicine use.
No significant benefit observed for mortality or other cardiovascular outcomes.
Abstract
Background: This study aimed to assess the efficacy, optimal dosing, and timing of colchicine therapy in reducing major adverse cardiovascular events (MACE), its impact on inflammatory markers, and safety concerns in patients following acute coronary syndrome (ACS) through a systematic review and meta-analysis of randomized controlled trials (RCTs). Methods: A comprehensive search of PubMed, Embase, and the Cochrane Library was conducted in accordance with PRISMA guidelines to identify RCTs comparing colchicine versus placebo or standard treatment in ACS patients. The primary outcome was MACE and secondary outcomes included all-cause and cardiovascular mortality, non-fatal MI, stroke, revascularization, heart failure, CRP/hs-CRP changes, and adverse effects. Fifteen RCTs involving 19,131 patients were analyzed. Results: The benefit of colchicine in reducing MACE risk was marginally…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
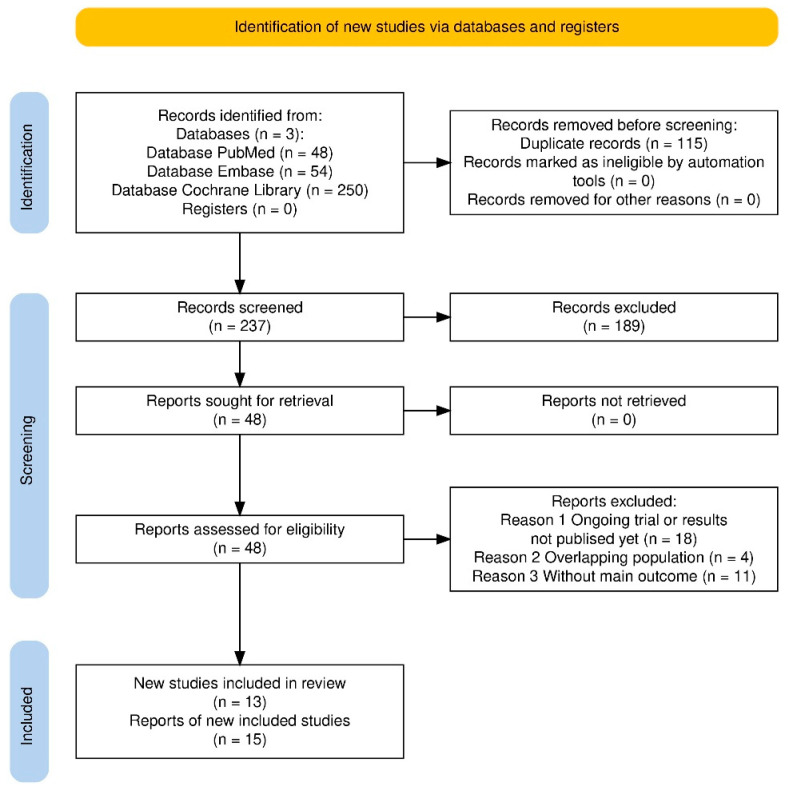 Figure 1
Figure 1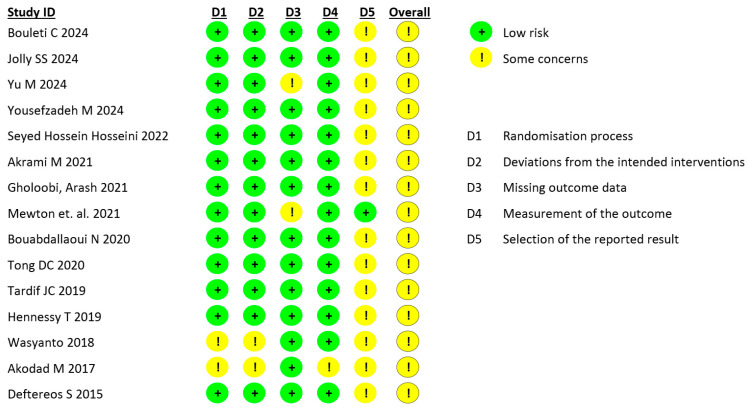 Figure 2
Figure 2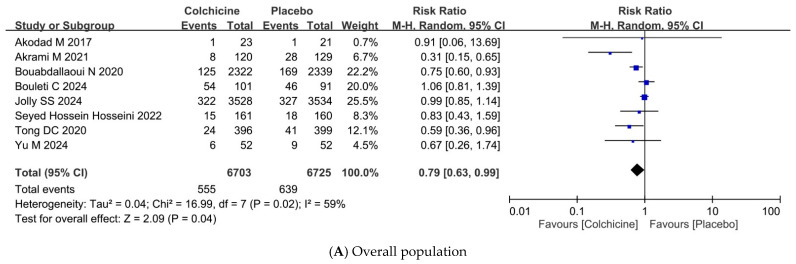 Figure 3
Figure 3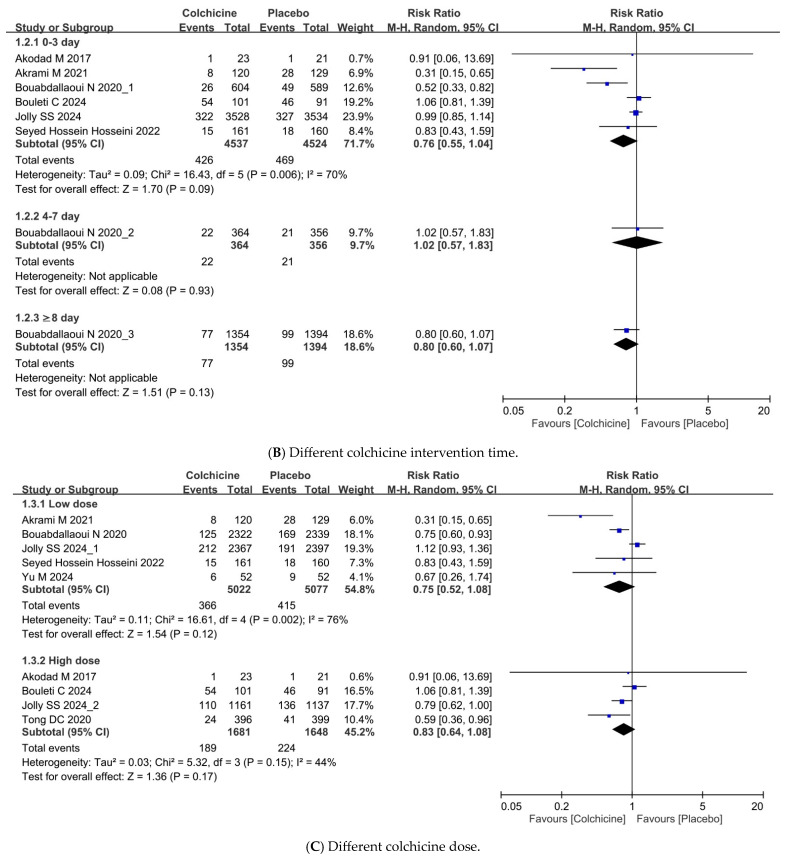 Figure 4
Figure 4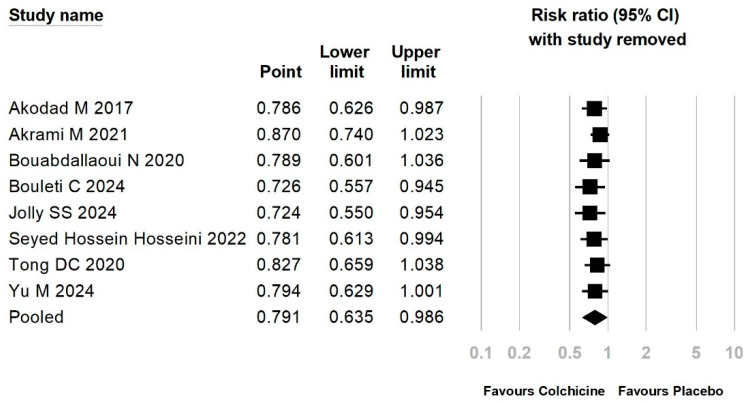 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammasome and immune disorders · Biomarkers in Disease Mechanisms · Adipokines, Inflammation, and Metabolic Diseases
1. Introduction
Inflammation is vital for myocardium recovery after acute coronary syndrome (ACS), but prolonged immune activation can exacerbate tissue damage [1,2]. High levels of inflammatory markers like C-reactive protein (CRP) were found to predict an unfavorable disease course during acute myocardial infarction (AMI) [3,4]. A previous anti-inflammatory drug trial targeting interleukin-1β in atherosclerotic disease observed a significant reduction in cardiovascular death, but at the expense of increased fatal infection, emphasizing the importance of balanced inflammatory regulation [5].
Colchicine is attractive as an anti-inflammatory medication due to its affordability, availability and relatively safe profile [6,7]. It was brought to attention when a retrospective, cross-sectional study showed lower myocardial infarction prevalence in gout patients using colchicine [8]. Subsequent randomized trials yielded mixed results when colchicine was used in patients with ACS. A significant reduction in major adverse cardiovascular events (MACE) was observed in the COLCOT study when colchicine was used within 30 days of AMI, and it was most efficacious when prescribed within the first three days [9,10]. Akrami et al. [11] supported the findings of this study. In contrast, the COVERT-MI [12], COPS [13], and Yousefzadeh et al. [14] trials failed to show significant benefits. Most recently, the CLEAR-SYNERGY (OASIS 9) trial (N = 7062) also reported no significant advantage of low-dose colchicine compared with placebo, even when administered within three days of AMI onset [15].
The conflicting findings surrounding colchicine’s therapeutic effects are apparent not only in its influence on MACE but also in its modulation of inflammatory biomarkers. CRP and high-sensitivity CRP (hs-CRP) were commonly assessed in prior investigations; however, results across these studies have remained inconsistent [14,16,17,18,19].
The observed inconsistencies in clinical outcomes may, in part, be attributable to variations in treatment regimens. The COLCOT trial demonstrated the greatest reduction in MACE when colchicine was administered within the first three days of AMI. However, this finding was not replicated in the CLEAR-SYNERGY (OASIS 9) trial. Across studies, colchicine regimens have varied considerably, with some trials requiring a loading dose [14,20,21], while others omitted it, followed by either a low-dose (0.5 mg once daily) [9,10,11,14] or high-dose maintenance regimen (1.0 mg once daily or 0.5 mg twice daily) [12,13]. Furthermore, discrepancies in time-to-treatment initiation [10,17,18] and the duration of use [9,12,16] may further complicate interpretation. These variations underscore the need for subgroup meta-analyses to clarify the optimal regimen and inform evidence-based prescribing strategies.
Despite conflicting trial results, previous meta-analyses have supported the use of colchicine in patients with coronary artery disease [22,23,24,25]. The American Heart Association (AHA) guideline provided a Class IIb recommendation on long-term use of low-dose colchicine to reduce the risk of MACE after ACS [26], while the European Society of Cardiology (ESC) guideline gives a Class IIb recommendation for ACS [27] and a Class IIa for chronic coronary syndrome [28]. The results of the CLEAR-SYNERGY (OASIS 9) trial [15] offer a timely opportunity for an updated systematic review and meta-analysis to clarify colchicine’s therapeutic role and optimal regimen in ACS. This study aimed to provide an updated assessment of its efficacy and dosing strategies.
2. Materials and Methods
This systematic review and meta-analysis was pre-registered on PROSPERO (ID number: CRD420251041546) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Table S1) [29].
2.1. Search Strategy
A comprehensive search was conducted in PubMed, Embase and the Cochrane Library from database inception to 23 January 2025, with no language restrictions, to identify relevant RCTs (randomized controlled trials). The search strategy was developed by two researchers (CWT and MHK) (Table S2). The key search terms included “acute coronary syndrome”, “acute myocardial infarction” and “colchicine”, incorporating Medical Subject Headings (MeSH), where applicable. Additional articles were identified in the reference lists of pertinent original studies and relevant reviews.
2.2. Inclusion Criteria
After removing duplicate records, two reviewers (YDL and HCC) independently selected the included studies based on the following parameters: (1) Patients: Adults with acute coronary syndrome; (2) Exposures: colchicine; (3) Comparison: placebo or standard treatment; (4) Outcome: MACE (cardiovascular mortality, non-fatal myocardial infarction, stroke, angina requiring revascularization, and heart failure), all-cause mortality, inflammatory level change (CRP and hs-CRP), and adverse effects (gastrointestinal side effects, hematologic events (myelotoxicity or myelosuppression, such as anemia, leukopenia, thrombocytopenia or pancytopenia), and infections); (5) Study design: RCTs only.
2.3. Literature Selection and Data Extraction
Two reviewers (YDL and HCC) individually screened titles and abstracts based on the inclusion criteria and read the full-text articles for final eligibility. A third reviewer (CWT) was consulted to resolve any discrepancies in the study selection.
Two authors (YDL and HCC) independently collected data, including the name of the first author, publication year, country, study population, number of patients, treatment regimens (dose, duration, duration of intervention, and time to first colchicine intervention), follow-up period, age, sex ratio, comorbidity, co-medication, and statistical data on the influence of safety and adverse events. For continuous variables, means and standard deviations (SDs) were extracted. If SDs for changes from baseline were not reported, they were imputed using a correlation coefficient approach [30]. Any discrepancies in data extraction were resolved by discussion. Two study cohorts were found to report on two different outcome measures in different publications. Only the required outcome data were extracted from each of the publications, while taking caution to avoid duplicates during analysis (COVERT-MI study: Data related to MACE from Bouleti et al. [20], CRP and left ventricular thrombus from Mewton et al. [12]; COLCOT study: Data related to time to first intervention and corresponding MACE from Bouabdallaoui et al. [10], and adverse effects from Tardif et al. [9]).
2.4. Risk of Bias Assessment
The methodological quality of included RCTs was assessed by two researchers (YDL and MHK) independently. We used the Cochrane Collaboration’s ROB tool 2.0 [31], addressing the critical domains of randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result and overall bias, to evaluate the methodological quality of the included RCTs.
2.5. Data Synthesis and Statistical Analysis
We conducted a random-effects meta-analysis due to the expected clinical heterogeneity among the included RCTs. Statistical heterogeneity across the included studies was quantified using the I^2^ statistic, with substantial heterogeneity defined as I^2^ > 50 [30]. Subgroup analyses performed included colchicine intervention time (0–3 days, 4–7 days, and ≥8 days) in accordance with the COLCOT study design [10] and colchicine dosage (low dose: ≤0.5 mg/day; high dose: >0.5 mg/day). Publication bias was evaluated by assessing funnel plot asymmetry for meta-analyses of outcomes that included ≥10 studies [32]. To assess the robustness of the results of our main analyses, we conducted a sensitivity analysis using the leave-one-out meta-analysis. A two-sided p < 0.05 was considered statistically significant, and all analyses were performed using Comprehensive Meta-Analysis software (version 4.0, Biostat, Englewood, NJ, USA) and Review Manager Version 5.3 (Cochrane Collaboration, 2020).
2.6. Certainty of Evidence of the Study Outcomes
Two independent reviewers (MHK and HCC) evaluated the CoE for each study outcome based on the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria [33]. Any discrepancy between the review authors was resolved by discussion with the senior author (CWT).
The datasets generated and analyzed during this current study are available from the corresponding author upon reasonable request via E-mail.
3. Results
3.1. Literature Search and Study Selection
A total of 352 records were identified through database searches (PubMed: 48, Embase: 54, Cochrane Library: 250). After removing 115 duplicate records, 237 studies were screened based on titles and abstracts. Following the exclusion of 189 ineligible studies, 48 full-text articles were assessed for eligibility. Of these, 33 studies were excluded due to ongoing trials or lack of published results (n = 18), overlapping study populations (n = 4), and lack of primary outcome reporting (n = 11). Ultimately, 15 RCT reports were included in this meta-analysis, and were all written in English. The PRISMA flow diagram illustrating the study selection process is provided in Figure 1.
3.2. Characteristics of Included Studies
The meta-analysis included 15 RCT reports, comprising a total of 19,131 patients with ACS. The study populations varied in terms of geographic location, baseline characteristics, colchicine dosing regimens, and follow-up duration (Table 1). The majority of studies enrolled patients with ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), or unstable angina (UA), with sample sizes ranging from 44 to 7062 participants. The duration of follow-ups ranged from 30 days to 2.98 years.
The baseline characteristics of the study populations were generally comparable, with mean ages ranging from 54.5 to 61 years, and predominantly male participants. The prevalence of key cardiovascular risk factors varied, with smoking (30–72%), hypertension (31–51%), diabetes (13–49%), and dyslipidemia (13–52%) reported across the studies. Further details on study characteristics, including comorbidities and concurrent cardiovascular therapies, are provided in Table 1.
3.3. Risk of Bias of Included Studies
All included studies were assessed as having some concerns in the overall risk of bias evaluation. The primary source of bias was the potential for selective reporting of results (Figure 2).
3.4. Primary Outcome: MACE and Subgroup Analyses
Among the eight RCTs with reporting MACE, comprising 13,428 patients, colchicine reduced the risk of MACE compared to placebo or standard treatment at a marginal statistical significance (RR = 0.79, 95% CI: 0.63–0.99, p = 0.04) (Figure 3A, Table 2). However, moderate heterogeneity (I^2^ = 59%) was observed across studies, suggesting some variability in treatment effects among different populations and study designs.
Subgroup analyses based on the timing of colchicine initiation did not reveal a clear benefit. Initiation within 0–3 days post-ACS (RR = 0.76, 95% CI: 0.55–1.04, p = 0.09, I^2^ = 70%), 4–7 days post-ACS (RR = 1.02, 95% CI: 0.57–1.83, p = 0.93), and ≥8 days post-ACS (RR = 0.80, 95% CI: 0.60–1.07, p = 0.13) showed no significant reduction in MACE risk (Figure 3B). Similarly, neither low-dose colchicine (≤0.5 mg/day) (RR = 0.75, 95% CI: 0.52–1.08, p = 0.12, I^2^ = 76%) nor high-dose colchicine (>0.5 mg/day) (RR = 0.83, 95% CI: 0.64–1.08, p = 0.17, I^2^ = 44%) significantly reduced MACE (Figure 3C).
3.5. Secondary Outcomes: All-Cause Mortality, Cardiovascular Mortality, Non-Fatal Myocardial Infarction, Stroke, Angina Requiring Revascularization, Heart Failure, Crp Change, Hs-Crp Change
Colchicine treatment did not demonstrate a significant effect on mortality outcomes (Table 2). The pooled analysis of nine RCTs including 13,548 patients showed no significant reduction in all-cause mortality (RR = 0.94, 95% CI: 0.78–1.12, p = 0.45, I^2^ = 0%), cardiovascular mortality (RR = 1.03, 95% CI: 0.81–1.29, p = 0.51, I^2^ = 0%), or non-fatal myocardial infarction (RR = 0.85, 95% CI: 0.69–1.05, p = 0.38, I^2^ = 6%), suggesting that colchicine does not confer a survival benefit in ACS patients. Stroke risk was lower in the colchicine group but did not reach significance (RR = 0.62, 95% CI: 0.28–1.36, p = 0.15, I^2^ = 39%). Similarly, angina requiring revascularization (RR = 0.73, 95% CI: 0.45–1.20, p = 0.09, I^2^ = 53%) and heart failure incidence (RR = 0.96, 95% CI: 0.49–1.89, p = 0.21, I^2^ = 35%) remained unaffected by colchicine treatment.
As for the changes in inflammatory markers CRP (mean difference = 3.43, 95% CI: −13.38 to 20.24, p = 0.45, I^2^ = 99%) and hs-CRP (mean difference = −0.43, 95% CI: −1.28 to 0.42, p = 0.32, I^2^ = 90%), the result was not interpretable due to high heterogeneity (Supplementary Figure S2). The high heterogeneity observed suggests substantial variability among studies in terms of baseline inflammatory status, colchicine dosing, and treatment duration.
3.6. Safety Outcome
Colchicine treatment was associated with an increased risk of gastrointestinal (GI) adverse events, particularly diarrhea, but did not show a significant impact on hematologic events or infections. In the pooled analysis of 10 studies with 13,693 patients, colchicine significantly increased the incidence of GI events, including all GI symptoms and serious events (RR = 1.49, 95% CI: 1.10–2.01, p < 0.001, I^2^ = 76%) (Table 3). The most frequently reported symptom was diarrhea, with colchicine users experiencing a 76% increased risk compared to controls (RR = 1.76, 95% CI: 1.16–2.66, p = 0.001, I^2^ = 76%). The high heterogeneity suggests variability in study populations and treatment durations, but the overall trend indicates that colchicine use is associated with notable GI intolerance. Colchicine did not significantly increase the risk of hematologic events (RR = 0.59, 95% CI: 0.21–1.67, p = 0.24, I^2^ = 27%) or infections (RR = 1.10, 95% CI: 0.72–1.68, p = 0.15, I^2^ = 41%).
3.7. Publication Bias and Sensitivity Analysis
The distribution of reports on MACE, as shown in the funnel plot, exhibits a symmetrical pattern, suggesting the absence of publication bias (p = 0.07; Egger’s test) (Supplementary Figure S1). Sensitivity analysis using a leave-one-out approach demonstrated that the overall estimates for MACE and thrombosis events remained largely unchanged, indicating that no single study had a disproportionate influence on the pooled results (Figure 4).
3.8. GRADE Assessment
We judged the CoE by the GRADE criteria for our primary and secondary outcomes to be low to high (Supplementary Table S3).
4. Discussion
Our meta-analysis demonstrates that colchicine provides a borderline-significant reduction in MACE among ACS patients. There were no significant differences in all-cause mortality, cardiovascular mortality, non-fatal MI, stroke, angina requiring revascularization, and heart failure. Early initiation (<3 days) and different dosing strategies (≤0.5 mg/day vs. >0.5 mg/day) did not yield meaningful differences in outcomes. Findings for delayed time-to-initiation (≥3 days) or for changes in CRP or hs-CRP were inconclusive. Gastrointestinal side effects were more common with colchicine, potentially impacting adherence.
Although the CLEAR SYNERGY trial [15]—a large, multicenter study enrolling over 7000 patients with AMI—did not demonstrate a significant reduction in MACE with colchicine therapy, our meta-analysis, which incorporated this trial, continued to show benefits for patients with ACS. The pooled analysis of over 13,000 patients revealed a reduction in MACE (RR: 0.79, 95% CI: 0.63–0.99, p = 0.04), but with moderate heterogeneity (I^2^ = 59%). Two potential factors may account for this discrepancy. First, the variations in trial designs, patient characteristics, treatment protocols, and follow-up duration may have influenced the results. Furthermore, the definition of MACE varies among the eight RCTs (Supplementary Tables S4 and S5). This worsened heterogeneity and made our findings less robust than anticipated. Second, sensitivity analyses identified four trials having a substantial impact on the overall estimates [10,11,13,34]. Notably, the COLCOT subgroup [10] was the largest positive contributor due to its sample size. Additionally, the trials by Akrami et al. [11] and Yu et al. [34] included a relatively high number of unstable angina cases within their composite MACE definitions. The reduction in MACE observed in the Akrami et al. [11] trial was primarily attributable to a lower incidence of unstable angina, raising the possibility that colchicine may reduce the occurrence of post-infarction unstable angina. The inclusion of such data has contributed to a slightly favorable outcome seen in our analysis, and the removal of these four trials easily shifts the results to non-significance. As such, we recommend cautious interpretation of this statistical outcome. The significance would be more pronounced if there were more participants/trials included. Nonetheless, our findings are consistent with the current clinical guidelines: a Class IIb recommendation for colchicine use in ACS patients. Further high-quality studies are warranted to refine the target population and to determine which specific components of MACE derive the greatest clinical benefit.
The timing of colchicine initiation has been proposed as a critical determinant of its therapeutic efficacy. A sub-analysis of the COLCOT trial [10] reported that initiating colchicine within three days of myocardial infarction significantly reduced MACE compared to placebo (HR: 0.52; 95% CI: 0.32–0.84). However, our subgroup analysis, where most of the included trials initiated colchicine within 0–3 days, did not demonstrate statistically significant benefit (RR = 0.76, 95% CI = 0.55–1.04, p = 0.09, I^2^ = 70%). One reason is that the small sample size within each subgroup may not be sensitive enough to detect a significant difference. The other reason was the substantial heterogeneity across trials (differences in patient characteristics, study designs, and colchicine protocols), probably obscuring any potential timing effect. Interpretation of the subgroups with delayed colchicine initiation (within 4–7 days and ≥ 8 days) was limited because each was informed by only a single study. In brief, early colchicine initiation did not significantly reduce MACE, and the evidence is insufficient to confirm or refute any benefit from delayed initiation in ACS patients. Future well-powered studies specifically designed to evaluate the impact of initiation timing are warranted.
Dosing strategy has also been hypothesized to influence the efficacy of colchicine. A subgroup analysis from the CLEAR SYNERGY trial suggested a potential benefit with high-dose colchicine (0.5 mg twice daily) [15], but our meta-analysis did not reveal such an advantage. Neither low-dose colchicine (≤0.5 mg/day) (RR = 0.75, 95% CI: 0.52–1.08, p = 0.12, I^2^ = 76%) nor high-dose colchicine (>0.5 mg/day) (RR = 0.83, 95% CI: 0.64–1.08, p = 0.17, I^2^ = 44%) significantly reduced MACE. The differences in patient baseline characteristics, such as comorbidities and background therapies, may also influence individual responses, obscuring potential dose-related effects. While higher doses may provide greater anti-inflammatory effects, the effect may not be sufficient to translate into a clinically meaningful reduction in cardiovascular events. Furthermore, higher doses of colchicine are associated with a raised incidence of gastrointestinal adverse events, contributing to reduced medication adherence and attenuated clinical benefit. Overall, increasing colchicine dosage may not offer additional clinical benefit and instead, may increase the risk of adverse outcomes.
Our meta-analysis found no significant reduction in CRP or hs-CRP with colchicine use in ACS patients, consistent with prior analyses [24,36]; however, the extreme heterogeneity makes this result uninterpretable. While some trials reported reductions in these inflammatory markers [16,19], these findings may be confounded by differences in baseline inflammatory marker levels between groups and the inconsistent measurement timing. The lack of standardization has limited the meaningful interpretation of our findings. Concurrently, there are other factors that could contribute to the lack of meaningful changes in the inflammatory markers. Chronic low-grade inflammation from comorbidities may attenuate observable changes in CRP/hs-CRP. Traditional inflammatory markers like CRP may not fully capture colchicine’s anti-inflammatory impact, highlighting the need for studies using alternative biomarkers such as MMP-9, NOX2, and TGF-β1 [37], which may more accurately reflect colchicine’s anti-inflammatory effects in future studies.
Colchicine has a narrow therapeutic window. It primarily causes toxicity by disrupting cell division, especially in rapidly proliferating tissues like the gastrointestinal lining and bone marrow [6,7]. Our meta-analysis confirmed a significantly increased risk of gastrointestinal side effects, especially diarrhea, even when low-dose colchicine is used, consistent with prior meta-analyses [23,38]. Fortunately, serious adverse events such as hematological events or infections were not significantly elevated. Interestingly, one study [12] raised the issue of a potential association between colchicine and left ventricular thrombus formation, a finding that has not been consistently observed in the past [6,38]. While there were rare instances of venous thromboembolism [9,14], further investigation is required to clarify any prothrombotic risk associated with colchicine use.
This meta-analysis has several strengths, mainly by including 15 RCTs with over 19,000 patients and performing multiple subgroup analyses in an attempt to identify potential subgroups that may benefit from colchicine use. Additionally, our methodological approach, particularly the use of mean absolute change for inflammatory biomarker analysis, ensures a more accurate assessment of colchicine’s impact on systemic inflammation. However, we acknowledge several limitations. The inconsistent definition of MACE, the limited number of studies available for subgroup analysis, and the moderate to high heterogeneity made outcome interpretation difficult. In addition, most studies lacked long-term follow-up, limiting conclusions about sustained benefits of colchicine in secondary prevention. These limitations underscore the need for a well-designed study to clarify colchicine’s role in ACS.
5. Conclusions
The benefit of colchicine in ACS patients for reducing MACE is of marginal statistical significance and should be interpreted with caution due to moderate heterogeneity and sensitivity to the inclusion of certain studies. While gastrointestinal side effects are common, serious adverse events are rare, though potential thrombotic risks will require further investigation. Given these findings, colchicine may still be useful as an adjunctive therapy and could offer some cardiovascular benefits in selected ACS populations. Future large-scale trials with standardized endpoints, longer follow-up, and more sensitive inflammatory biomarkers are warranted to fully clarify its therapeutic role.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Libby P. Ridker P.M. Maseri A. Inflammation and atherosclerosis Circulation 20021051135114310.1161/hc 0902.10435311877368 · doi ↗ · pubmed ↗
- 2Frantz S. Bauersachs J. Ertl G. Post-infarct remodelling: Contribution of wound healing and inflammation Cardiovasc. Res.20098147448110.1093/cvr/cvn 29218977766 PMC 2639128 · doi ↗ · pubmed ↗
- 3Zhang X. Wang S. Fang S. Yu B. Prognostic Role of High Sensitivity C-Reactive Protein in Patients With Acute Myocardial Infarction Front. Cardiovasc. Med.2021865944610.3389/fcvm.2021.65944634109224 PMC 8181755 · doi ↗ · pubmed ↗
- 4Lim J. Davies A. Brienesse S. Mabotuwana N.S. Boyle A. Inflammatory cell response following ST-elevation myocardial infarction treated with primary percutaneous coronary intervention and its impact on cardiovascular outcomes: A systematic review and meta-analysis Int. J. Cardiol.202337611010.1016/j.ijcard.2023.01.08236758862 · doi ↗ · pubmed ↗
- 5Ridker P.M. Everett B.M. Thuren T. Mac Fadyen J.G. Chang W.H. Ballantyne C. Fonseca F. Nicolau J. Koenig W. Anker S.D. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease N. Engl. J. Med.20173771119113110.1056/NEJ Moa 170791428845751 · doi ↗ · pubmed ↗
- 6Stamp L.K. Horsley C. Te Karu L. Dalbeth N. Barclay M. Colchicine: The good, the bad, the ugly and how to minimize the risks Rheumatology 20246393694410.1093/rheumatology/kead 62538019947 PMC 10986813 · doi ↗ · pubmed ↗
- 7Leung Y.Y. Yao Hui L.L. Kraus V.B. Colchicine—Update on mechanisms of action and therapeutic uses Semin. Arthritis Rheum.20154534135010.1016/j.semarthrit.2015.06.01326228647 PMC 4656054 · doi ↗ · pubmed ↗
- 8Crittenden D.B. Lehmann R.A. Schneck L. Keenan R.T. Shah B. Greenberg J.D. Cronstein B.N. Sedlis S.P. Pillinger M.H. Colchicine use is associated with decreased prevalence of myocardial infarction in patients with gout J. Rheumatol.2012391458146410.3899/jrheum.11153322660810 PMC 3733459 · doi ↗ · pubmed ↗