Ring-like (Donut-Shaped) Intracranial Aneurysms: A Warning Morphology of Mural Jet Flow and Pre-Rupture Instability
Dragoslav Nestorović, Andrija Savić, Petar Milenković, Miloš Stojaković, Tamara Švabić, Igor Nikolić

TL;DR
This paper identifies ring-like intracranial aneurysms as a high-risk, unstable type that often leads to rupture and requires early treatment.
Contribution
The paper formally defines ring-like aneurysms as a distinct subtype and highlights their pre-rupture instability.
Findings
All 16 reported ring-like aneurysms were large or giant with central thrombosis and a high rupture rate (37.5%).
Symptomatic presentation was common (62.5%), and posterior circulation involvement was observed in 44% of cases.
The study emphasizes the need for early endovascular treatment to prevent delayed rupture.
Abstract
Background/Objectives: “Ring-like” intracranial aneurysms—historically described as “doughnut-like” or “donut sign”—represent a rare configuration in which a central thrombus coexists with a circumferential mural flow ring. Traditionally considered a radiologic curiosity, this morphology likely reflects a shear-driven hemodynamic state rather than a stable organized thrombus. We aimed to summarize all PubMed-documented cases of ring-like aneurysms, define their morphologic and clinical spectrum, and assess their hemodynamic significance, rupture risk, and treatment outcomes. An additional aim is to formalize the use of the term “ring-like aneurysm” as a distinct morphologic subtype and to clearly differentiate it from the neuroradiologic “donut sign,” which represents an imaging appearance rather than a specific anatomic configuration. Methods: A systematic PubMed search (1996–2024) was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
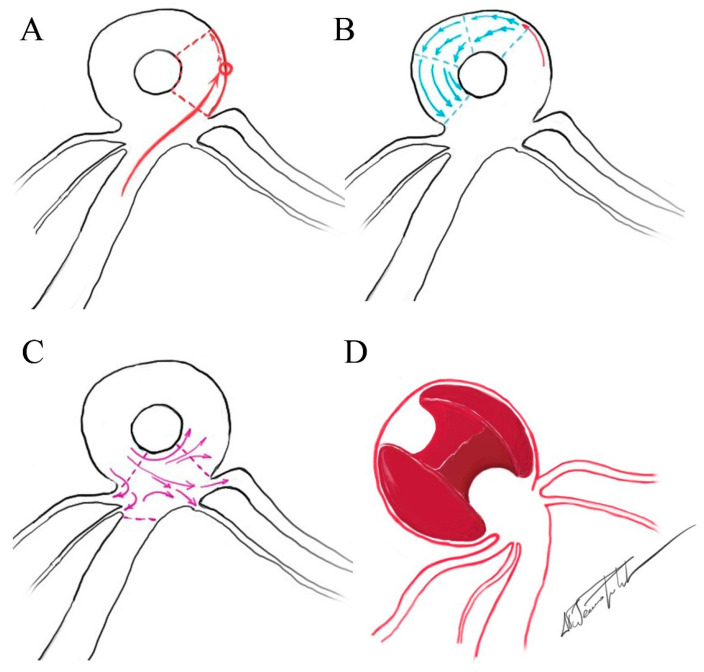 Figure 1
Figure 1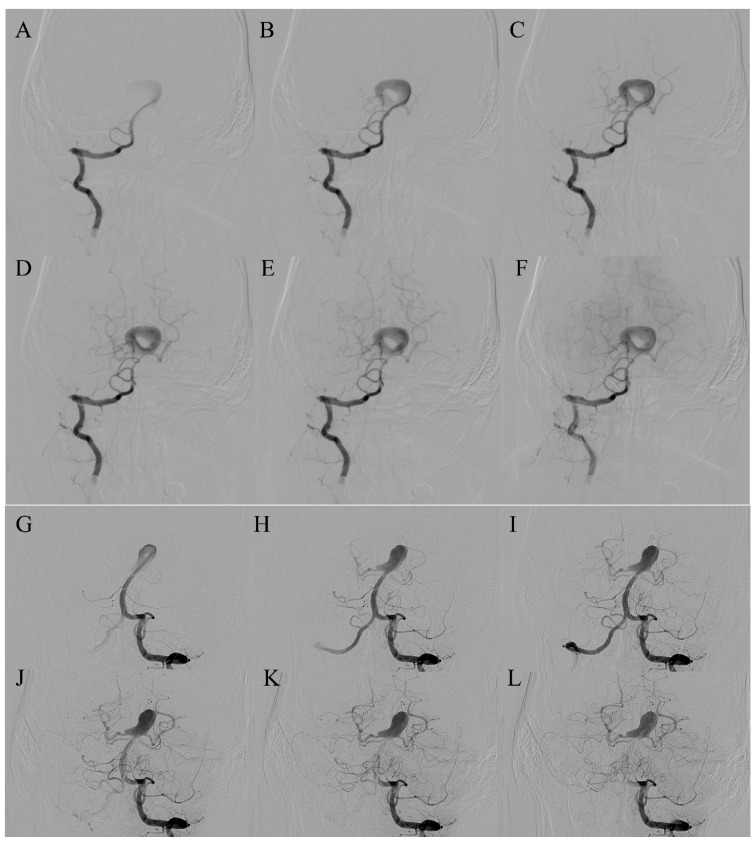 Figure 2
Figure 2 Figure 3
Figure 3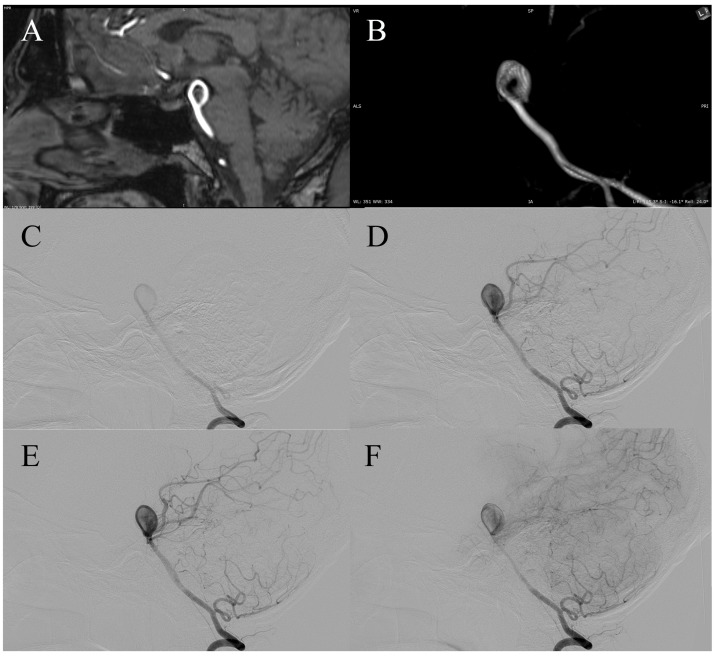 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Cerebral Venous Sinus Thrombosis · Intracerebral and Subarachnoid Hemorrhage Research
1. Introduction
The term “doughnut-like” aneurysm was first introduced by Ogawa et al. in 1996 [1], who described a partially thrombosed basilar tip aneurysm with a concentric flow lumen and central thrombus on 3-dimensional computed tomography angiography (3D-CTA) and digital subtraction angiography (DSA). This was the earliest recognition of the ring-shaped morphology—circumferential mural patency surrounding a central clot—that would later be referred to as the “donut sign” by van Rooij et al. eighteen years later [2]. Its reintroduction and subsequent popularization established the “donut sign” as a distinct imaging descriptor of partially thrombosed aneurysms. However, the “donut sign” should not be conflated with the ring-like aneurysm morphologic type. The “donut sign” denotes an imaging appearance that may also be observed in certain serpentine aneurysms [3] whereas the term “ring-like aneurysm” refers to a specific structural configuration. Despite its distinctive appearance, the morphologic boundaries and clinical significance of this configuration have not been clearly defined in the existing literature.
To address this ambiguity, the present study adopts the term ring-like aneurysm to denote an intracranial aneurysm with a circumferential residual lumen surrounding a central organized thrombus, in which inflow and outflow share a common neck. The objective is to consolidate all PubMed-documented cases, define the morphologic and clinical spectrum of ring-like aneurysms, and distinguish this entity from the neuroradiologic “donut sign.”
2. Materials and Methods
A systematic search of the PubMed database was performed for the period 1996–2024. The search used the following keyword combinations and Boolean operators: (“ring-like aneurysm” OR “donut aneurysm” OR “doughnut aneurysm” OR “ring-shaped aneurysm” OR “circumferential lumen” OR “central thrombus”) AND (“intracranial” OR “cerebral” OR “basilar” OR “aneurysm”). Reference lists of eligible publications were additionally screened to identify any secondary citations meeting inclusion criteria.
We included only PubMed-indexed, English-language reports that described true ring-like (donut-shaped) intracranial aneurysms characterized by a peripheral circumferential flow lumen surrounding a central thrombus. We excluded (1) non-indexed or non-English publications, (2) serpentine, fusiform, dolichoectatic, or partially thrombosed aneurysms that merely mimicked a ring-like configuration, and (3) reports lacking sufficient imaging or narrative detail to confirm a ring-like morphology.
For all included cases, we systematically extracted aneurysm location, maximal sac dimensions, clinical presentation (ruptured, symptomatic unruptured, or incidental), treatment modality (coiling, clipping, flow diversion, bypass, or conservative) and clinical outcomes. All data were independently verified by cross-referencing narrative descriptions with published imaging.
Descriptive statistics were used to summarize proportions across the pooled cohort. Rupture prevalence (SAH/ICH) and other categorical proportions were reported with Wilson 95% confidence intervals. A binomial test was used to compare the observed rupture prevalence with a conservative expected annual rupture risk derived from population-level data on large and giant intracranial aneurysms.
3. Results
Across the pooled cohort of 16 patients, 37.5% (6/16) presented with rupture (SAH or ICH), with a 95% confidence interval (CI) of 18.5–61.4%. Non-ruptured but symptomatic presentation accounted for 62.5% (11/16), corresponding to a 95% CI of 38.6–81.5%. All aneurysms in the series were large or giant (16/16; 100%), with a minimum sac diameter of ≥14 mm. A female predominance was observed (11/16; 69%), yielding an approximate female-to-male ratio of 2.2:1. Posterior circulation involvement was identified in 44% (7/16) of cases, with the basilar tip representing the most frequent location. Mortality analysis was performed on 15 evaluable patients, excluding the index case described by Ogawa et al. due to missing follow-up information. The overall mortality was 20% (3/15), with a 95% CI of 7.0–45.2%.
All publication cases were displayed in Table 1 chronologically.
4. Discussion
Although visually distinctive, the biological and hemodynamic significance of the ring-like configuration has remained insufficiently characterized. Subsequent reports have suggested that this morphology represents an active, shear-driven state rather than a stable, chronically organized thrombus [12,13,14]. This terminology emphasizes the hemodynamic nature of the configuration rather than a purely descriptive angiographic shape.
The angiographic “donut sign” [1] reflects wall-adjacent circulation and indicates persistent mural flow with central absence of contrast opacification. However, the “donut sign” is an imaging descriptor only, and may also be observed in certain serpentine aneurysms without implying the same underlying mechanism. In contrast, the ring-like aneurysm represents a dynamic flow-dependent state in which a focused, tangential inflow jet circulates along the aneurysm wall, maintaining a patent mural ring and preventing complete thrombosis [1,5,6].
4.1. Hemodynamic Interpretation
In the ring-like pattern aneurysms, shear-driven recirculation maintains flow along the mural ring while the central zone remains stagnant, causing gradual thrombus formation. Within its lumen, the flow architecture is tri-phasic, consisting of a focused inflow jet that impinges on the wall, a circumferential wall-adjacent recirculation zone that sustains the mural ring, and a progressively dispersed outflow stream that circulates towards the shared neck (Figure 1A). This hemodynamic arrangement may be consistent with the high rupture rate (37.5%) observed in pooled cases. To date, no prior publication has proposed a morphologic subdivision of ring-like aneurysms. We propose two reproducible patterns—bifurcation-type (Figure 2) and trunk-type (Figure 3)—each of which appears to be associated with characteristic circulation dynamics determined by the presence or absence of branching vessels. In trunk-type ring-like aneurysms, the lack of daughter branches creates a single inflow–outflow pathway through the common neck. Without lateral outflow, the contrast column remains within the sac for longer, resulting in more sustained intra-aneurysmal circulation and more pronounced flow complexity at the neck.
From a rheological perspective, blood within the ring-like lumen exhibits non-Newtonian behavior, where viscosity increases in low-shear regions and decreases in the high-shear mural layer. This shear-thinning property contributes to the maintenance of the peripheral jet, promoting persistent recirculation along the aneurysm wall while the central zone becomes progressively stagnant. The resulting architecture functionally forms a dual-compartment system—an outer, low-viscosity shear-maintained ring and an inner, high-viscosity thrombus core—forming a quasi-stable yet rupture-prone equilibrium [13,14]. Across the merged dataset, ring-like aneurysms show a markedly elevated rupture incidence compared with annual population estimates (1.6–6.5%) and even exceeding expected lifetime rupture risk (~30%). This may reflect a combination of larger aneurysm size, unique flow geometry, and case selection bias, but reinforces the distinctly high rupture potential that warrants clinical vigilance [15,16].
4.2. Dynamic Evolution of the Ring-like Configuration
The ring-like lumen is not a definitive anatomic subtype but a flow-dependent configuration sustained by shear-driven mural circulation. The “eaten apple-core” configuration of the central thrombus places its basal surfaces in direct contact with the aneurysm wall, exposing these regions to the same inflammatory, proteolytic, and hypoxic injury mechanisms described in large and giant partially thrombosed aneurysms [17,18,19,20]. In ring-like aneurysms, this mural weakening can further be compounded by the circumferential jet-inflow that courses along the wall, creating a dual pattern of biochemical and shear-related stress. The dynamic nature of this configuration is evident in both published and original cases. In the first case of the series by van Rooij et al. [2], a ring-like pattern emerged two weeks after stent implantation, indicating that altered inflow geometry and peripheralization of the jet can create a circumferential flow channel even when it is not initially present. In contrast, in Case 4 of our series [10], a clearly defined ring-like aneurysm was confirmed on diagnostic DSA, yet six weeks later, at the time of planned embolization, the entire outflow channel was no longer angiographically visible (Figure 2G–L). Case 5 further supports the dynamic nature of this morphology. On pre-procedural MRA, the aneurysm demonstrated a classic ring-like configuration with a central signal void corresponding to organized thrombus. However, diagnostic DSA performed several weeks later revealed almost complete recanalization of the aneurysmal sac, with faint residual central contrast opacification (Figure 4). This transformation indicates near-complete dissolution of the central thrombus and re-establishment of mural flow, underscoring that the “ring-like” appearance may fluctuate over short time intervals depending on the balance between shear-driven flow and intraluminal thrombus stability. These contrasting transformations show that the configuration appears to be governed by instantaneous hemodynamic conditions rather than by stable structural features. Dynamic changes in thrombus morphology should be interpreted not as direct indicators of rupture risk, but as evidence of underlying hemodynamic instability—an element that may contribute to the symptomatic and rupture behavior observed in reported cases.
4.3. Histopathology and Biology
Histologic and 7T MRI studies have reported that partially thrombosed aneurysms harbor vasa vasorum proliferation, inflammation, and intramural hemorrhage adjacent to the thrombus [12,14]. These biological processes weaken the wall, particularly in regions exposed to shear stress. The mural lumen in partially thrombosed aneurysms is therefore not inert, but a biologically active interface capable of enzymatic degradation and progressive wall thinning.
4.4. Clinical Implications
Radiologically, the ring-like configuration may be mistaken for stable thrombosis, but it should be interpreted as a hemodynamic warning. Cases in both adults and children confirm that ring-like aneurysms may rupture without warning [1,13]. Flow-diverter reconstruction represents a physiologically plausible approach: by suppressing tangential inflow and modifying wall-shear distribution, the device promotes gradual thrombosis and healing [7]. However, transient perianeurysmal edema may occur post-treatment, likely reflecting wall inflammation and thrombus reorganization [8,9,19,21,22,23]. In some instances, delayed rupture may develop either spontaneously or after incomplete hemodynamic exclusion, which may reflect insufficient thrombosis of the mural ring under persistent inflow stress [2,5]. These observations underscore the potential importance of early and complete endovascular reconstruction of the inflow zone.
4.5. Comparison with Serpentine Aneurysms
Serpentine aneurysms fundamentally differ in their flow architecture, which features separate inflow and outflow tracts and characteristically sluggish intra-aneurysmal flow. In contrast, ring-like aneurysms maintain a single neck with a focused, mural inflow jet—a configuration that, based on available case reports, appears to confer reduced stability and a higher propensity for rupture [1,2,4,7,14].
4.6. Demography and Localization
The female predominance observed in this pooled cohort mirrors the established gender distribution of intracranial aneurysms in general and therefore does not appear to be specific to the ring-like subtype. Ring-like aneurysms most frequently occur in the supraclinoid ICA and at the basilar apex-regions characterized by complex flow curvature and branching that may predispose to persistent mural ring flow [1,2,4,7,8,24].
4.7. Future Perspectives
Future work should combine patient-specific CFD with serial MRI and histologic correlation to better characterize shear-stress conditions associated with rupture risk [25]. Dedicated CFD simulations of ring-like aneurysms are warranted to characterize shear-stress heterogeneity within the mural ring and to identify hemodynamic patterns that may precede or contribute to rupture. Such modeling could help bridge the current gap between morphologic observation and quantitative hemodynamic analysis. Establishing a prospective registry of ring-like aneurysms may further clarify their natural history and treatment outcomes.
5. Conclusions
Ring-like aneurysms represent a reproducible and high-risk morphologic subtype within the spectrum of partially thrombosed intracranial aneurysms. The pooled rupture prevalence of 37.5% suggests that this configuration reflects an actively maintained, shear-dependent state rather than an end-stage thrombotic residue. The neuroradiologic “donut sign” may serve as a potential imaging indicator of an underlying jet-inflow pattern, reflecting persistent mural circulation and an active hemodynamic state associated with increased rupture risk. Early identification of this morphology and timely flow-modifying treatment may be important in preventing progression to rupture.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogawa T. Okudera T. Noguchi K. Sasaki N. Inugami A. Uemura K. Yasui N. Cerebral aneurysms: Evaluation with three-dimensional CT angiography AJNR Am. J. Neuroradiol.1996174474548881237 PMC 8337977 · pubmed ↗
- 2Van Rooij S.B. Bechan R.S. Markenstein J.E. Sluzewski M. Van Rooij W.J. The donut sign: A new angiographic sign for partially thrombosed aneurysms with flow-induced intraluminal thrombus Interv. Neuroradiol.201420555910.15274/INR-2014-1000924556300 PMC 3971142 · doi ↗ · pubmed ↗
- 3Ito H. Miyano R. Sase T. Wakui D. Matsumori T. Takasuna H. Oshio K. Tanaka Y. Outflow occlusion with A 3-A 3 anastomosis for a doughnut-shaped partially thrombosed giant A 2 aneurysm Surg. Neurol. Int.20167 S 1069 S 107110.4103/2152-7806.19637928144486 PMC 5234299 · doi ↗ · pubmed ↗
- 4Takeuchi S. Katoh H. Ishihara H. Yamada H. Wada K. Nawashiro H. Large doughnut-shaped internal carotid artery aneurysm Acta Neurol. Belg.201211223123210.1007/s 13760-012-0043-z 22426672 · doi ↗ · pubmed ↗
- 5Maingard J. Brooks M. ‘Donut’ basilar aneurysm with brainstem compression: Treatment using a flow diverting stent Interv. Neuroradiol.20162226626910.1177/159101991562691826842607 PMC 4984362 · doi ↗ · pubmed ↗
- 6Cholet C. Mathon B. Law-Ye B. Rare Intracranial Donut Aneurysm World Neurosurg.2017103950.e 1950.e 310.1016/j.wneu.2017.04.08828438651 · doi ↗ · pubmed ↗
- 7Lee C.H. Liao C.H. Chen W.H. Lee H.T. Tsuei Y.S. Angiographic doughnut-shaped aneurysm of intracranial internal carotid artery Acta Neurochir.201715972172410.1007/s 00701-017-3110-728188419 · doi ↗ · pubmed ↗
- 8Sgreccia A. Caragliano A. Sanfilippo G. Campa S. Trignani R. Giannoni M. De Nicola M. Consoli A. Rodesch G. Polonara G. Rare and Symptomatic Cavernous Donut-Shaped Aneurysm Treated by Flow Diverter Deployment World Neurosurg.201912122723110.1016/j.wneu.2018.09.21930312811 · doi ↗ · pubmed ↗