Evaluation of NTRK Fusions Detection Method in Esophageal Squamous Cell Carcinoma and Gastric Adenocarcinoma
Tomoyuki Momma, Motonobu Saito, Shotaro Nakajima, Katsuharu Saito, Erika Machida, Ken Miyabe, Yusuke Sato, Hiroyuki Hanayama, Hirokazu Okayama, Zenichiro Saze, Kosaku Mimura, Naoto Tsuchiya, Akiteru Goto, Kouya Shiraishi, Koji Kono

TL;DR
This study evaluates the effectiveness of using IHC and NGS to detect NTRK fusions in esophageal and gastric cancers, finding that NTRK fusions are rare in these cancers.
Contribution
The study confirms the rarity of NTRK fusions in esophageal and gastric cancers and highlights the limitations of IHC screening for TRK protein.
Findings
TRK protein was expressed in 10 out of 254 ESCC cases but none of the 401 GC cases.
NGS and FISH analyses found no NTRK fusions in the TRK-positive ESCC cases.
In silico analysis confirmed the low prevalence of NTRK fusions in these cancers.
Abstract
Neurotrophic tyrosine receptor kinase (NTRK) fusions function as oncogenes and have been targeted by TRK inhibitors with excellent clinical outcomes. The international expert consensus recommends immunohistochemical (IHC) screening for TRK protein followed by next generation sequencing (NGS) to measure expression of NTRK fusions for tumors with low NTRK fusion expression. To confirm the clinical utility of this recommendation in esophageal and gastric cancers, total TRK protein expression was measured by IHC using anti-pan-TRK antibody in 254 esophageal squamous cell carcinoma (ESCC) and 401 gastric adenocarcinoma (GA) samples. Subsequently, DNA-based NGS and fluorescence in situ hybridization (FISH) were performed for tumors expressing TRK to measure NTRK fusion expression. Further, expression of NTRK fusions was evaluated in esophageal and gastric cancers using public databases. IHC…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
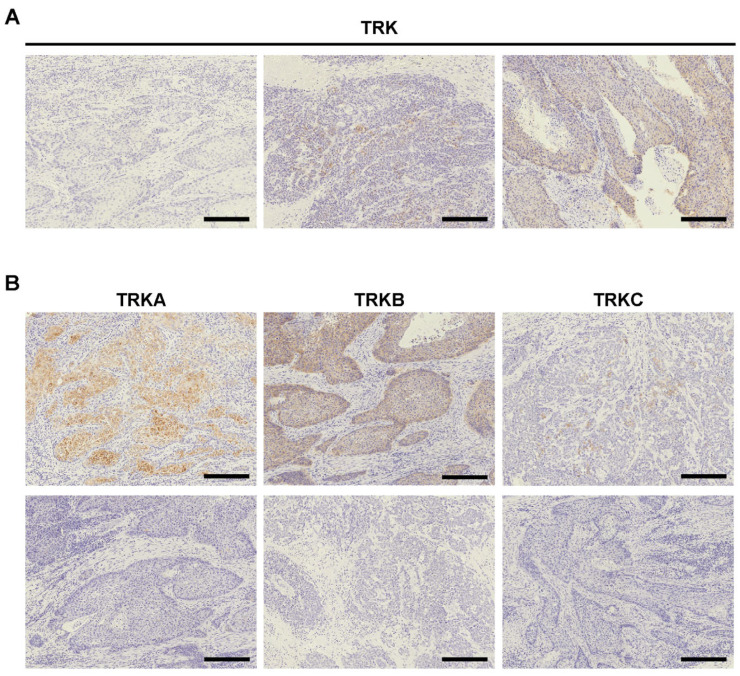 Figure 1
Figure 1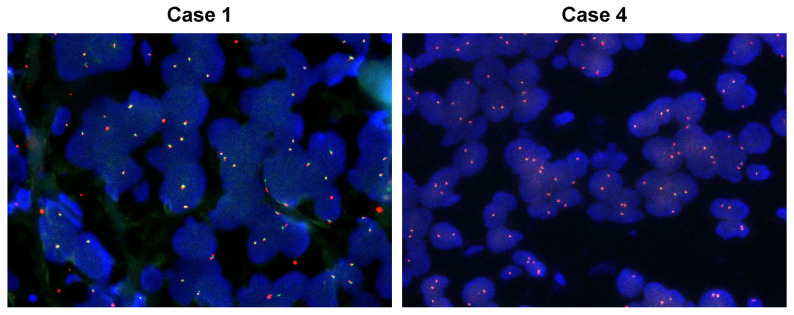 Figure 2
Figure 2- —Japan Society for the Promotion of Science (JSPS) KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Cancer, Stress, Anesthesia, and Immune Response · Wnt/β-catenin signaling in development and cancer
1. Introduction
Neurotrophic tyrosine receptor kinase (NTRK) genes consist of three isoforms, NTRK1, NTRK2, and NTRK3, and encode a family of tropomyosin receptor kinases (TRK), including TRKA, TRKB, and TRKC, respectively [1]. TRK proteins are physiologically expressed in the central and peripheral nervous system, and comprise the receptor tyrosine kinase family of neurotrophin receptors [1]. Among gene aberrations occurring in NTRK, the most significant oncogenic aberration is gene fusion that continually activates TRK receptors, causing constitutive activation of downstream oncogenic signaling [1,2]. This oncogenic activation leads to phosphorylation of the TRK protein, and the efficacy of tyrosine kinase inhibiters (TKI) is widely recognized, along with ALK, RET, and ROS1 fusions [3]. In NTRK fusion-positive cancers, larotrectinib and entrectinib have demonstrated excellent clinical outcomes [4,5].
While NTRK fusions are rarely detected in common cancers, they are highly prevalent in rare cancers, such as secretory breast carcinoma, mammary analog secretory carcinoma, adult and infantile congenital fibrosarcoma, and pediatric cellular and mixed congenital mesoblastic nephroma [1]. In gastrointestinal tract cancers, NTRK fusions are relatively highly detected in gastrointestinal stromal tumor (GIST), primarily in cases without KIT, PDGFRA, or RAS mutations, and in colorectal cancer, most frequently in Microsatellite Instability (MSI)-high tumors [1,6,7]. On the other hand, The Cancer Genome Atlas (TCGA) and FoundationCORE databases suggest NTRK fusions are rarely present in esophageal and gastric cancers [8,9].
To detect NTRK fusions, immunohistochemical (IHC) staining, fluorescence in situ hybridization (FISH), RT-qPCR, and both RNA- and DNA-based next generation sequencing (NGS) are performed [10,11]. Although NGS is the definitive means for detection of NTRK fusions, it is not feasible to routinely perform this advanced analysis in all patients. Therefore, the international expert consensus recommends IHC screening for TRK expression followed by NGS analysis to measure expression of NTRK fusions in TRK^+^ (positive) cases [10,12]. Importantly, the positivity rate of TRK staining is different between studies, possibly due to differences in patient demographics and antibodies for used IHC staining. For example, a prior report used TCGA data from Caucasian populations to identify that NTRK fusions were not detected in any of the analyzed esophageal squamous cell carcinoma (ESCC) or gastric adenocarcinoma (GA) cases [9]. In addition, very few ESCC or GA cases from Caucasian populations were identified as TRK^+^ by IHC staining with the anti-pan-TRK antibody [13,14]. Seemingly in contrast, other studies reported that 20–65% of GA cases from Asian populations expressed TRKs using IHC staining with anti-TRKA, TRKB, or TRKC antibodies [15,16]. Therefore, the practical utility of the consensus-recommended screening method must be further evaluated in esophageal and gastric cancers.
In the present study, we measured TRK positivity by IHC staining using a pan-TRK antibody in ESCC and GA samples from Asian populations (Japanese). Subsequently, NGS or FISH was performed on TRK^+^ cases to measure expression of NTRK fusions. We further discuss the utility of NTRK fusion screening methods for esophageal and gastric cancer in the context of present and prior findings.
2. Results
2.1. TRK Expression in ESCC and GA
We first performed IHC staining for TRK (pan-TRK), TRKA, TRKB, and TRKC in our cohort, which included 254 ESCC and 401 GA tumors (Figure 1, Table 1 and Table 2, and Supplemental Figure S1). The GA cohort included 27 (6.7%) EBV (+) cases and 33 (8.2%) dMMR GA cases. IHC staining for pan-TRK revealed that among ESCC cases, ten cases were weakly or moderately positive for TRK expression (Table 3). When comparing clinicopathological factors between TRK^+^ and TRK^−^ ESCC cases, no significant findings were observed. Contrastingly, no TRK^+^ cases were detected in the GA study cohort. IHC staining for TRKA, TRKB, and TRKC for the ten TRK^+^ ESCC cases, positive expression for at least one of these antibodies was detected. Because TRKA and TRKB staining was positive in most of our cases including those with negative staining for the pan-TRK antibody, it is worthy to note that using antibodies for TRKA or TRKB could overestimate cases potentially harboring NTRK fusions, which is consistent with a previous report [17]. In conclusion, ten ESCC cases showedpositive TRK expression, but none of the GA cases were selected for confirmation analysis to detect NTRK fusions.
2.2. Confirmation of NTRK Fusion in TRK+ ESCC Cases
Ten TRK^+^ ESCC cases were deemed to potentially harbor NTRK fusions by IHC screening, and they were subjected to DNA-based NGS analysis known as the NCC Oncopanel. Due to the poor quality of the DNA extracted from FFPE samples, sequencing data were obtained from eight out of ten ESCC cases. As a result, none of NTRK1 or NTRK2 fusions were detected in the sequenced ESCC cases. Because NTRK3 is not included in the NCC Oncopanel, we performed FISH to detect NTRK3 fusions (Figure 2). After confirming the validity of the experimental methodology using a NTRK1 fusion positive case, we confirmed that none of NTRK3 fusions were detected in the ten TRK^+^ ESCC cases (Table 3 and Supplemental Figure S2). In addition, no NTRK aberrations, including amplification, were identified in the sequenced ESCC cases. All gene alterations detected in ESCC cases were listed, and the lack of NTRK mutation or copy number alterations was confirmed (Table 4 and Supplementary Table S1).
2.3. Database NTRK Fusion Detection
Next, we summarized the prevalence of patients with esophagogastric cancer harboring NTRK fusions using the TCGA database (n = 3960), and we included esophageal cancer (n = 1476, 968 adenocarcinoma and 508 squamous cell carcinoma), esophagogastric cancer (n = 528 with 140 adenocarcinoma and 388 unknown histology), gastroesophageal junction cancer (n = 268, all adenocarcinoma), and gastric cancer (n = 1672, all adenocarcinoma) (Table 5). Three cases (0.08%, n = 3/3960) expressing NTRK1 fusions (RRP15-NTRK1, NAV1-NTRK1, and one case with both PEAR1-NTRK1 and NTRK1-STK11 fusions) were detected in esophagogastric adenocarcinoma (esophageal, esophagogastric, or gastroesophageal junction). However, NTRK fusions were not detected in patients with ESCC or GA from Western populations. Contrastingly, the China Pan-cancer study (n = 10194) revealed that two of 582 (0.3%) ESCC cases and seven of 850 (0.8%) GA cases from Asian populations expressed NTRK fusions (Table 5). The fusion partner of NTRK3 detected in the China Pan-cancer study is not a common partner detected in other adult NTRK3 fusion-positive tumors [1,17]. Consistently, a recent real-world data study using cancer comprehensive genomic profiling testing (FoundationOne CDx) further confirmed that NTRK fusions are rarely detected in esophageal (0.24%) and gastric (0.16%) cancers [8].
3. Discussion
In the present study, we demonstrated that in our cohort of ESCC and GA cases, only ten ESCC cases, and no GA cases, were TRK^+^ on initial IHC screening, and that none of the TRK^+^ ESCC cases subjected to NGS analysis or FISH expressed NTRK fusions. The TCGA study revealed that other than the PEAR1-NTRK1 fusion, which has been detected in patients with breast cancer and sarcoma [17,18], NTRK fusions identified in esophageal and gastric cancers are not common mutations. In the TCGA study of Western populations, NTRK fusions were detected in patients with esophageal adenocarcinoma and gastroesophageal junction adenocarcinoma but were not detected in ESCC or GA cases. On the other hand, in the TCGA study of Asian populations, NTRK fusions were detected in patients with ESCC and GA but were not detected in esophageal adenocarcinoma patients. A case report from Japan described a patient with GA harboring the ATP1B-NTRK1 fusion, which is also a less common fusion. The ATP1B-NTRK1 fusion is not listed in other cancers of the TCGA database [19]. Because adenocarcinoma is the most common type of esophageal cancer in Western populations, while squamous cell carcinoma is more common in Asian populations, NTRK fusions might not be detected in the small number of Asian patients with esophageal adenocarcinoma [20]. Furthermore, since the overall prevalence of NTRK fusion-positive tumors was relatively high in patients with Asian ancestry (0.40%) compared to patients with European ancestry (0.28%), this could have influenced the finding that NTRK fusions were more likely to be detected in Asian populations [8]. However, since NTRK fusions are extremely rare in ESCC and GA even among Western or Asian populations from the database analyses, it is challenging to study NTRK fusions, and this has become a limitation in the research.
The European Society for Medical Oncology (ESMO) established a practical guideline to detect NTRK fusions using the molecular diagnosis methods available in daily practice [10]. Although an NGS assay for NTRK1, NTRK2, and NTRK3 is the confirmatory method, the performance of NGS analysis for unselected patients is uncommon due to limited NGS access in clinical settings. For tumor types with a high incidence of NTRK fusions, FISH, RT-PCR, or RNA-based NGS are recommended to determine if NTRK fusions are present. On the other hand, in tumors with low incidence of NTRK fusions, TRK detection with IHC screening followed by NGS analysis for detecting NRTK fusions is recommended. In the present study, a pan-TRK antibody (EPR17341), which has already been confirmed to be highly sensitive and specific to NTRK fusions, was used for IHC screening [11]. Prior studies reported that while TRK expression was observed in gastric gland and tumor-adjacent nerve tissue, TRK was not expressed in the tumor component among 372 Caucasian GA cases [13]. Another study also reported that 7 out of 477 GA tumors were identified as TRK^+^ by IHC, but no NTRK fusions were detected by NGS [14]. Furthermore, even though 1 of 66 GA tumors were TRK^+^ by IHC, and the break-apart of NTRK1 was confirmed by FISH, NTRK1 fusions were not confirmed by NGS [21]. Importantly, these reports demonstrated that even when positive IHC staining for TRK was detected in ESCC and GA tumors, none of NTRK fusions was confirmed by NGS [13,14,21]. A parallel analysis using anti-TRKA, anti-TRKB and anti-TRKC antibodies revealed that positive TRKA and TRKB staining was more frequently detected than anti-pan-TRK staining in ESCC. Based on the NGS finding that none of the TRK^+^ cases harbored NTRK fusions, IHC screening with antibodies against TRKA or TRKB could produce relatively high false-positive rates for NTRK fusions. Most importantly, since IHC staining for TRK was also negative in our positive control of NTRK1 fusion-positive esophageal cancer, IHC screening may require further consideration. In conclusion, consistent with previous reports indicating that IHC staining has limited utility as a biomarker for detecting tumors harboring NTRK fusions, awaiting the development of more reliable antibodies may help reduce the time and financial burden associated with identifying false-negative NTRK fusion cases through NGS [22].
It should be noted that NTRK amplifications also induce increased TRK expression, and the prevalence of NTRK amplifications has been reported to be 0.48% of AACR GENIE cases, including various types of cancers [23]. While we did not identify NTRK amplifications in our ESCC cases, analysis of the TCGA database demonstrated that only one GA case from Asian populations harbored NTRK1 amplifications. NTRK1 is located at 1q23.1, and an increased copy number involving that site is considered a potential oncogenic alteration in patients with malignant melanoma and hepatocellular carcinoma, but gene amplification including 1q23.1 is not a common structural variant in esophageal or gastric cancers [24,25].
In this study, NTRK fusions are rarely detected in patients with ESCC or GA from Asian populations, and the analyses were reconfirmed. Because ESCC and GA are verified to be tumors with low incidence of NTRK fusions, IHC screening followed by NGS confirmation is recommended for detection of NTRK fusions. However, IHC staining for TRK could include many false-positive cases, confirmation by NGS would be required prior to considering treatment with TRK inhibitors. The implementation of IHC testing for tumor with low NTRK fusion positivity rates may be justified when using TRK antibodies that demonstrate high positive predictive values for TRK. So far, direct NGS testing would likely be indicated only for tumors with high NTRK fusion positivity rates.
4. Materials and Methods
4.1. Patients
The study included 254 ESCC and 401 GA specimens from patients who underwent surgical resection at Fukushima Medical University Hospital between 2002 and 2021. All cases have been used in our previous studies, and basic characteristics were previously documented [26,27,28]. GA samples were previously subjected to Epstein-Barr virus-encoded small RNA (EBER) ISH to determine EBV infection status and IHC staining for the mismatch repair (MMR) proteins MLH1, MSH2, MSH6, and PMS2 [29]. Data on age, sex, TNM stage (an updated standard for staging cancer, focusing on Tumor (T), Node (N), and Metastasis (M), 8th classification), and pathological diagnosis were retrospectively collected. The carcinomas at the time of primary tumor resection were staged according to the guidelines set forth by the Union for International Cancer Control classification. The study was approved by the ethics committee of Fukushima Medical University (Protocol No. 2367 in 2016 initial approval and REC2024-041 in 2024 renewal, 24 January 2025). For the use of previously collected specimens, the approved research protocol was disclosed in accordance with relevant guidelines, and patients were given the opportunity to opt out. For the prospective collection of specimens, written informed consent was obtained from all participants. All experiments were conducted in accordance with the approved study plan and relevant guidelines.
4.2. Immunohistochemical Staining and Evaluation
IHC staining was performed using the polymer peroxidase method with formalin-fixed, paraffin-embedded (FFPE) histology sections (4 μm thick), as described previously [29]. Briefly, the sections were treated for deparaffinization and rehydration, then endogenous peroxidase activity was blocked using 0.3% hydrogen peroxide. After rinsing in PBS, the sections were incubated with ananti-pan-TRK antibody (#EPR17341; 1:50 dilution; Abcam, Cambridge, UK), anti-TRKA antibody (#2510; 12G8; 1:400 dilution; Cell Signaling Technology, Danvers, MA, USA), anti-TRKB antibody (#4607; 80G2; 1:2000 dilution; Cell signaling Technology), or anti-TRKC antibody (#3376; C44H5; 1:1000 dilution; Cell Signaling Technology) at 4 °C overnight. Incubation was performed by a peroxidase-labeled polymer conjugated to goat antirabbit immunoglobulins (ENvision + kit; Dako, Agilent, Santa Clara, CA, USA) as the secondary antibody for 30 min at room temperature, after the PBS wash. For visualization, diaminobenzidine staining was performed, followed by counterstaining with hematoxylin and eosin (H&E). TRK positivity was calculated as the percentage of positive staining cancer cell and defined as negative, 0%; weak positive, <1%; moderate positive, 1–10%; and strong positive, 11–100%, as previously described [29].
4.3. Next Generation Sequencing
NGS analysis was performed using the NCC Oncopanel, as described previously [30]. Briefly, extracted genomic DNA from theFFPE section was prepared for sequencing libraries using SureSelect XT reagent (Agilent Technologies, Santa Clara, CA, USA) and a KAPA Hyper Prep kit (KAPA Biosystems, Wilmington, MA, USA). Subsequently, samples were analyzed on the Illumina NextSeq platform (Illumina, San Diego, CA, USA) with 150 bp paired-end reads. The NCC Oncopanel test is a hybridization capture-based NGS assay designed to examine mutations, amplifications, and homozygous deletions of the entire coding region of 124 genes of clinical or preclinical relevance, together with rearrangements of 13 oncogenes, NTRK1,and NTRK2, included in the panel.
After the adapter sequences using the Cutadapt program was removed, the obtained result of the was mapped to the human reference genome Burrows–Wheeler Aligner and the Smith–Waterman algorithm The cisCall program (version 7.1.5) was used for detected somatic mutations (single nucleotide variants (SNV) and short insertions and deletions (Indels)), copy number amplifications (CNV), and rearrangement (homozygous deletions and fusions). Somatic mutations were selected using the previously described criteria using the NHLBI GO Exome Sequencing Project (ESP6500) (http://evs.gs.washington.edu/EVS/) (accessed on 29 June 2019) or the Integrative Japanese Genome Variation Database (iJGVD, 20181105) (https://ijgvd.megabank.tohoku.ac.jp/) (accessed on 29 June 2019) to remove single nucleotide polymorphisms (SNPs) [30]. Mutations were classified as “pathogenic/likely pathogenic variants” in ClinVar or “oncogenic/likely oncogenic variants” in the OncoKB (http://oncokb.org) databases using oncokb-annotatorand commit 8910b65 (accessed on 29 June 2019). Amplifications with >4-fold copy number increases were defined as positive, and genes with <0.5-fold copy number decreases were defined as homozygous deletion candidates. Somatic mutation and amplification were determined using the Integrative Genomics Viewer (IGV; http://www.broadinstitute.org/igv/ accessed on 29 June 2019).
4.4. FISH
FISH analysis of formalin-fixed, paraffin-embedded (FFPE) histology sections (10 μm thick) was performed using the ZytoLight SPEC NTRK3 Dual Color Break Apart Probe (PL164) (ZytoVision GmbH, Bremerhaven, Germany), according to the manufacture’s information. Slides were evaluated for break-apart signals of cancer cells under the fluorescent microscope (Nikon Eclipse Ci with fluorescence LED illumination system D-LEDI) (Nikon, Tokyo, Japan) independently by two pathologists (K. Miyabe and A. Goto) who were blinded to the patient’s history and histological findings.
4.5. Database Analysis
Gene change data of patients with esophageal and gastric cancer including the expression of NTRK fusions were obtained from the TCGA cBioPortal database (http://www.cbioportal.org/). NTRK1, NTRK2, and NTRK3 data were used for the analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cocco E. Scaltriti M. Drilon A. NTRK fusion-positive cancers and TRK inhibitor therapy Nat. Rev. Clin. Oncol.20181573174710.1038/s 41571-018-0113-030333516 PMC 6419506 · doi ↗ · pubmed ↗
- 2Amatu A. Sartore-Bianchi A. Bencardino K. Pizzutilo E.G. Tosi F. Siena S. Tropomyosin receptor kinase (TRK) biology and the role of NTRK gene fusions in cancer Ann. Oncol.201930 viii 5viii 1510.1093/annonc/mdz 38331738427 PMC 6859819 · doi ↗ · pubmed ↗
- 3Saito M. Shiraishi K. Kunitoh H. Takenoshita S. Yokota J. Kohno T. Gene aberrations for precision medicine against lung adenocarcinoma Cancer Sci.201610771372010.1111/cas.1294127027665 PMC 4968599 · doi ↗ · pubmed ↗
- 4Drilon A. TRK inhibitors in TRK fusion-positive cancers Ann. Oncol.201930 viii 23viii 3010.1093/annonc/mdz 28231738426 PMC 6859818 · doi ↗ · pubmed ↗
- 5Marcus L. Donoghue M. Aungst S. Myers C.E. Helms W.S. Shen G. Zhao H. Stephens O. Keegan P. Pazdur R. FDA Approval Summary: Entrectinib for the Treatment of NTRK gene Fusion Solid Tumors Clin. Cancer Res.20212792893210.1158/1078-0432.CCR-20-277132967940 · doi ↗ · pubmed ↗
- 6Yamashiro Y. Kurihara T. Hayashi T. Suehara Y. Yao T. Kato S. Saito T. NTRK fusion in Japanese colorectal adenocarcinomas Sci. Rep.202111563510.1038/s 41598-021-85075-y 33707574 PMC 7952565 · doi ↗ · pubmed ↗
- 7Atiq M.A. Davis J.L. Hornick J.L. Dickson B.C. Fletcher C.D.M. Fletcher J.A. Folpe A.L. Marino-Enriquez A. Mesenchymal tumors of the gastrointestinal tract with NTRK rearrangements: A clinicopathological, immunophenotypic, and molecular study of eight cases, emphasizing their distinction from gastrointestinal stromal tumor (GIST)Mod. Pathol.2020341910.1038/s 41379-020-0623-z 32669612 · doi ↗ · pubmed ↗
- 8Westphalen C.B. Krebs M.G. Le Tourneau C. Sokol E.S. Maund S.L. Wilson T.R. Jin D.X. Newberg J.Y. Fabrizio D. Veronese L. Genomic context of NTRK 1/2/3 fusion-positive tumours from a large real-world populationnpj Precis. Oncol.2021569 Correction in npj Precis. Oncol. 2021, 5, 8610.1038/s 41698-021-00206-y 34285332 PMC 8292342 · doi ↗ · pubmed ↗