Levels of Cu, Zn, and Se in Maternal and Cord Blood in Normal and Pathological Pregnancies: A Narrative Review
Radomir Aničić, Dejan Mihajlović, Jovana Kocić, Jovana Jagodić, Aleksandar Stojsavljević

TL;DR
This review explores how copper, zinc, and selenium levels in maternal and cord blood affect pregnancy outcomes and fetal development.
Contribution
This is the first global narrative review to examine Cu, Zn, and Se levels in maternal and cord blood and their associations with adverse pregnancy outcomes.
Findings
Levels of Cu, Zn, and Se in maternal and cord blood vary globally and across pregnancy trimesters.
Abnormal levels of these elements are linked to preterm birth, preeclampsia, and other adverse outcomes.
The review suggests optimal maternal levels of Cu, Zn, and Se for healthy pregnancies.
Abstract
Copper (Cu), zinc (Zn), and selenium (Se) play a pivotal role in pregnancy. Both a deficiency and an excess of Cu, Zn, and Se have deleterious consequences for the outcome of pregnancy. Accordingly, maintaining optimal levels of circulating Cu, Zn, and Se is critical for proper fetal growth and development. However, to our knowledge, this is the first narrative global review that not only summarizes Cu, Zn, and Se levels in maternal and cord blood but also examines their associations with multiple adverse pregnancy outcomes. Thus, this up-to-date review seeks to address these key questions. To achieve these goals, literature was collected from the past several decades from three relevant databases (PubMed, Scopus, and Cochrane Library), and rigorous exclusion and inclusion criteria were set for peer-reviewed studies that met the requirements for a final inclusion in the review analysis.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
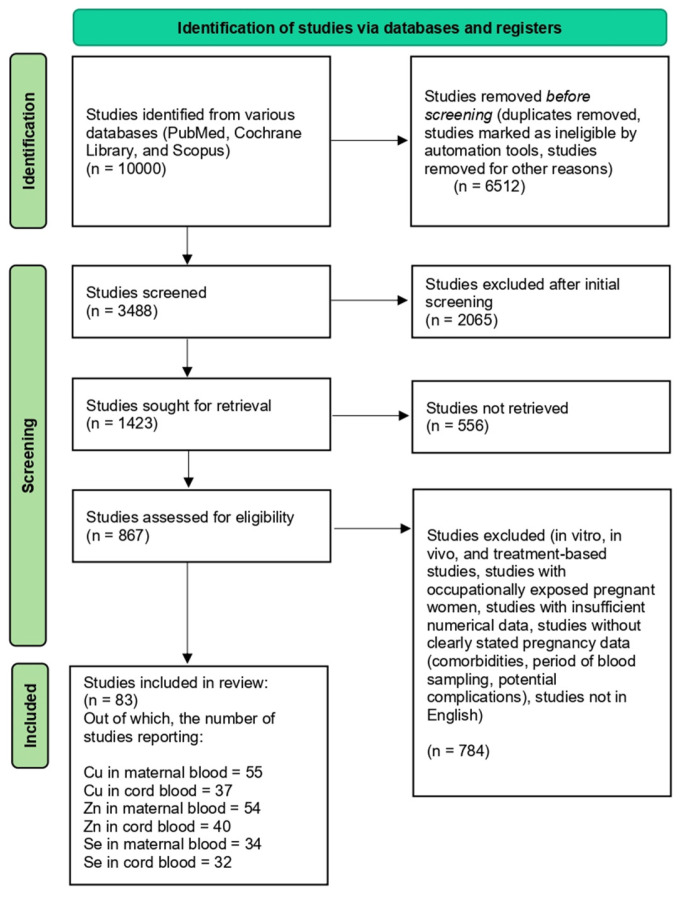 Figure 1
Figure 1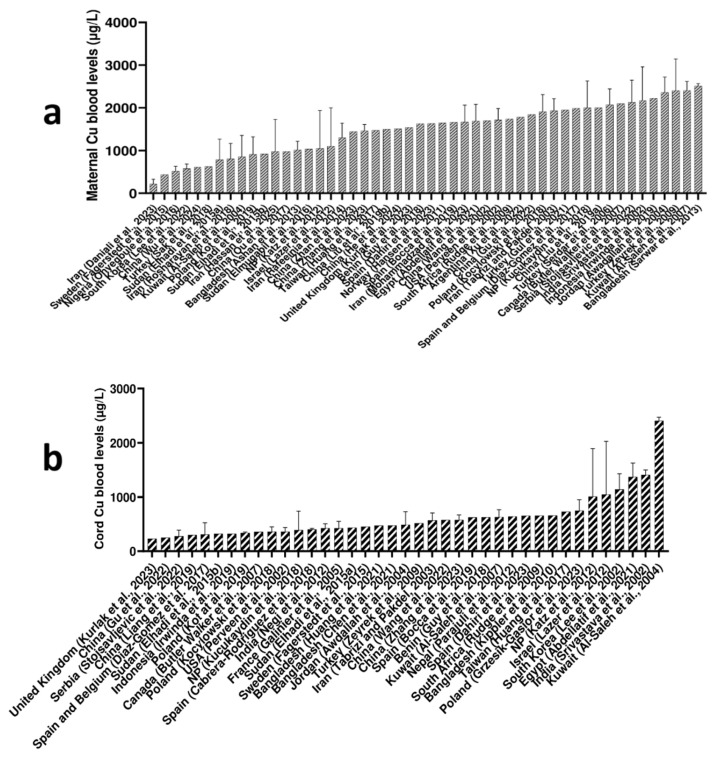 Figure 2
Figure 2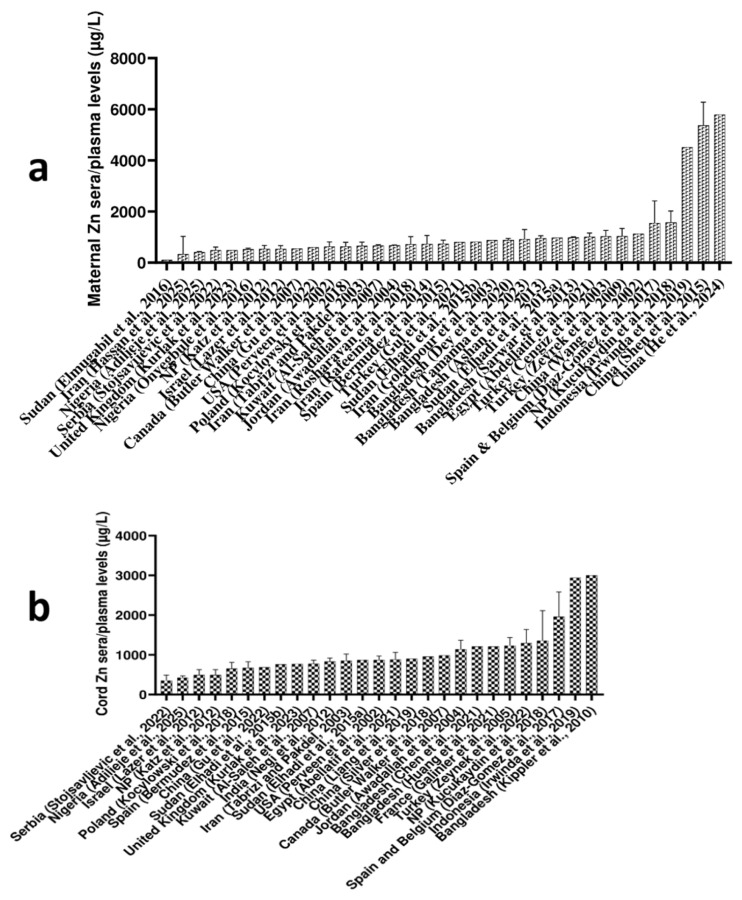 Figure 3
Figure 3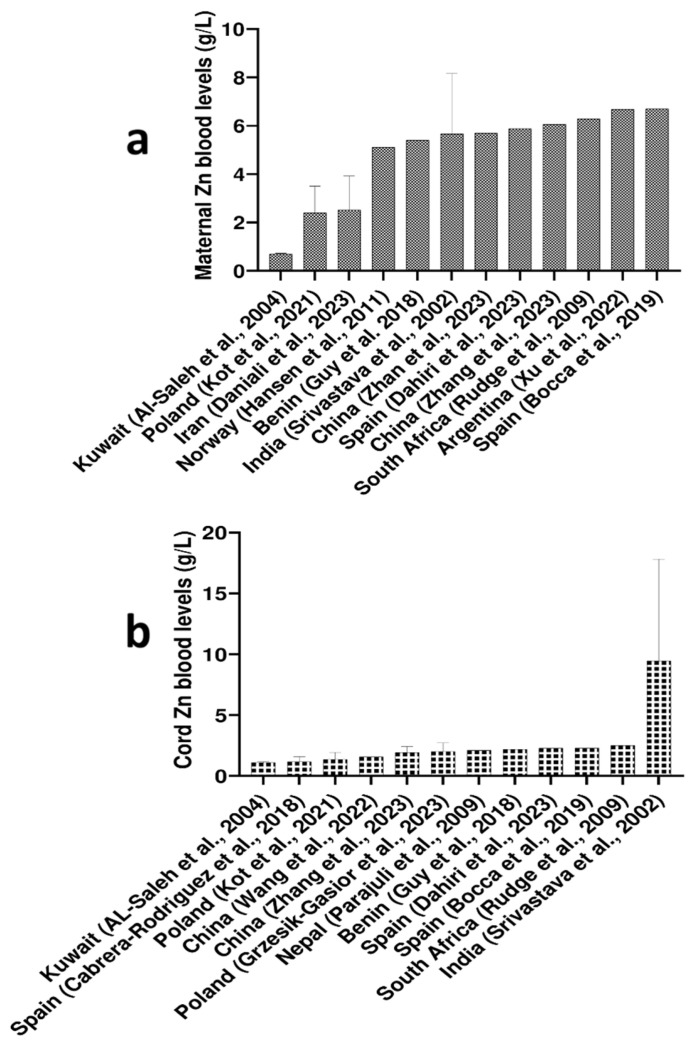 Figure 4
Figure 4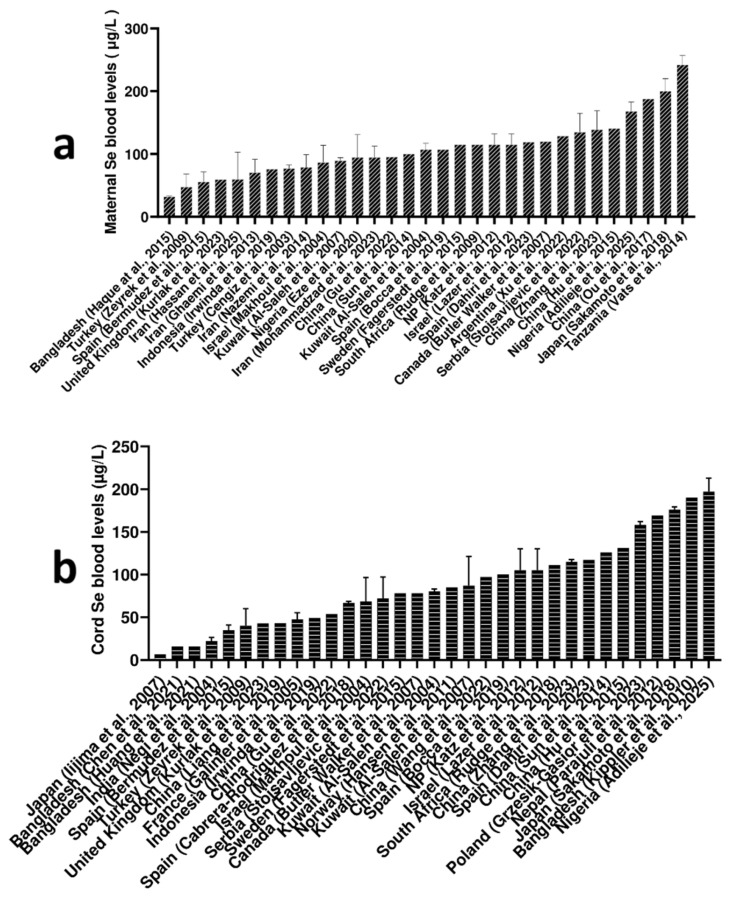 Figure 5
Figure 5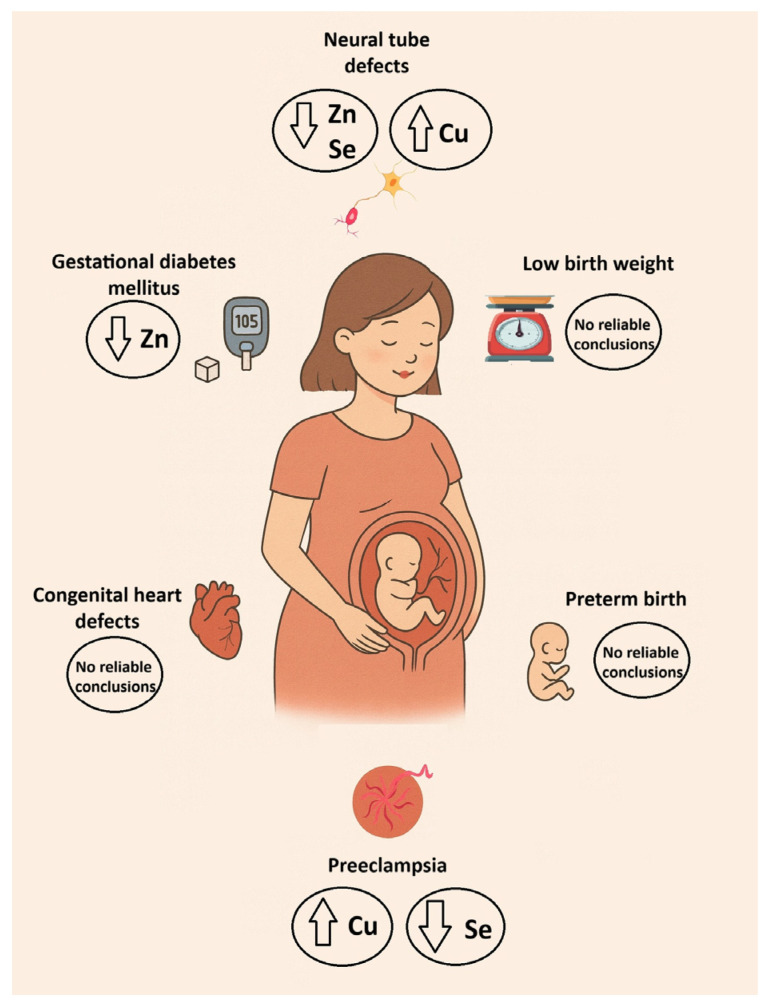 Figure 6
Figure 6- —Ministry of Science, Technological Development, and Innovation of the Republic of Serbia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrace Elements in Health · Heavy Metal Exposure and Toxicity · Pregnancy and Medication Impact
1. Introduction
The total amount of trace elements makes up 0.01% (per dry weight) of the human body. Most trace elements are not essential for humans; in fact, even low levels of most trace elements have detrimental effects on human health [1]. Essential trace elements for humans are iron (Fe), copper (Cu), zinc (Zn), manganese (Mn), chromium (Cr^3+^), cobalt (Co), iodine (I), molybdenum (Mo), and selenium (Se) [2]. Essential trace elements are key nutrients that cannot be synthesized in the human body [3]. A lack of essential trace elements can lead to serious disruptions in the functioning of the body and even death [4]. On the other hand, an excess of an essential trace element also disrupts the body’s homeostasis and leads to numerous disorders, including cancer [5].
Pregnancy is a physiologically altered state in females characterized by an increased need for essential nutrients [6]. Copper, Zn, and Se are pivotal trace elements whose balance is necessary for normal pregnancy [7]. Consequently, disturbed levels of these trace elements could have a pathological outcome for a pregnancy [8]. According to the European Food Safety Agency (EFSA), adult women generally need 1.3 mg of Cu per day. During pregnancy, it is necessary to intake 1.5 mg of Cu per day [9]. The daily requirement for Zn is 8 mg/day for adult women. However, during pregnancy, a higher intake of Zn is recommended, 11 mg/day [10]. Adult women, including pregnant women, need 70 µg of Se per day [11]. According to the American College of Gynecologists and Obstetricians (ACOG), these amounts of Cu, Zn, and Se are usually met through a balanced diet. Still, in certain cases, supplementation can be necessary [12].
Numerous studies have examined high or low levels of essential trace elements in pregnancy. Thus, high blood levels of Cu are associated with low birth weight (LBW), preterm birth (PTB), and spontaneous abortions [13]. Low levels of blood Cu are associated with increased risks of miscarriage and PTB [14]. High blood levels of Zn can be lethal for the fetus, while low blood Zn levels are associated with preeclampsia (PE), LBW, PTB, etc. [15]. Selenium plays a dominant role in preventing oxidative stress, increasing the body’s antioxidant capacity in synergy with vitamin E and other antioxidants. This support effectively helps maintain the body’s homeostasis, particularly during pregnancy [16]. High blood Se levels are associated with an increased risk of congenital heart defects (CHDs). Low blood Se levels during pregnancy are associated with several complications, including gestational hypertension, gestational diabetes mellitus (GDM), preterm birth, miscarriage, and LBW [17]. However, some studies indicate that the available evidence is still inconclusive regarding the impact of these trace elements on the conditions mentioned above [18].
In this narrative review, the aim was to present data on the levels of Cu, Zn, and Se in maternal and cord blood worldwide, the elemental differences between maternal and cord blood, the fluctuations of their blood levels depending on the trimester of pregnancy, and differences in Cu, Zn, and Se levels between arterial and venous cord blood. An additional aim was to present key findings on the effects of Cu, Zn, and Se on birth weight and PTB, PE, GDM, neural tube defects (NTDs), and CHDs.
To resolve these goals, literature was collected from the past two and a half decades (from January 2000 to July 2025) from three relevant databases (PubMed, Scopus, and Cochrane Library), and rigorous exclusion/inclusion criteria were set for peer-reviewed studies that met the conditions for final inclusion in our review analysis. Studies were eligible for inclusion if they were peer-reviewed, reported original data, and assessed Cu, Zn, or Se levels in maternal and/or cord blood, with or without relevant clinical outcomes. Furthermore, they were assessed if they reported any of the following outcomes: birth weight, preterm birth, pre-eclampsia, gestational diabetes mellitus, neural tube defects, or congenital heart defects. Excluded articles encompassed letters, conference abstracts, commentaries, studies lacking trace element measurements, and publications without an accessible full text. All records were screened in two stages: title/abstract and full-text review, according to predefined eligibility criteria. Two reviewers independently screened studies, and discrepancies were resolved through discussion or consultation with a third reviewer. The overall study selection process, including the number of records identified, screened, excluded, and included, is documented in the PRISMA flow diagram (Figure 1). Search strategies were developed using combinations of controlled vocabulary (e.g., MeSH terms) and free-text keywords related to trace elements and pregnancy outcomes. The search terms included variations of: “copper,” “zinc,” “selenium,” “maternal blood,” “cord blood,” “pregnancy,” “trimester,” “birth outcomes,” “preterm birth,” “pre-eclampsia,” “gestational diabetes,” “neural tube defects,” and “congenital heart defects.” Boolean operators (AND/OR), truncation, and database-specific filters were applied to maximize the retrieval of relevant studies.
2. Copper, Zn, and Se Circulating Levels in Pregnant Women Around the World
This section included studies that examined Cu, Zn, and Se levels in maternal and cord blood from around the world. Some studies reported their numerical values as medians, while others opted for mean ± standard deviation. Copper, Zn, and Se levels in maternal and cord blood were considered only in healthy pregnant women, to: (1) conduct comparative analyses between countries and propose optimal ranges for Cu, Zn, and Se in whole blood and serum/plasma, (2) examine differences in Cu, Zn, and Se levels between maternal and cord blood, (3) propose optimal ranges for Cu, Zn, and Se depending on the trimester of pregnancy, and (4) examine differences in Cu, Zn, and Se levels between arterial and venous cord blood.
2.1. Maternal Blood Cu, Zn, and Se Levels Worldwide
The observed global range of maternal Cu levels spans approximately from 400 to 2500 μg/L, with some of the highest levels reported in Bangladesh (2508 μg/L) [19], Kuwait (2404 μg/L) [20], and Turkey (2402 μg/L) [21]. The lowest maternal Cu levels were reported from Iran (213 μg/L) [22], Sweden (437 μg/L) [23], Nigeria (517 μg/L) [24], and South Korea (575 μg/L) [25], observing no apparent trend regarding parts of the world and reported low maternal Cu levels. Details are given in Figure 2a.
The highest levels of maternal Zn serum/plasma levels were observed in two studies from China (5368 μg/L, reported by Shen et al., 2015 and 5794 μg/L, reported by He et al., 2024) [26,27], followed by the Zn level reported in Indonesia (4516 μg/L) [28]. The data noted by these studies are markedly elevated, raising concerns about potential preanalytical errors that could have influenced the findings. He et al. (2024) reported that their participants resided in one of the world’s largest electronics manufacturing hubs [27], a factor that could account for the elevated Zn levels observed in their study. If the aforementioned studies from China and Indonesia are excluded, the majority of other studies worldwide fall into the loose range of 350–1500 μg/L for median Zn maternal sera/plasma levels. The lowest maternal sera/plasma Zn levels of 108 μg/L were shown in the study from Sudan [29], followed by 334 μg/L reported in Iran [30], and 416 μg/L reported in Nigeria [31]. Details are given in Figure 3a.
Since Zn levels differ between whole blood and serum/plasma, primarily due to Zn’s strong binding affinity to hemoglobin (Hb) within erythrocytes, which are absent in plasma or serum [32], we chose to report a separate global reference range for Zn concentrations in whole blood. Thus, considering maternal whole blood, the highest Zn levels were observed in Spain (6.70 mg/L) [33], followed by Argentina (6.68 mg/L) [34], and South Africa (6.29 mg/L) [35], while the lowest reported maternal blood Zn level came from Kuwait (0.696 mg/L) [36]. Details are given in Figure 4a.
Regarding maternal blood Se levels worldwide, Tanzania [37] showed the highest Se levels (242 μg/L), followed by Nigeria (168 μg/L) [31], China (141 μg/L) [38], and Serbia (135 μg/L) [39]. Globally, Bangladesh [40] showed the lowest Se maternal blood level with 32 μg/L, followed by Turkey (47.6 μg/L) [21]. Based on reported studies, maternal blood Se levels worldwide range from approximately 40 μg/L to 250 μg/L. Details are given in Figure 5a.
2.2. Cord Blood Cu, Zn, and Se Levels Worldwide
Some of the highest Cu cord levels were reported in Kuwait (2406 μg/L) [36], India (1410 μg/L) [41], and Egypt (1370 μg/L) [42]. Some of the lowest Cu cord levels were reported in the United Kingdom (232 μg/L) [43], China (250 μg/L) [44], and Serbia (276 μg/L). Based on the reported studies, Cu cord levels worldwide span approximately from 230 μg/L to 2400 μg/L [21,36,39,40,41,42,43]. Details are given in Figure 2b.
Globally, the highest Zn levels in cord sera/plasma (Figure 3b) were reported in Bangladesh (3000 μg/L) and Indonesia (2938 μg/L) [28,45]. In contrast, the lowest Zn cord sera/plasma levels were noted in Serbia (356 μg/L) and Nigeria (426 μg/L) [31,39]. Based on reported studies, excluding the two highest cord serum/plasma Zn levels from Asia, the global range of cord Zn levels generally spans from 350 μg/L to 1400 μg/L.
The highest levels of Zn in cord whole blood were observed in India (9.15 mg/L), while Zn levels in cord blood from other countries ranged from 1.10 to 2.50 mg/L (Figure 4b) [41]. Given the notably higher cord Zn levels (both in sera/plasma and whole blood) observed in South and South-East Asia, it can be hypothesized that these findings could be influenced by elevated Zn concentrations in local soil and groundwater, which could, in turn, affect Zn content in foodstuffs and ultimately contribute to the high Zn levels in cord blood [46].
Nigeria exhibited the highest global Se cord blood level (197 μg/L) among the reported studies, followed closely by Bangladesh (190 μg/L) [31,45]. According to the Nigerian study, the cord blood Se levels they observed were higher than the reference range, a finding they attributed to the efficient placental transfer of Se from mother to fetus [31]. Interestingly, two independent studies also reported the lowest global Se cord blood levels in Bangladesh, both noting the same value (15.8 μg/L) [47,48], followed by the Se level reported in India (22.1 μg/L) [49]. According to reported studies, if the lowest reported levels from two South Asian studies are excluded, the global range for cord blood Se broadly falls between 30 μg/L and 190 μg/L. Details are given in Figure 5b.
2.3. Differences in Levels of Cu, Zn, and Se Between Maternal and Cord Blood
Analysis of global data indicates that maternal blood Cu levels tend to be higher than those reported in cord blood (Figure 2 and Table 1). This can be explained by the strict regulation of Cu transfer from mother to fetus [50]. However, some exceptions exist. A study from Kuwait reported higher Cu levels in cord blood than in maternal blood (2406 μg/L vs. 853 μg/L, respectively) [36]. A study from Egypt observed higher maternal Cu levels overall but found relatively similar levels between maternal and cord blood (1630 μg/L vs. 1370 μg/L, respectively) [42].
Far more of the included studies assessed Zn levels in serum or plasma (36 studies reported maternal sera/plasma Zn levels, while 27 studies reported Zn levels in cord sera/plasma samples) than in whole blood (12 studies reported Zn levels in maternal whole blood samples, and 12 studies reported Zn levels in cord whole blood) (Figure 3 and Table 2). Zinc levels in both maternal and cord serum/plasma show considerable global variation. In several studies reporting relatively low maternal Zn levels, cord Zn levels remained relatively comparable, suggesting efficient fetal uptake [31,50,51]. The substantial inter-study variability worldwide could be attributed to factors such as differences in dietary habits and prenatal supplementation practices. Notably, the highest maternal Zn serum/plasma levels were reported in two independent studies from China, with levels exceeding 5000 μg/L, whereas the average levels worldwide generally range between 350 and 1500 μg/L [26,27]. Interestingly, most studies found higher Zn levels in cord serum/plasma than in corresponding maternal matrices [52,53,54]. Overall, the data suggest that Zn levels tend to be higher in cord serum/plasma than in maternal serum/plasma.
Considering Zn whole blood levels, results differed somewhat across countries. For instance, Al-Saleh et al. (2007 Kuwait) and Srivastava et al. (2002, India) reported higher Zn levels in cord blood than in maternal blood [20,41]. However, the majority of studies reported higher Zn levels in maternal whole blood than in cord whole blood, which was opposite to the trend observed in the sera/plasma samples (Figure 4 and Table 2). This likely reflects differences in how Zn is distributed between blood compartments: the placenta actively transports Zn to the fetus to support growth, particularly in late gestation, which increases extracellular (serum/plasma) Zn in cord blood, while intracellular Zn within fetal red blood cells remains comparatively lower.
The majority of studies reported that Se levels tend to be lower in cord blood than in maternal blood (Figure 4 and Table 3). This may be explained by the carefully regulated transfer of Se to the fetus, as well as the enhanced antioxidant defenses in the mother during pregnancy [50]. A study from Spain reported similar Se levels in maternal and cord blood (107 μg/L vs. 100 μg/L, respectively) [33]. However, some opposite trends were observed as well. For example, one study from China showed higher Se levels in cord blood (126 μg/L) than in maternal blood (100 μg/L), and a study from Nigeria exhibited the same trend (197 μg/L in cord blood vs. 168 μg/L in maternal blood) [31,55].
2.4. Copper, Zn, and Se Levels Depending on the Trimester of Pregnancy
Based on published data for Cu, Zn, and Se depending on the trimester of pregnancy (Table 1), Table 4 summarizes the levels of Cu, Zn, and Se in maternal blood depending on the trimester of pregnancy, while Table 5 suggests reference intervals for these trace elements in healthy, normal pregnancies. Our review of the literature revealed that Cu levels tend to increase as the pregnancy progresses. The lowest Cu level in the 1st trimester (1053 μg/L) was reported by Martin-Lagos et al., while a study by Polanska et al. (2017) reported the highest level (1980 μg/L) [56,57]. Overall, studies revealed a range of 1000 to 1900 μg/L Cu in maternal blood for the 1st trimester. In the 2nd trimester, Cu levels were in the range of 1100 to 2400 μg/L, while in the 3rd trimester, they were in the range of 1100 to 2600 μg/L (Table 4). The increase in Cu levels during pregnancy could be attributed to the expansion of maternal blood volume, the growing fetal demand for essential nutrients, and elevated ceruloplasmin concentrations driven by increased estrogen levels [58].
By reviewing the literature data in Table 2, it is notable that most studies reported a steady decrease in Zn levels as the pregnancy progresses, with two exceptions. A study by Choi et al. observed a decline in Zn levels from the 1st (66 μg/L) to the 2nd (55 μg/L) trimester, followed by an increase in the 3rd trimester (94 μg/L). In contrast, Huang et al. reported an opposite trend, with Zn levels rising from the 1st (1030 ± 270 μg/L) to the 2nd (1170 ± 450 μg/L) trimester, then decreasing in the 3rd trimester (1110 ± 280 μg/L) [70,71]. The general decrease in Zn levels from 1st to 3rd trimester could be explained by the increase in placental and fetal demand [72]. Taking into consideration the reported Zn levels in healthy, normal pregnancies, most studies fell into the loose ranges of 70 to 910 μg/L for the 1st, 70 to 810 μg/L for the 2nd, and 70 to 750 μg/L for the 3rd trimester (Table 2).
In contrast to Cu, our analysis revealed that Se levels tend to decrease as the pregnancy progresses (Table 3 and Table 4). These observations can likely be attributed to the utilization of Se from maternal blood to support fetal development and placental growth and function [72]. Based on the literature data, Se levels for the 1st trimester fell in the range of 45 to 110 μg/L, while levels in 2nd and 3rd trimesters ranged from 42 to 100 μg/L and 37 to 91 μg/L, respectively (Table 2).
2.5. Differences in Cu, Zn, and Se Levels Between Arterial and Venous Cord Blood
The umbilical cord usually contains two arteries and one vein. The umbilical arteries carry deoxygenated blood and metabolic waste from the fetus to the placenta, while the umbilical vein returns oxygenated, nutrient-rich blood from the placenta to the fetus. Together, they maintain essential fetal–placental circulation throughout gestation. Since arterial and venous blood do not have the same biochemical composition, the question arises whether the levels of Cu, Zn, and Se are the same or different [73,74]. In this regard, Al-Saleh et al. (2011) reported that trace element levels in cord venous serum were consistent with studies using mixed cord serum (arterial + venous) and with those studies using arterial and venous cord serum separately [36]. However, we found that the literature findings do not fully support their statement. Thus, Osada et al. (2002) found that Cu and Zn levels were significantly lower in umbilical artery serum (505 ± 149 µg/L and 406 ± 84.2 µg/L, respectively) than in umbilical vein serum (596 ± 71.8 µg/L and 465 ± 103 µg/L, respectively) in neonates of appropriate gestational age [75]. Their findings are consistent with the study by Rossipal et al. (2000) [76]. Interestingly, Díaz-Gómez et al. (2017) found lower levels of Zn in arterial cord serum (1548 ± 326 µg/L) than in venous cord serum (1959 ± 626 µg/L) but conversely found higher levels of Cu in arterial cord serum (451 ± 190 µg/L) than in venous cord serum (311 ± 216 µg/L) [54]. Al-Saleh et al. (2011) also demonstrated that Se levels in arterial cord serum were significantly higher than in venous cord serum (107 ± 7.20 vs. 80.4 ± 2.60 µg/L), while Rossipal et al. (2000) and Osada et al. (2002) did not find significant differences in Se levels in these matrices [36,75,76]. Lazer et al. (2012) investigated the differences in Cu, Zn, and Se levels in cord arterial and venous plasma during active labor and elective cesarean delivery [51]. In active labor, Cu levels were higher in the cord vein (1109 ± 885 μg/L) than in the cord artery (993 ± 812 μg/L). In contrast, during elective cesarean delivery, Cu levels were higher in the cord artery (905 ± 773 μg/L) compared to the cord vein (625 ± 658 μg/L). A similar pattern was observed for Se levels. In both active labor and elective cesarean delivery, Zn levels were consistently higher in cord artery plasma than in cord vein plasma [51]. Since few studies have addressed differences in Cu, Zn, and Se levels between arterial and venous cord serum/plasma, further research is urgently needed to provide more detailed insight into trace element levels in both serum and whole blood.
3. Copper, Zn, and Se Levels in Altered Pregnancy
In this section, the included studies consist of cross-sectional, case–control, retrospective, prospective cohort studies, and meta-analytical studies showing the influence of Cu, Zn, and Se on pregnancy outcomes, emphasizing fetal LBW and PTB, PE, GDM, NTDs, and CHDs.
3.1. Association Between Cu, Zn, and Se with Birth Weight and Neonatal Anthropometric Parameters
One indicator/predictor of fetal growth and development is birth weight. According to the World Health Organization (WHO), LBW has become one of the major risk factors for the global burden of disease [120]. The prevalence of LBW infants showed different geographic patterns, with rates of 7.6% in the United States, 5.9–11.8% in China, and about 25% in India [38]. The current rate of LBW stands at 8.2% of births in developed countries [121]. An estimated 20 million (15.5%) babies are born with LBW (<2.5 kg) worldwide each year, and approximately 95.5% of these births occur in low- and middle-income countries [114].
Birth weight primarily depends on genetics, placental circulation, and maternal nutrition [122]. Babies with LBW are about 20 times more likely to die during infancy and childhood than babies born with normal birth weight [114]. Intrauterine growth restriction and LBW are associated with increased morbidity and mortality, poor cognitive development, and neurological impairment, but also with widespread diseases later in life, including diabetes, cardiovascular diseases, renal dysfunction, mental disorders, and other complications [122].
Poor nutrition during pregnancy has been linked to miscarriages, stillbirths, and early neonatal mortality [123]. As premature babies are born before rapid intrauterine growth, they are susceptible to deficiencies of essential trace elements [124]. Micronutrient deficiencies are associated with pregnancy complications and anthropometric abnormalities in newborns [125]. In contrast, mineral supplementation in women with poor nutrition reduces the incidence of pregnancy complications [126].
Several studies investigated the relationship between Cu levels during pregnancy and birth outcomes, yielding inconsistent results (Table 1). Notably, Al-Saleh et al. (2011), Bermúdez et al. (2015), and Chen et al. (2021) reported a significant inverse relationship between cord blood Cu levels and birth weight, suggesting that elevated Cu levels could negatively affect fetal growth [36,47,77]. Bermúdez et al. (2015) further observed that cord Cu levels were significantly higher among small for gestational age (SGA) infants compared to appropriate for gestational age (AGA) and large for gestational age (LGA) groups [77]. Chen et al. (2021) mentioned that animal studies demonstrate growth restriction following high Cu exposure, such as in rat fetuses and fathead minnows, likely due to the downregulation of growth-related genes [47]. They also noted that elevated Cu exposure may pose a developmental risk [47].
In contrast, Awadallah et al. (2004) found no significant correlation between either maternal or cord Cu levels and birth weight [52]. Cabrera-Rodríguez et al. (2018) and Kippler et al. (2010) also found no significant association between cord Cu levels and birth weight, while Díaz-Gómez et al. (2017) found no significant correlation between maternal Cu levels and birth weight [45,54,78]. Overall, while some evidence points to a potential negative impact of elevated cord Cu levels on birth weight, findings remain inconclusive. Differences in study populations, dietary Cu exposure, matrices (plasma, serum, whole blood), and analytical methods could account for the variability in results. To establish a clearer understanding of how Cu influences fetal growth, future research should prioritize large-scale, prospective cohort studies with standardized sampling and measurement protocols.
Among the reviewed studies examining the relationship between Zn levels during pregnancy and birth weight, several reported a significant positive association (Table 2). Notably, Abdellatif et al. (2021) observed that higher Zn levels in cord blood were significantly correlated with increased birth weight [42]. Similarly, Awadallah et al. (2004) found a positive correlation between cord Zn levels and birth weight in healthy pregnancies [52]. These findings support the potential role of Zn in promoting fetal growth. Given Zn’s fundamental roles in antioxidant protection, immune competence, tissue formation, and cellular proliferation, all of which underpin normal fetal development, its potential impact on fetal growth and birth weight warrants close consideration.
In contrast, the majority of other studies, by Al-Saleh et al. (2011), Bermúdez et al. (2015), Bocca et al. (2019), Cabrera-Rodríguez et al. (2018), Chen et al. (2021), and Díaz-Gómez et al. (2017), found no significant link between Zn levels (in maternal or cord blood) and birth weight [33,36,47,54,77,78]. Additionally, Bocca et al. (2019) found no correlation between maternal and cord Zn levels, suggesting inconsistent transplacental transfer or homeostatic regulation [33]. While some studies—particularly those conducted in Middle Eastern and South Asian populations—indicate a positive association between Zn level and birth weight, the majority of findings from European cohorts do not support a consistent link. These inconsistencies could stem from regional variation in dietary Zn intake, underlying micronutrient profiles, socioeconomic factors, and environmental conditions. Differences in study methodologies, such as sample size, study design, timing, and type of Zn assessment, and how well confounders are accounted for, are also likely contributors. Taken together, these elements indicate that the association between Zn status and birth weight is highly context-specific and shaped by a complex mix of biological, environmental, and population characteristics.
Regarding Se, only Chen et al. (2021) reported a positive link between cord blood Se levels and newborn birth weight, suggesting that higher Se levels could contribute to increased birth weight (Table 3) [47]. In contrast, Al-Saleh et al. (2011), Bermúdez et al. (2015), Cabrera-Rodríguez et al. (2018), and Hu et al. (2015) found no significant relationship between maternal or cord blood Se levels and birth weight [36,38,77,78]. Al-Saleh et al. (2011) proposed that transplacental Se transfer occurs via passive diffusion and that monitoring Se levels in maternal or cord blood could not be useful for assessing fetal growth [36]. The majority of available evidence indicates that Se levels during pregnancy are not consistently linked to birth weight (Figure 6). Variation in findings across studies may reflect differences in geographic setting, underlying maternal nutritional status, and environmental sources of Se exposure. In addition, inconsistencies in the biological matrices used for Se assessment, laboratory analytical techniques, sample sizes, and overall study design could also contribute to the mixed results. Taking all of this into account, further large-scale studies are warranted to provide more comprehensive insights.
Several studies investigated the influence of Cu, Zn, and Se blood levels on neonatal anthropometric parameters, with mixed findings (Table 1, Table 2 and Table 3). Abdellatif et al. (2021) reported significant positive correlations between cord and maternal Cu levels with gestational age, birth length, and head circumference [42]. Similarly, Xu et al. (2022) found maternal Cu levels associated with shorter birth length and smaller head circumference [34]. Kot et al. (2021) observed a positive link between maternal Cu and gestational age, but a negative correlation with head circumference [127]. In contrast, Kippler et al. (2010) and Daniali et al. (2023) found no significant associations between Cu levels and gestational age or birth size [22,45]. Perveen et al. (2022) and Srivastava et al. (2002) also reported no significant differences in maternal Cu levels by gestational age, though Srivastava et al. (2002) noted a weak correlation between cord Cu and gestational age [41,88]. Grzesik-Gąsior et al. (2023) found the Cu/Zn ratio was significantly associated with head circumference [89]. Hassan et al. (2025) [30] reported negative correlations between serum Cu levels and anthropometric measures, especially head circumference. Details are given in Table 1.
Regarding Zn, Abdellatif et al. (2021) and Kippler et al. (2010) reported significant positive correlations between cord blood Zn levels and gestational age, birth length, and head circumference [42,45]. Abdellatif et al. also found that maternal Zn levels were positively associated with these parameters [42]. Similarly, Díaz-Gómez et al. (2017) and Kot et al. (2021) observed positive correlations between maternal Zn levels and gestational age, although Kot et al. (2021) noted a negative correlation between cord Zn and head circumference [54,127]. In contrast, Perveen et al. (2022) and Srivastava et al. (2002) [41] found no significant associations between plasma or cord Zn levels and gestational age [41,88]. Grzesik-Gąsior et al. (2023) and Daniali et al. (2023) also reported no significant associations between Zn levels and anthropometric outcomes [22,89]. Xu et al. (2022) found negative associations between maternal Zn levels and anthropometric parameters, although they observed a positive link with gestational age in female infants [34]. Details are given in Table 2.
Al Saleh et al. (2004) concluded that blood Se levels are not useful for assessing fetal growth. Similarly, Kippler et al. (2010) and Grzesik-Gąsior et al. (2023) reported no significant associations between Se levels and gestational age or anthropometric parameters [36,45,89]. In contrast, Makhoul et al. (2004) found a significant positive correlation between gestational age and cord serum Se levels [128]. Tang et al. (2016) and Xu et al. (2022) observed negative correlations between Se levels and anthropometric parameters [34,118]. Details are given in Table 3.
3.2. Association Between Cu, Zn, and Se and Preterm Birth
Preterm birth, defined as birth before 37 completed weeks of gestation, is the leading global cause of mortality in infants and children under 5 years of age [92]. Causes of PTB include decidual inflammation, decidual hemorrhage, pathologic uterine distention, and conditions that increase fetal and maternal stress [129]. According to two meta-analytic studies, trace elements could play a role in the pathogenesis of PTB [130,131]. Thus, Chiudzu et al. (2020) found that serum Cu levels were significantly higher in women who had spontaneous PTB (median, 2.61 mg/L) compared to women who delivered at term (median, 2.39 mg/L) [108]. In contrast, a study by Li et al. (2024) found no significant difference in serum Cu levels between cases (median, 1795 μg/L) and controls (median, 1823 μg/L), both of whom delivered at full term [107]. In the third study, conducted by Gohari et al. (2023), serum Cu levels were significantly lower in women who had preterm deliveries (1498 ± 531 μg/L) than in those who delivered at term (1840 ± 714 μg/L) [132]. Data related to Cu levels in cord serum reported by Galinier et al. (2005) showed that serum cord Cu levels were significantly lower in preterm than in term infants (full-term: 425 ± 133 µg/L vs. preterm: 286 ± 127 µg/L) [80]. On the other hand, Wang et al. (2022) reported the opposite results for cord blood Cu (cases: 540 μg/L vs. controls: 516 μg/L) [59]. Huang et al. (2021) in their study from Bangladesh showed that Cu levels in cord blood were not associated with the risk of PTB [48]. A multicountry meta-analysis conducted by Monangi et al. (2024) found that for every 1 μg/mL increase in maternal Cu level, the risk of PTB increased by 30% across 18 cohorts [133]. Although maternal Cu levels could be associated with PTB, Cu alone was not sufficient to predict or directly cause the condition. Copper is part of a broader interplay involving inflammation, oxidative stress, maternal nutrition, and genetic and environmental factors [134]. Low blood Cu levels can impair the body’s antioxidant defenses, compromise immune function, and increase susceptibility to infections. Copper is a cofactor for many enzymes, including superoxide dismutase, which protects cells from oxidative damage; low Cu levels can therefore lead to heightened oxidative stress, which could adversely affect placental function. Impaired immunity and increased infection risk can trigger inflammatory responses that compromise fetal membranes and the uterine environment. Together, these mechanisms have been linked to adverse pregnancy outcomes such as PTB and premature rupture of membranes, highlighting the possible role of adequate Cu levels in maintaining a healthy pregnancy [135]. Details are given in Table 1.
Regarding Zn, Chiudzu et al. (2020) found that serum Zn levels were higher in women who had spontaneous PTB (810 μg/L) than in those who delivered at term (730 μg/L) [108]. Li et al. (2024) did not find a statistically significant difference between serum Zn levels in cases (828 μg/L) and controls (813 μg/L) [107]. Huang et al. (2021) concluded that Zn levels in cord serum did not differ between preterm and full-term infants [48]. In contrast, Kucukaydin et al. (2018), in a study investigating the levels of trace elements in cord blood in cases of preterm premature rupture of membranes (PPROM), found that Zn levels were lower both in maternal blood and in the blood of preterm infants compared to levels in maternal blood without PPROM [72]. Specifically, maternal serum Zn levels were 800 ± 300 μg/L in the PPROM group vs. 1360 ± 740 μg/L in the non-PPROM group. In cord serum, Zn levels were 1170 ± 430 μg/L with PPROM compared to 1570 ± 450 μg/L without PPROM [72]. The overall results of the analyzed studies are contradictory and show differing data; therefore, a definitive conclusion about a significant link between Zn and PTB cannot be drawn. However, it remains possible that Zn, similarly to Cu, could play a role in the pathogenesis of PTB. Additional well-designed, large-scale studies are needed to clarify the potential contribution of Zn to PTB risk and to better understand the underlying biological mechanisms. Details are given in Table 2.
Chiudzu et al. (2020) reported that serum Se levels were higher, though not significantly, in women with spontaneous PTB (79.7 µg/L) compared with those who delivered at term (74.2 µg/L) [108]. Similarly, Li et al. (2024), in a study of 192 preterm and 282 full-term deliveries, found no significant difference in serum Se concentrations between the groups (preterm: 99.8 µg/L; term: 96.8 µg/L) [107]. Huang et al. (2021) also observed no significant difference in cord blood Se levels between preterm and term infants, consistent with their findings for other analyzed elements [48]. In contrast, a multicohort meta-analysis by Monangi et al. (2024), which included 17 cohorts comprising approximately 10,000 pregnant women, reported that although some studies identified a statistically significant correlation between higher maternal Se levels and reduced PTB risk, this association was not consistent across all populations [133]. The substantial heterogeneity observed suggests that contextual factors—such as nutritional status, sociodemographic characteristics, and genetic background—could influence the relationship between Se and PTB. Additional details are provided in Table 3.
3.3. Association Between Cu, Zn, and Se and Preeclampsia
Preeclampsia, as a subgroup of hypertensive disorders of pregnancy, is an entity associated with new-onset hypertension (>140/90 mm Hg systolic/diastolic blood pressure), usually with accompanying proteinuria (>300 mg/24 h) [118]. It commonly occurs after 20 weeks of gestation and often near term [136]. Preeclampsia encompasses 2% to 8% of pregnancy-related complications, more than 50,000 maternal deaths, and over 500,000 fetal deaths annually worldwide [137]. Nowadays, PE is considered as more than hypertension and proteinuria; it is now known to be a dysfunction of several organ systems (i.e., renal, hepatic, neurologic, hematological, or uteroplacental) caused by endothelial dysfunction [138]. Preeclampsia can be broadly categorized into two subtypes: early-onset (placental) and late-onset (maternal) PE [139]. Common risk factors, such as first pregnancy, multiple pregnancies, and pre-existing conditions such as hypertension and diabetes, can increase the risk of PE, as can maternal age (both younger and older than optimal), obesity, a family history of PE, and certain autoimmune conditions. In addition, assisted reproductive technologies, kidney disease, and specific infections are associated with a higher risk of PE [140]. Due to inadequate placentation and hypoxia, various factors with angiogenic and anti-angiogenic effects and oxidative stress parameters are elevated in PE [135]. To overcome this, specific trace elements are needed that would ultimately act synergistically with antioxidants and prevent further cell damage [18].
The majority of studies demonstrated significantly higher blood Cu levels in pregnant women with PE than in normotensive healthy pregnant women (controls) [34,49,96,97,98,99,100,101]. However, two studies reported contrasting findings, with lower serum Cu levels in PE pregnancies than in controls [19,141]. Regarding cord blood, Negi et al. (2012) found that Cu levels were significantly lower in cord plasma from women with PE (349 ± 95.3 µg/L) and eclampsia (261 ± 72.1 µg/L) than in controls (425 ± 82.3 µg/L) [49]. These results are consistent with a study from England, Kurlak et al., who reported higher serum Cu in women with PE (1606 μg/L) than in controls (1541 μg/L) [43]. Kurlak et al. [43] proposed that women who develop pre-eclampsia could exhibit increased uptake of essential trace elements such as Cu, potentially as a compensatory response to counteract the elevated oxidative stress associated with the condition. Thus, as Kurlak et al. [43] noted, higher Cu levels observed in such cases could be a consequence, rather than a cause, of pre-eclampsia [43]. On the other hand, no significant difference was found between early-onset and late-onset PE in maternal plasma Cu levels. In contrast, cord plasma Cu levels did differ between these two groups, with higher levels found in cases of late-onset PE compared to early-onset PE [43]. Details are given in Table 1.
Regarding Zn, most of the analyzed studies (n = 6) found no statistically significant difference in blood Zn levels between pregnant women with PE and controls [29,34,96,98,100,110]. Three studies reported higher Zn levels in PE women than in controls, while two studies observed lower Zn levels in the blood of PE women than in the blood of controls [24,27,99,141]. For example, Negi et al. (2012) showed that Zn levels were significantly lower in cord plasma from PE (744 ± 150 µg/L) and eclampsia (677 ± 117 µg/L) cases than in controls (830 ± 88.5 µg/L) [49]. Kurlak et al. [43] showed that maternal plasma Zn was significantly lower in 55 women with PE (418 µg/L) than in 60 controls (486 µg/L). Contrary to Cu, Kurlak et al. [43] found a significant difference in early-onset/late-onset PE, with lower blood Zn levels in both early-onset and late-onset PE compared with controls [43]. Zinc levels in cord plasma were significantly higher than maternal Zn levels in both PE groups, and there were no differences in circulating levels when the PE group was divided into early/late onset PE. Details are given in Table 2.
Regarding Se, all analyzed studies showed lower blood Se levels in women with PE than in controls [40,110,116]. Also, Negi et al. (2012) reported significantly lower cord blood Se levels in PE (18.6 ± 5.21 μg/L) and eclampsia (n = 14) (16.3 ± 5.23 μg/L) than in controls (22.2 ± 4.19 μg/L) [49]. These findings are consistent with those of Kurlak et al., who reported that Se levels in cord plasma were significantly lower (42.7 μg/L) than in maternal plasma (59.5 μg/L) [43]. Moreover, Se levels were also significantly lower in the cord plasma of newborns born to women with PE (37.4 µg/L) than in controls (42.7 µg/L). The increased oxidative stress observed in PE could contribute to reduced Se levels. In addition, PE causes impaired placental function, which could hinder the transfer of Se to the maternal circulation, further contributing to lower Se concentrations [43]. In contrast, Makhoul et al. (2004) in their cross-sectional study show that cord serum Se levels were significantly associated with birth weight and 5 min Apgar score, but not with PE [128]. Details are given in Table 3.
In summary, compared with healthy pregnancies, it can be concluded that Cu levels are significantly higher in the blood of pregnant women with PE, whereas Se levels are significantly lower (Figure 6). In the case of Zn, the findings are inconsistent, making it difficult to draw a definitive conclusion. Several factors could help explain this variability in Zn status. Inflammatory processes could influence the circulating levels of Zn in some cases. Differences in maternal nutrition, supplementation practices, and overall dietary intake across study populations can also influence Zn status. Additionally, oxidative stress could alter the activity of zinc-binding proteins, and the degree of placental dysfunction or disease severity could affect how Zn is handled during pregnancy [50]. Variations in study design, such as when samples were collected or how Zn was measured, likely contribute further to the mixed findings reported in the literature. These observations highlight the complex interplay of trace elements in PE and underscore the need for further well-designed, large-scale studies to better understand how imbalances in Cu, Se, and Zn could contribute to the pathophysiology of the disease and influence maternal and fetal outcomes.
3.4. Association Between Cu, Zn, and Se and Gestational Diabetes Mellitus
Gestational diabetes mellitus is a condition characterized by hyperglycemia during pregnancy in women who have not been previously diagnosed with diabetes [142]. The most common complications of GDM include macrosomia, which is associated with an increased risk of operative delivery and adverse neonatal outcomes, such as shoulder dystocia and its related complications [143]. Additionally, PE occurs more frequently in women with GDM. According to ACOG, all pregnant women should undergo laboratory-based screening for GDM, typically through blood glucose testing between 24 and 28 weeks of gestation (ACOG Practice Bulletin No. 190). However, for overweight or obese women who present additional risk factors—such as a previous history of GDM—early screening for undiagnosed type 2 diabetes is recommended, ideally at the first prenatal visit [144]. Many healthcare providers use a two-step approach for GDM screening, beginning with a 50 g oral glucose tolerance test (OGTT). Although the American Diabetes Association (ADA) acknowledges that Hb A1C testing could also be utilized, it is generally not recommended as a standalone diagnostic tool due to its lower sensitivity compared to OGTT [145].
There is evidence that trace elements could play a role in the pathogenesis of GDM [105]. We analyzed three studies concerning Cu levels in maternal blood, and all three showed different results. In one study, Cu levels in pregnant women with GDM were higher; in another, they were lower; and in the third, there was no difference compared to healthy pregnant women [106,119,146]. Details are given in Table 1.
Regarding Zn, the situation is somewhat different—most of the studies reviewed reported lower blood Zn levels in women with GDM compared to controls. Only one study, conducted by Mohammadzadeh et al. (2023), found no difference in serum Zn levels between the GDM group (69.20 μg/L) and the controls (67.57 μg/L) [104]. Details are given in Table 2.
Tan et al. (2001) analyzed serum Se levels in healthy pregnant women, those with impaired glucose tolerance, and those with GDM. They found that serum Se levels were significantly lower in women with GDM (63.5 ± 12 μg/L) than in controls (74.1 ± 16.7 μg/L) [119]. In contrast, Mohammadzadeh et al. (2023) reported different findings; they did not find a statistically significant difference in serum Se levels between women with GDM (98.2 ± 22.8 μg/L) and controls (94.7 ± 17.8 μg/L) [104]. Details are given in Table 3.
In summary, it can be concluded that the findings related to Cu and Se are inconsistent, and that further studies with larger sample sizes are needed to draw definitive conclusions about their association with GDM. As for Zn, there appears to be a pattern suggesting that maintaining optimal levels could be important in preventing its decline in GDM [147,148] (Figure 6). Zinc is essential for insulin synthesis, storage, and secretion, as well as for glucose metabolism and antioxidant defense, all of which are critical for maintaining glycemic control during pregnancy [104,149]. Therefore, ensuring optimal Zn status could help prevent or mitigate the decline in Zn levels often observed in women with GDM, potentially supporting better maternal and fetal outcomes.
3.5. Association Between Cu, Zn, and Se and Neural Tube Defects
Neural tube defects are birth defects of the brain and spinal cord that occur when the neural tube, which forms the brain and spinal cord, does not close completely during early pregnancy [146]. The defects arise from failure of embryonic neural tube closure by the fourth week of pregnancy [150]. NTDs occur in 0.5 to 2 per 1000 pregnancies [150]. The most common risk factor is a previous pregnancy with NTDs [146]. Periconceptional folate intake (4 mg/day of folic acid) can prevent about 70% of NTDs [151].
The summarized data of the literature search are given in Table 1, Table 2 and Table 3. Copper levels in the blood of women with NTD fetuses were significantly higher than those in healthy pregnant controls, which indicates that high levels of Cu could be associated with NTD development. Zeyrek et al. (2009) reported that Cu levels in both maternal and cord serum were significantly higher in the NTD group than in healthy controls [21]. Specifically, maternal serum Cu levels were 2831 ± 1017 μg/L in the NTD group vs. 2402 ± 744.2 μg/L in controls, while cord serum Cu levels were 790 μg/L in the NTD group vs. 517 μg/L in controls. In contrast, maternal serum Zn levels were significantly lower in the NTD group (836 ± 334 μg/L) than in controls (1036 ± 300 μg/L). However, cord serum Zn levels did not differ significantly between groups (NTD: 1391 ± 504 μg/L; controls: 1294 ± 346 μg/L). The Cu/Zn ratio in women’s sera of neonates with NTD was significantly higher than in controls, so this ratio could have a diagnostic value. The same authors showed no significant differences for Se levels in maternal serum (cases: 46.8 ± 26.4 μg/L vs. controls: 47.6 ± 20.6 μg/L) and cord serum (cases: 42.2 ± 21.9 μg/L vs. controls: 39.9 ± 20.0 μg/L) between NTD cases and controls [21]. In the study by Kucukaydin et al. (2018), who investigated Zn, Se, and Cu plasma levels in neonates diagnosed with NTDs and their mothers, plasma levels of Zn and Se were significantly higher in women from the control group compared to those from the NTD group [72]. Specifically, Zn levels were 1392 ± 111 μg/L in controls vs. 1084 ± 114 μg/L in the NTD group, and Se levels were 79.9 ± 8 μg/L in controls vs. 55.4 ± 7 μg/L in the NTD group. In contrast, Cu levels were significantly higher in the NTD group (2253 ± 245 μg/L) than in controls (1194 ± 295 μg/L). The same pattern was observed in cord plasma: Zn and Se levels were significantly lower in the NTD group than in controls, while Cu levels were significantly higher. Similar findings were reported by Cengiz et al. (2004), who showed that Cu serum levels were significantly higher in pregnant women whose babies had NTDs, compared to those with healthy babies (2331 ± 221 µg/L vs. 2073 ± 377 µg/L, respectively) [151]. In contrast, Zn serum levels were significantly lower in the NTD group (625 ± 159 µg/L) than in controls (1026 ± 237 µg/L) [151]. Golalipour et al. (2009) and Dey et al. (2010) reported the same trend regarding Zn; namely, Zn levels were significantly lower in pregnant women whose babies had NTDs compared to the control group [111,112]. Golalipour et al. (2009) reported maternal Zn levels of 745 μg/L in the NTD group vs. 877 μg/L in the control group [111]. Similarly, Dey et al. (2010) found that serum Zn levels were significantly lower in women with neonates who had NTDs (610 ± 53.1 μg/L) compared to women in the control group (883 ± 65.0 μg/L) [112]. Tian et al. (2022) showed that low maternal Se levels were associated with an increased risk of fetal malformations, including NTDs, and can negatively impact infant cognitive development [152]. Vats et al. (2014) and Cengiz et al. (2004) showed that blood Se levels measured in women with NTD neonates were significantly lower than in healthy pregnant women [37,151]. Specifically, Vats et al. (2014) reported the maternal blood Se level in NTD cases to be 306 ± 11.0 µg/L, while in controls it was 364 ± 17.1 µg/L [37]. Cengiz et al. (2004) reported the maternal serum Se level in NTD cases was 55.2 ± 11.3 µg/L, while in controls it was 77.4 ± 5.50 µg/L [151].
In summary, based on those aforementioned studies with consistent results, it can be concluded that pregnant women carrying a fetus with NTDs, as well as neonates with the same condition, exhibit higher blood levels of Cu and lower blood Zn and Se levels than do controls (Figure 6). The observed imbalances likely reflect the crucial roles of these trace elements in antioxidant defense, cell proliferation, and neural development during early fetal growth. These findings could potentially be of diagnostic significance in the future. Also, the diagnostic significance of the Cu/Zn ratio should be examined in the future.
3.6. Association Between Cu, Zn, and Se and Congenital Heart Defects
Congenital heart defects are the most common congenital anomalies in newborn babies (Xie et al. 2018) [102]. Screening for CHDs is a key component of the 2nd-trimester ultrasound, with >95% of pregnant women participating. The screening boasts high detection rates, identifying >80% of severe CHDs before birth [153]. Early detection enables accurate diagnosis and genetic testing, as well as timely planning and intervention [55].
Studies suggest that adequate intake of Zn and Se, and possibly maintaining an appropriate Zn/Cu or Se/Cu ratio, could be protective against CHDs. Yang et al. (2022) found that higher intakes of Zn and Se (from diet and supplements) during pregnancy could reduce the risk of CHDs, while no significant associations were found between dietary and supplement Cu intake with the risk of CHDs [154]. However, one study from China conducted by Guo et al. (2019) investigated the Se level in maternal hair and its link with CHDs [155]. They found that high levels of Se in maternal hair were associated with the presence of CHDs. Ou et al. (2017) measured Se levels in the blood of pregnant women whose babies had CHDs, and reported that the median blood Se level was significantly lower in the case group (pregnant women with babies diagnosed with CHDs) (172 μg/L) than in the control group (186 μg/L) [103]. Additionally, the same study demonstrated that the median maternal blood Cu level was significantly lower in the case group (838 μg/L) than in the control group (896 μg/L) [103] (Table 1, Table 2 and Table 3).
In summary, no reliable conclusions can be drawn about the benefits of Cu, Zn, and Se on CHDs, given the heterogeneity of the clinical matrices used by the authors and the small number of studies addressing this topic (Figure 6). Differences in population characteristics, nutritional status, environmental exposures, and the timing of trace element assessment could further contribute to the inconsistent findings. Given these limitations, additional well-designed, adequately powered studies are needed to clarify whether these essential trace elements play a meaningful role in the etiology or prevention of CHDs.
Limitations
Of the 83 studies analyzed, 34 controlled for key confounding factors such as dietary intake, supplementation, smoking status, BMI, parity, socioeconomic variables, genetic variants, and geographic differences. The limited and inconsistent adjustment for these variables represents an important limitation of the current evidence base. Nevertheless, the available data indicate that more comprehensive control of confounders would likely sharpen the estimates rather than substantially change the overall conclusions. In this sense, the main patterns observed across studies appear reasonably robust, though it remains essential to recognize that methodological constraints persist and should be taken into account when interpreting the findings. Differences in population characteristics, nutritional status, environmental exposures, and the timing of trace-element assessment may also contribute to the variability in findings. In light of these limitations, further well-designed and adequately powered studies are needed to better elucidate the role of trace elements in adverse pregnancy outcomes. Taken together, these constraints underscore the need for further large-scale, well-designed investigations that employ consistent and thorough adjustment for confounding factors.
4. Conclusions
To the best of our knowledge, this is the first study to examine the presented topic comprehensively. While Cu, Zn, and Se levels in blood-associated matrices during pregnancy differ across countries, they largely fall within a consistent range, enabling us to propose evidence-based global reference ranges for these essential trace elements in maternal blood and cord blood. Furthermore, most studies reported higher levels of Cu, Zn, and Se in maternal blood than in cord blood. Considering pregnancy trimesters, a clear trend can be observed regarding element levels: Zn and Se tend to decrease as the pregnancy progresses, while Cu levels increase. Only a few studies investigated differences in Cu, Zn, and Se levels between arterial and venous cord blood, and their findings are inconsistent. This highlights the urgent need for further research regarding this topic. Numerous studies have assessed the influence of Cu, Zn, and Se on neonatal anthropometry and birth outcomes, with mixed results. Evidence suggests potential associations between maternal trace element levels and preterm birth, although these are insufficient to establish predictive or causal relationships. More consistent patterns were observed for PE and GDM: women with PE generally exhibited higher Cu and lower Se levels, whereas women with gestational diabetes had lower Zn levels compared with healthy controls. Additionally, both pregnant women carrying fetuses with NTDs and affected neonates displayed higher Cu and lower Zn and Se levels than healthy controls. These findings raise important questions regarding the potential role of targeted trace element supplementation in the prevention and management of pregnancy complications.
Given these findings, further research is urgently needed. Large-scale, well-designed studies and meta-analyses are required to clarify the mechanistic roles of Cu, Zn, and Se in pregnancy and neonatal health. Future studies should prioritize standardized sampling and analytical protocols to improve comparability, employ longitudinal cohort designs to track trace element trajectories throughout pregnancy, and validate the proposed trimester-specific reference ranges in larger and more diverse populations. Additionally, investigations into environmental, dietary, and regional factors affecting trace element status are essential to understand the substantial variability observed across populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Da Silva J.A.L. Essential Trace Elements in the Human Metabolism Biology 20241390810.3390/biology 1311090839596863 PMC 11592267 · doi ↗ · pubmed ↗
- 2Aaseth J.O. Toxic and Essential Metals in Human Health and Disease 2021 Biomolecules 202212137510.3390/biom 1210137536291583 PMC 9599252 · doi ↗ · pubmed ↗
- 3Stehle P. Stoffel-Wagner B. Kuhn K.S. Parenteral Trace Element Provision: Recent Clinical Research and Practical Conclusions Eur. J. Clin. Nutr.20167088689310.1038/ejcn.2016.5327049031 PMC 5399133 · doi ↗ · pubmed ↗
- 4Mehri A. Trace Elements in Human Nutrition (II)—An Update Int. J. Prev. Med.202011210.4103/ijpvm.IJPVM_48_1932042399 PMC 6993532 · doi ↗ · pubmed ↗
- 5López-Alonso M. Rivas I. Miranda M. Trace Mineral Imbalances in Global Health: Challenges, Biomarkers, and the Role of Serum Analysis Nutrients 202517224110.3390/nu 1713224140647345 PMC 12251835 · doi ↗ · pubmed ↗
- 6King J.C. Physiology of Pregnancy and Nutrient Metabolism Am. J. Clin. Nutr.2000711218 S 1225 S 10.1093/ajcn/71.5.1218 s 10799394 · doi ↗ · pubmed ↗
- 7Kilinc M. Coskun A. Bilge F. Simsek Imrek S. Atli Y. Serum Reference Levels of Selenium, Zinc and Copper in Healthy Pregnant Women at a Prenatal Screening Program in the Southeastern Mediterranean Region of Turkey J. Trace Elem. Med. Biol.20102415215610.1016/j.jtemb.2010.01.00420569925 · doi ↗ · pubmed ↗
- 8Wang R. Zhang L. Chen Y. Zhang S. Zhuang T. Wang L. Xu M. Zhang N. Liu S. Elevated Non-Essential Metals and the Disordered Metabolism of Essential Metals Are Associated with Abnormal Pregnancy with Spontaneous Abortion Environ. Int.202014410606110.1016/j.envint.2020.10606132890886 · doi ↗ · pubmed ↗