Mindfulness-Based Interventions to Implement the Psychological Well-Being of Nursing Students: A Scoping Review
Milena Consorte, Elena Morotti, Fabio Nanni, Alessandro Giannandrea, Stefano Benini, Monica Martoni

TL;DR
This review explores how mindfulness practices affect nursing students' well-being, finding varied approaches and a focus on stress reduction rather than broader psychological benefits.
Contribution
The study maps existing mindfulness interventions for nursing students and highlights gaps in exploring positive well-being outcomes and standardization.
Findings
Mindfulness interventions for nursing students show heterogeneity in design and delivery.
Most studies focus on stress and anxiety, with less attention to positive outcomes like empathy and self-efficacy.
Online delivery of interventions has increased post-COVID.
Abstract
What are the main findings? Mindfulness-based interventions (MBIs) are increasingly integrated into nursing education; however, substantial heterogeneity exists in intervention protocols, duration, delivery modes, and facilitator training.The majority of studies focus on reducing psychological distress, whereas outcomes related to positive psychological well-being and core nursing competencies remain underexplored. Mindfulness-based interventions (MBIs) are increasingly integrated into nursing education; however, substantial heterogeneity exists in intervention protocols, duration, delivery modes, and facilitator training. The majority of studies focus on reducing psychological distress, whereas outcomes related to positive psychological well-being and core nursing competencies remain underexplored. What are the implications of the main findings? Future research should broaden…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
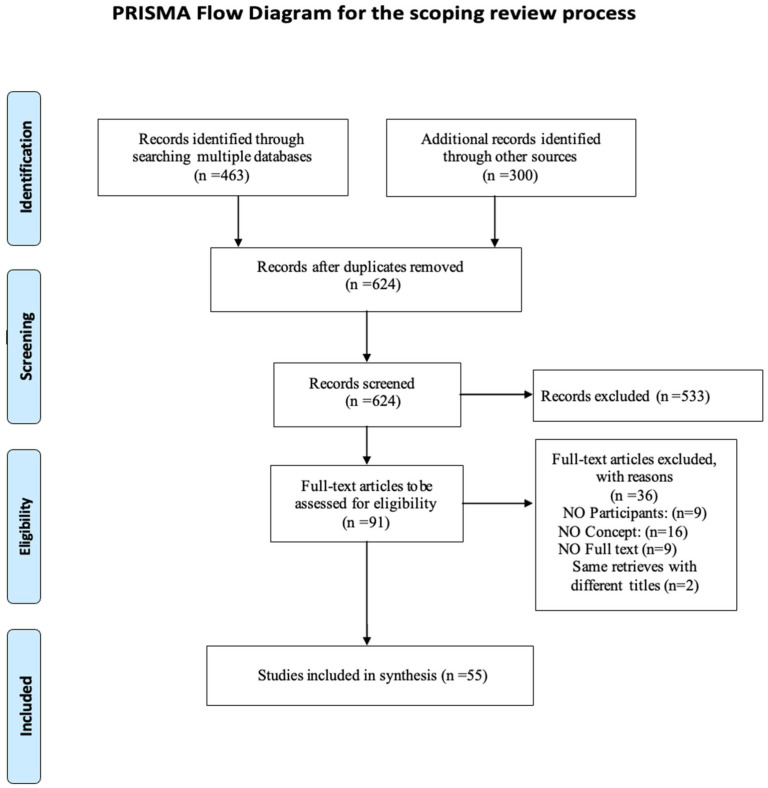 Figure 1
Figure 1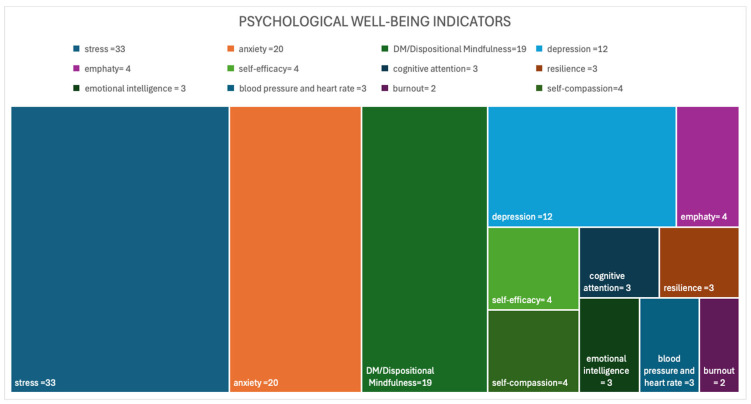 Figure 2
Figure 2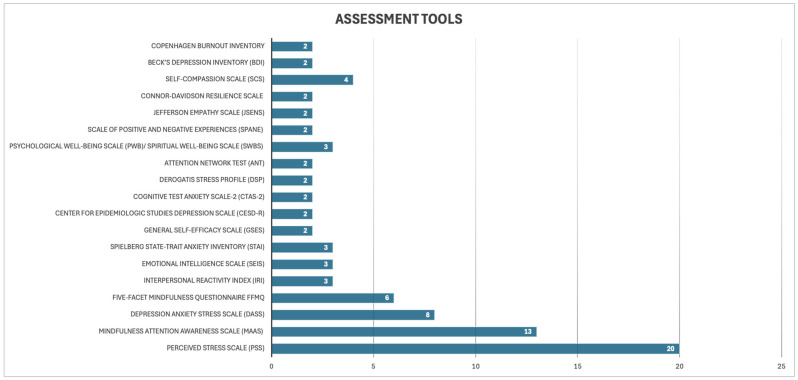 Figure 3
Figure 3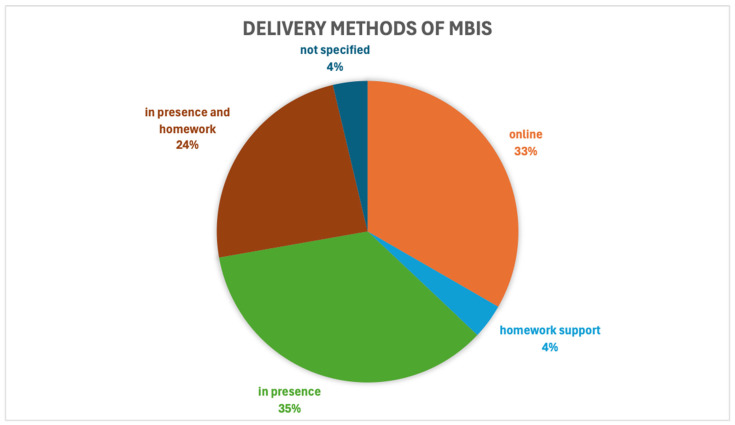 Figure 4
Figure 4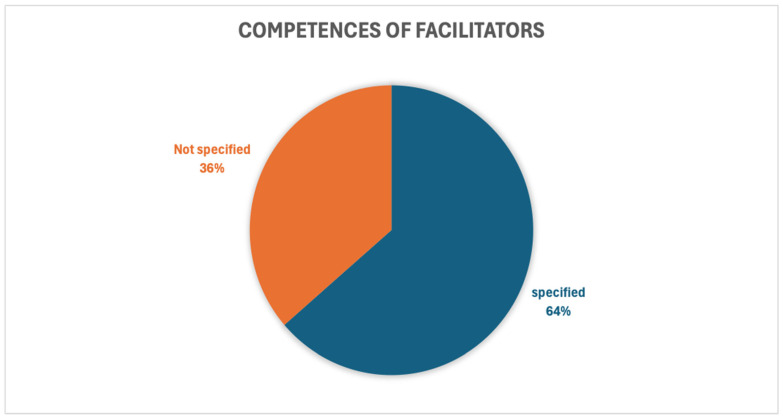 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMindfulness and Compassion Interventions · Healthcare professionals’ stress and burnout · COVID-19 and Mental Health
1. Introduction
For nursing students, the concept of “self-care” is associated with Dorothea Orem and her self-care theory. From a universal perspective, nursing care ideally aims to promote the patient’s full intellectual, emotional, spiritual, and physical well-being [1]. However, caring for others requires nurses to invest a significant physical, cognitive, emotional, and relational resources. For this reason, the construct of “self-care” should be understood as having a double value, encompassing both intra and interpersonal dimensions, because one’s ability to take care of others effectively is closely connected to one’s ability to care for oneself [2].
Over the years, the concept of self-care has become increasingly important in the nursing profession, as the extent to which this population is subject to repeated stressors has become apparent [3,4,5]. This exposes nurses to the risk of developing an increasing degree of compassion fatigue [5,6,7], which can negatively affect not only their health, but also the quality of care provided [8,9]. This reflection transforms the need to reduce the risk of psychological distress and compassion fatigue into an ethical and deontological duty. Care must be focused first and foremost on the professional, in order to preserve and renew the energy that will be expended in the process of caring for those receiving assistance. In other words, only by reserving a space for ourselves will we be able to welcome the being of others [1].
In this regard, the great intuition of theorist Jean Watson, founder of the Human Caring theory, is precisely to address the concept of care within this dual vision. Watson places care at the centre of her thinking. In her theory, Watson identifies a deep correlation with the thinking of important philosophers such as Heidegger, who defines care as a fundamental ontological phenomenon [10], and Levinas, with his Ethics of Belonging [11,12]. Building on this philosophical foundation, Watson emphasizes that caring for oneself is inseparable from caring for others. This conceptual bridge paves the way for self-care practices that resonate with mindfulness, understood as an attitude of presence and compassion in the here and now [13].
The importance of these practices becomes even more evident when considering that nursing students are subjected to higher levels of stress than their peers in other disciplines, mainly due to academic demands and clinical placements [14]. Since the COVID-19 pandemic, the importance of self-care has become even more apparent. Among the various self-care practices, mindfulness-based interventions (MBIs) introduced as part of university courses have consistently shown positive effects on students’ psychological well-being [15]. Mindfulness has been operationally defined as “the awareness that arises from paying attention in a particular way: intentionally, in the present moment, and non-judgmentally” [16]. A multicenter cross-sectional study conducted in Northern Italy in 2020 reported that approximately 70% of nursing students experienced significant psychological distress. However, students with higher dispositional mindfulness (DM) showed lower levels of distress. Based on these findings, the authors suggested integrating mindfulness courses specifically tailored for nursing students in their curricula as a protective factor against stress [17]. In addition, dispositional mindfulness is associated with key relational competencies. Higher DM levels are positively correlated with perspective taking and empathic concern and negatively related to personal distress. Nursing students with higher levels of DM appear better able to understand others’ perspectives, experience compassion, and manage emotional discomfort in challenging interpersonal situations. Consequently, ad hoc mindfulness intervention may support the development of functional empathy within university programmes [18].
Mindfulness practices involve intentionally focusing attention on the present moment, including breathing, body sensations, thoughts and emotions, and the environment around us. This attentional focus reduces ruminative thinking about the past and anxiety-provoking anticipations of the future, such as concerns related to academic and clinical performance. Present moment awareness fosters an approach to care grounded in listening, acceptance, and empathy, thereby enhancing the quality of the helping relationship [19]. Mindfulness-based interventions (MBIs) are recognized as a protective factor against psychological distress associated with clinical practice and academic demands in nursing education. Their relevance extends beyond stress reduction, as they align with the evolving nursing paradigm that emphasizes holistic and person-centred care rather than a purely technical approach [20]. In this context, mindfulness is closely related to self-care and has been linked to constructs such as resilience and compassion [21]. Despite a growing interest in MBIs, from an initial analysis of the literature, studies investigating the effects of mindfulness interventions on nursing students refer exclusively to stress and anxiety. Other dimensions of psychological well-being, such as self-efficacy, empathy, resilience, emotional intelligence, and compassion satisfaction have received limited attention.
As of December 2023, preliminary research conducted on MEDLINE, the Cochrane Database of Systematic Reviews, and Joanna Briggs Institute Evidence Synthesis databases identified no systematic reviews specifically addressing mindfulness-based interventions aimed at promoting psychological well-being among nursing students. Two systematic reviews closely related to this topic were identified, but both had a narrower or different focus. The review by Aloufi et al. [22] examined MBIs primarily in relation to the reduction in stress, anxiety, and depressive symptoms among undergraduate nursing students [22]. While demonstrating the potential effectiveness of MBIs in managing psychological distress, the review focused almost exclusively on symptom reduction and did not explore broader dimensions of psychological well-being or positive psychological outcomes. Similarly, the Cochrane review by Kunzler et al. [23] investigated psychological interventions designed to foster resilience among healthcare students [23]. However, this review included a wide range of heterogeneous interventions, with mindfulness-based approaches representing only one component, and did not provide a specific or comprehensive analysis of MBIs or their multidimensional outcomes. Furthermore, the population was mixed and did not include only nursing students. Consequently, an important gap remains in the literature regarding how mindfulness-based interventions have been specifically applied to nursing students and which outcomes related to psychological well-being have been investigated beyond stress and anxiety.
A scoping review (ScR) is therefore warranted to describe the types of mindfulness-based interventions implemented in this population. This scoping review aims to map all examined psychological well-being outcomes—both positive and negative—and the assessment tools used. Addressing this gap will contribute to a more comprehensive understanding of the role of mindfulness in nursing education and inform future research and educational programme development.
2. Methods
The research was conducted adhering to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews—PRISMA-ScR- guidelines (Supplementary File S1: PRISMA checklist) and in accordance with Peters’ framework, as indicated by the methodology of the Joanna Briggs Institute [24,25,26].
The objectives, inclusion criteria and methods were specified in an a priori scoping review protocol registered on the Open Science Framework (https://osf.io/) on 10 March 2024, available at the link https://osf.io/7ek8d.
2.1. Review Question(s)
Primary question:
-
-Which mindfulness-based interventions (MBIs) are administered to nursing students to implement their psychological well-being (e.g., increased level of awareness, resilience, empathy, emotional intelligence, self-care, compassion satisfaction, compassion fatigue, reduced stress, anxiety, and self-efficacy)? Sub-questions:
-
-Are the periods in which they are administered (academic year, internship, theoretical lessons, laboratory activities) specified?
-
-Are any adverse events reported in studies that included mindfulness-based interventions for nursing students?
-
-What measurement tools are given to students to assess the outcomes of mindfulness-based interventions (MBIs)?
-
-Are the competencies of the mindfulness facilitator administering the intervention specified?
2.2. Eligibility Criteria
PCC eligibility criteria were used. The PCC mnemonic stands for Population, Concept, and Context [26].
Population: The scoping review considered studies that refer to pre-licence and undergraduate nursing students. Studies that refer to undergraduate students of other degree programmes (medicine, psychology, physiotherapy, obstetrics and the like), postgraduate nursing students, or master’s and doctoral degree programmes in Nursing were excluded.
Concept: The scoping review considered studies that refer to all types of mindfulness-based interventions, and included mindful self-compassion, teaching methodologies, and tools (face-to-face workshops, online programmes, seminars, interventions, or self-study programme formats). In addition, the included studies had to describe the outcomes obtained and the competencies of the MBIs trainer. Descriptive studies of students’ mental health that only suggest the need for new approaches to implement their well-being were excluded.
Context: The scoping review considered studies that relate to bachelor and pre-licensure programmes in Nursing. International studies from all countries, written in English, with an abstract and full text, that encompass the eligibility criteria of the scoping review were included.
Types of Sources
Experimental and quasi-experimental studies were included, as well as qualitative and mixed methods studies in which mindfulness-based interventions were administered to undergraduate nursing students. In addition, grey literature, i.e., dissertations and theses, which adhered to the eligibility criteria of the scoping review was also considered. Systematic reviews were excluded but their reference sections were analyzed in order to identify relevant studies that did not emerge from the search strategy.
2.3. Search Strategy
In January 2024, the first phase of the search was conducted on MEDLINE (PubMed) and CINAHL (EBSCO) to identify topic-related titles and abstracts according to the PCC framework. Text words from relevant abstracts were selected and evaluated to identify keywords. The search string was adapted accordingly for each database (Appendix A).
The second phase of the search was conducted from 11 March to 15 March 2024, in the databases PubMed, ERIC (Ovid), CINAHL (EBSCOhost), PsycINFO (Ovid), and ProQuest. In the stated time frame, the search for other sources also included Google Scholar (years > 2020 for feasibility reasons). The following limits were applied: abstract and full text available, English language. Articles published after 15 March 2024, were not included.
The third phase of the search examined the references section of reviews to include articles, with abstracts and full text, that did not emerge from the database searches. When clarification related to the PCC was required, the author of the article was contacted; the specified response time was seven days; failure to respond within this time frame resulted in exclusion of the article.
2.4. Study/Source of Evidence Selection
The selection process is reported in the PRISMA-ScR-Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping review flowchart [24], including the reasons for the exclusion of the articles which did not meet the inclusion criteria (Figure 1, Section 3).
All identified records were collected in a Microsoft Excel spreadsheet and duplicates were removed. Each title and abstract (TI/AB) was then independently screened by the three reviewers (M.C., E.M., F.N.) for evaluation against the inclusion criteria. Potentially relevant items were recovered in full. The subsequent full-text screening phase, conducted by the three reviewers (M.C., E.M., F.N.), further reduced the number of articles included. Disagreements that arose between the reviewers, at any phase of the selection process, were resolved through discussion or by requesting the intervention of an additional reviewer (M.M.).
2.5. Data Extraction
For the data summary, the data extraction table presented in the protocol has been partially modified: the section dedicated to secondary objectives (not explained in the studies) has been removed; the publication country, conclusions, and limitations have been added.
2.6. Data Analysis and Presentation
Graphs were used as synthesis tools, in particular for data related to the distribution of sources by country of origin, outcomes, and the most frequent assessment tools. A descriptive summary accompanies the graphical results and outlines how the results relate to the objectives and questions of the scoping review.
3. Results
3.1. Search Results
Of the 763 articles that emerged, 55 were included in the scoping review. The PRISMA—for scoping review flowchart (Figure 1) shows the screening process.
After the removal of duplicates, three independent reviewers (M.C., E.M., F.N.) evaluated the titles and abstract (TI/AB). At this stage, most of the excluded articles were cross-sectional studies that correlated dispositional mindfulness with outcomes associated both positively and negatively with the psychological well-being of nursing students. Other excluded articles concerned mixed populations or interventions that were not truly mindfulness based. The subsequent selection of the full texts further reduced the number of articles as they did not fully meet the eligibility criteria.
During the third phase, which involved reviewing the references of systematic reviews excluded from this scoping review, two relevant articles were identified. These were subsequently included among the records from other sources, which primarily consist of doctoral theses.
3.2. Inclusion of Sources of Evidence
Some articles did not provide complete answers to the scoping review questions; therefore, one reviewer (M.C.) contacted the authors by email to request additional information. The authors of the doctoral dissertations could not be contacted because no email address for correspondence was available. For journal articles, e-mails were sent to the corresponding authors, to request clarification in relation to the scoping review questions. Of these, nine out of 29 responded within the specified time frame of one week [27,28,29,30,31,32,33,34,35]; for three authors, the correspondence email address was not valid [36,37,38]. In order to gain broader mapping, however, the reviewers decided to include all sources, as the missing information pertained to secondary questions only.
3.3. Review Findings
In this section, the aggregate results are presented in narrative, tabular and graphic form. The data were extrapolated from the data extraction table (see Supplementary File S2: DATA EXTRACTION TABLE ScR) and presented in tabular or graphic form by one of the authors (M.C).
3.3.1. Study Characteristics
In the ScR we have included 37 journal articles (67%) [19,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62] and 18 doctoral dissertations (33%) [63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80]. Of the studies included, most were conducted in the United States of America. The origin of all the articles is shown in Table 1.
As for the distribution by year, an increase from the year 2022 onwards was evident. This increase could depend on two factors: the pandemic period which induced a focus of attention on certain topics; Google Scholar research that was conducted within a time limit (>2020) for feasibility reasons.
Among the study designs we find a prevalence of quasi-experimental studies (40%) [29,34,35,47,48,49,50,52,53,55,59,60,61,62,64,67,70,71,73,76,78,79] and Randomized Controlled Trials or RCTs (38%) [31,33,36,37,38,39,40,41,42,44,46,51,54,56,57,63,66,68,69,72,80]; Mixed-Method studies appear for 16% of sources [19,27,28,32,58,65,74,75,77]; qualitative studies for 5% [30,43,45].
3.3.2. Participants in the Studies
In relation to the number of participants, the panorama of articles is very varied: the sample size ranged from five [34] to 201 students [19]. Regarding the doctoral dissertations the sample size ranged from nine [71] to 203 [70]. The total of participants who began the studies is 4320, and the total of participants who did not complete required activities or withdrew before the end of the studies is 799. The problem of dropout rate is common to many studies. This may be attributed to the low adherence of students due to commitments.
3.3.3. Mindfulness-Based Interventions Applied
The MBIs found in the studies are numerous and differ in terms of type, investigated outcomes, duration and mode of delivery. Thirteen studies are inspired by the MBSR, Mindfulness-Based Stress Reduction [27,31,35,38,51,52,54,59,60,67,76,78], lasting eight weeks, and two of these were carried out in online mode [54,59]. Two studies applied Koru Mindfulness Meditation [66,77], which is based on practices such as diaphragmatic breathing, breath awareness, dynamic breathing, body scanning, mindful walking, Gatha meditation, guided imagery, and thought/feeling labelling. Among the remaining studies, four focused on heterogeneous Mindful Self Compassion (MSC) protocols, whereas the others proposed interventions based on Mindfulness Meditation are proposed. See Table 2 for further details.
In the included studies there are some interventions (30%) lasting longer than 8 weeks [27,30,31,32,37,38,42,48,52,59,62,68,79,80], 10 weeks [40], or 12 weeks [49,51] and many are shorter in duration. The most common interventions are unstructured and involve sporadic practices implemented in preparation for an examination or a lesson. Shorter interventions are often related to self-control before a cognitive or motor performance and last from two minutes or less [33,70], or three minutes [58,63], up to nine hours over two days [50].
3.3.4. Outcomes
The most frequently investigated indicators remain those negatively associated with psychological well-being: stress (30.0%), anxiety (18.2%) and depression (10.9%). Dispositional mindfulness is the only positive indicator that is investigated quite frequently; it appears 19 times (17.3%) in the research included in the scoping review. Figure 2 describes the most frequently investigated outcomes in the studies.
3.3.5. Assessment Tools
The results are followed by measurement scales. The most frequently used scales in the studies included are the Perceived Stress Scale (PSS), which measures perceived stress levels [81]; the Mindfulness Attention Awareness Scale (MAAS) for dispositional mindfulness [82]; the Depression Anxiety Stress Scale (DASS) that measures depression, anxiety, and stress, which are often associated with each other [83]. PPS and MAAS were used 20 and 13 times, respectively. Figure 3 descrbes the assessment tools that are most frequently used in studies.
A comprehensive overview of the study characteristics is presented in Table 2, including first author, year of publication and country, study design, sample Size and dropout rate, experimental group intervention, control group intervention, outcome measures (variables), finding and publication type.
3.3.6. Delivery Method of Mindfulness-Based Interventions
In included studies, the most common delivery method of MBIs is face-to-face [19,30,33,36,37,39,40,43,44,45,48,50,56,58,60,62,67,75,80]. There is a significant propensity for face-to-face interventions with Supplementary Materials for home practice [27,29,31,34,35,38,42,51,52,53,68,72,76]. However, a shift toward online delivery is evident, especially in publications after 2021, a trend that was probably due to social restrictions during the COVID pandemic. In fact, 15 out of 18 [28,32,46,49,54,55,57,61,64,65,70,73,74,77,79] studies, the total of those applying online modalities, were conducted from 2021 to 2024 (compared to three studies with online interventions before 2021) and of these only five sources come from Google Scholar (for the time filter applied).
In addition to online MBIs, protocols built ad hoc for the population examined, administered on IT platforms (institutional and non-institutional) and applications for smartphones and videos on YouTube were offered. The different delivery methods are represented in Figure 4.
3.3.7. Competencies of the Facilitators of Mindfulness-Based Interventions
Albeit very heterogeneous, the competencies of the facilitators involved in mindful-based interventions are specified in most studies (64%), as shown in Figure 5. Out of a total of 55 studies, 19 did not specify the level of competence of the facilitator [19,27,39,40,47,53,55,56,58,59,63,64,69,73,74,75,77,78,79]; of these studies, seven were administered online [55,59,64,73,74,77,79]. In most of the remaining 36 studies, the trainers were mindfulness facilitators with certification at different levels and personal experience of practice, with the exception of three studies in which they were psychiatrists [46,52,66], two sources in which they were psychologists [36,50], and two articles in which they were cognitive behavioural therapists [51,54].
3.3.8. Adverse Events
In the papers included in this ScR, two articles examined this topic and ruled out the presence of adverse events [50,71]. However, one of these articles reported a possible risk of emotional dependency among students [50]. For the other articles, eight authors provided additional information in response to our e-mail request for clarification. They reported that participants did not experience any significant adverse events [28,29,30,31,32,33,34,35]. In one clarification, it was noted that some students fell asleep during the practice [30]; in another, a student, who described himself as generally anxious, reported increased awareness accompanied by elevated stress levels. Despite this adverse experience, the student continued and completed the course [35]. In the latter case, the intervention was an adapted MBSR programme, consisting of two-hour sessions held twice a week for four weeks. The remaining papers did not address the issue of adverse events related to the mindfulness-based intervention.
3.3.9. Intervention Characteristics
Table 3 presents the intervention characteristics of the included studies, including MBIs duration, mode of delivery, links to website or mobile apps, reported adverse events, facilitators’ competence, and the context in which the interventions were applied.
4. Discussion
The importance of integrating a mindfulness-based approach into nursing curricula has been clearly and exhaustively explained by Beddoe & Murphy [27], who frame mindfulness as a response to core questions in nursing education: how we care for ourselves, how we compassionately care for others, and what values should guide professional training. Central to this perspective is the recognition that compassion which excludes oneself is incomplete [84]. In line with this framework, the findings of the present scoping review suggest that MBIs offer added value to the education of nursing students. However, the review also highlights substantial heterogeneity in the types of interventions implemented, and in the outcomes assessed. In the studies included in this ScR, the predominant indicators are always those associated with psychological distress, such as stress, anxiety, and depression. Variables that are positively associated with psychological well-being are investigated in only 37.3% of research. This result is in line with previous systematic reviews conducted in the same population of interest [22,85,86]. Having extensively studied the effects of MBIs on distress reduction, future research should broaden its focus to outcomes that are more closely aligned with the relational and humanistic dimensions of nursing practice.
Carl Rogers, founder of the Theory of Counselling, summarized the main qualities for person-centred care—empathy, active listening skills, and authentic presence—that are closely connected to mindfulness and positive mediators of psychological well-being. These qualities may buffer against compassion fatigue. An authentic helping relationship enhances compassion satisfaction (ProQOL manual https://proqol.org/proqol-manual; accessed on 22 November 2025), with a direct impact on professional well-being and quality of the care provided. In this context, the inclusion of Mindful Self-Compassion in nursing curricula appears particularly relevant. Nevertheless, only two studies introduce MSC interventions [54,86]. Furthermore, the protocols adopted were not comparable, limiting conclusions regarding their effectiveness.
Another critical issue emerging from this ScR concerns the mode of delivery (in-person or online) and intensity of MBIs. Many interventions were designed as brief online programmes to increase accessibility and reduce student dropout [45,59]. Brief bursts of MBIs administered through devices, however, generated conflicting results. In fact, it is difficult for educators to try to calibrate the duration of the protocols that they should offer, particularly in light of clinical and academic commitments. These findings are in line with those of Jimènez et al. [87], who showed that low-intensity MBIs (lasting between 8 and 15 min per meeting) can produce statistically significant effects on outcomes such as rumination, distraction, and impulse control [88,89]. The review concludes with the suggestion that new research should be carried out on the effects of short MBIs on larger samples so that these techniques can be incorporated into clinical practice. This conclusion leads to the third critical issue found in this ScR: most studies relied on small and convenient samples. In addition, most of them lacked follow-up assessment to evaluate the maintenance of the outcomes obtained and their impact on the quality of care.
The issue of adverse events also warrants attention. The majority of studies included in this review did not report negative outcomes, particularly when low-intensity interventions were used. The isolated reports of increased stress or discomfort were associated with higher-intensity programmes. Consistent with the work of Baer et al. [90], the safety of MBIs appears to depend on practice intensity, participant vulnerability, and facilitator expertise. This finding underscores the importance of adequately trained instructors and careful adaptation of intervention intensity to the student population.
Consistent with the work of Baer et al. [90], of the Oxford Mindfulness Centre, the safety of MBIs appears to depend on practice intensity (expressed in terms of daily commitment required and exploratory depth of self), intrinsic factors of the participant (susceptibility to frequent manifestations of psychological distress or recurrent depression), and intrinsic factors of the trainer, such as experience, professionalism, the ability to lead a group, and the embodiment of meditative practice. Baer et al. [90] identify low-intensity interventions as those that direct attention to the capacity for awareness in sensory perception. Generally, these types of MBIs are not associated with personal injury. Their research does not show adverse events linked to moderate-intensity practices, although research in this field is still in its infancy. MBSR or MBCT programmes can be considered moderate-intensity interventions, and it would be desirable for them to be conducted by experienced professionals (e.g., psychologists, psychotherapists) in order to manage the possible occurrence of adverse events. The use of the conditional is necessary, given the wide variability in trainers’ expertise across current programmes. High-intensity practices are defined as residential meditation retreats where generous commitment is required from participants, such as prolonged silences and daily meditations lasting hours. In line with the findings of the review by Baer et al. [90], facilitator training also varied greatly across the sources included. This variability further complicates comparisons between interventions and highlights the need for clearer reporting standards in future research. Despite these limitations, there is broad consensus across the literature on the value of integrating MBIs into nursing curricula, not only to mitigate academic and clinical stress, but also to enhance compassion satisfaction and professional well-being.
4.1. Intervention Characteristics and Outcomes of MBIs
In relation to the intervention characteristics summarized in Table 1 and Table 2, the effectiveness of mindfulness-based interventions (MBIs) appears to vary systematically according to programme structure, duration, and facilitator competence. More structured and longer interventions, such as Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cognitive Therapy (MBCT), and Koru-based programmes, are more frequently associated with statistically significant improvements in stress, anxiety, emotional regulation, empathy, and self-care outcomes [27,29,31,35,38,44,51,52,66,80]. These effects are predominantly reported in studies involving trained or experienced facilitators and sustained engagement over several weeks, often combined with regular home practice [44,51,52,66]. However, such interventions also entail higher demands in terms of time commitment and organizational resources, which may limit their feasibility and attractiveness within academic curricula [27,51,52].
In contrast, mindfulness meditation interventions centred on sensory awareness and brief guided practices show more heterogeneous results. While several studies report statistically significant improvements in stress, anxiety, or dispositional mindfulness [36,39,40,41,46,55,61,69,75], others yield non-significant quantitative findings despite positive qualitative feedback, including increased calmness, attentional focus, and emotional centring [19,28,32,43,65]. These interventions appear to be more adaptable in terms of duration and delivery format, including online and hybrid modalities, potentially enhancing accessibility within nursing education programmes [32,41,46,49,64].
Very brief MBIs administered immediately before academic activities or examinations demonstrate mixed effectiveness. Although these interventions are highly feasible and time-efficient, quantitative outcomes are often modest or non-significant [28,63,65,70,73], possibly due to insufficient depth of practice and implementation challenges, such as limited faculty engagement and variable student adherence. Overall, the evidence summarized in Table 1 and Table 2 suggests that the effectiveness of MBIs in nursing education is not inherent to mindfulness practice alone, but is closely moderated by intervention intensity, facilitator expertise, delivery context, and opportunities for sustained practice.
4.2. Limitation of Scoping Review
This scoping review presents some methodological limitations. First, the data extraction tool was refined after the review process had commenced, as the original version proposed in the protocol had not been piloted. The modifications were necessary to adequately capture the heterogeneity of mindfulness-based interventions and outcomes identified and were transparently reported in line with JBI guidance. Second, the literature search was completed in March 2024; therefore, studies published thereafter were not included, and more recent evidence may not be represented in the present review. This temporal limitation highlights the need for future updates of the evidence as the field continues to evolve. In addition, filters such as restriction to the English language and a temporal filter for Google Scholar (>2020) were applied for feasibility reasons. This may have reduced the number of sources included in this ScR.
A further limitation of this scoping review is that, in accordance with JBI and PRISMA-ScR guidance, it did not aim to evaluate the effectiveness of mindfulness-based interventions. Consequently, the review provides a descriptive synthesis of reported outcomes rather than a critical appraisal or effect-size estimation. While this approach is consistent with the purpose of scoping reviews, it highlights the need for future systematic reviews and meta-analyses to assess the effectiveness of MBIs once more methodologically homogeneous studies become available.
4.3. Methodological Limitations of the Existing Literature
This review identified several methodological limitations that constrain the interpretability and transferability of current evidence. Most studies relied on small, non-probabilistic convenience samples, reported high dropout rates, and lacked follow-up assessments to evaluate the sustainability of outcomes over time. In addition, outcome measures were predominantly self-reported, limiting the ability to assess the impact of MBIs on observable clinical or educational outcomes.
Another relevant limitation concerns the heterogeneity of intervention protocols, delivery formats, and facilitator training. This variability complicates comparisons across studies and limits the identification of best practices. Furthermore, although most studies reported no adverse events, the inconsistent reporting of negative or unintended effects represents an additional methodological weakness.
4.4. Implications for Education and Practice
The findings of this scoping review highlight the growing integration of MBIs within nursing education, while also revealing a lack of conceptual alignment between intervention objectives and the core values of the nursing profession. Although MBIs are predominantly implemented to reduce psychological distress, and their potential to foster positive psychological resources—such as empathy, self-efficacy, compassion, and emotional intelligence—remains underutilized.
From an educational perspective, these findings suggest that MBIs should be more explicitly framed as formative tools supporting professional identity development, relational competence, and sustainable self-care, rather than solely as stress-management strategies. Integrating mindfulness and mindful self-compassion within curricula may contribute to preparing students for emotionally demanding clinical environments and enhance compassion satisfaction, with potential downstream effects on quality of care.
The integration of self-care and mindfulness-based interventions directly into undergraduate nursing curricula may represent a key strategy for enhancing student engagement and adherence. Voluntary or extracurricular participation may be associated with variable attendance and inconsistent practice, whereas curricular integration can normalize self-care as a core professional competence and promote sustained engagement over time. Moreover, the analysis of intervention characteristics indicates that programmes adopting a structured and theory-informed approach to self-care activities are more consistently associated with positive outcomes across psychological, emotional, and professional domains.
These observations highlight the potential value of developing a population-specific protocol tailored to nursing students. An ad hoc protocol could contribute to greater standardization of intervention components (e.g., duration, intensity, facilitation, and practice requirements), thereby improving comparability across studies and strengthening the overall evidence base. In addition, a structured, curriculum-embedded protocol may support adherence by aligning self-care practices with educational objectives and assessment frameworks, reinforcing their relevance within professional training rather than positioning them as optional or ancillary activities.
4.5. Implications for Future Research
The gaps identified in this scoping review indicate several priorities for future research. Among these is the need to broaden the domains of outcomes beyond psychological distress to include positive indicators of well-being in line with nursing competencies (e.g., empathy, compassionate satisfaction, self-efficacy, emotional intelligence). In addition, it will be useful to conduct research with greater methodological rigour, using larger samples and longitudinal designs with follow-up assessments to examine the maintenance of outcomes and their impact on educational and clinical practice. Consequently, it is appropriate to optimize the measurement of outcomes by integrating self-reported data with observational or patient-reported measures, particularly with regard to compassionate care. The characteristics of the intervention must be clear in future research, including intensity, duration, mode of delivery, and facilitator training, to support reproducibility and implementation. Feasibility and acceptability must be assessed at the organizational level, addressing institutional readiness, cultural barriers, and resource implications in nursing education. It is important to emphasize that, once a sufficiently homogeneous body of evidence is available, future research projects, such as systematic reviews or meta-analyses, will be needed to evaluate the effectiveness of MBIs.
5. Conclusions
The aim of this ScR was to map the existing literature on mindfulness-based interventions designed for nursing students and their association with psychological well-being. The findings reveal substantial heterogeneity in intervention types, delivery formats, and outcome measures. Most studies focused on reducing psychological distress, while indicators positively associated with well-being, such as self-efficacy, empathy, compassion, and emotional intelligence, remain underexplored. Future research should prioritize these outcomes, as they reflect core competencies of the nursing profession. Expanding the evidence base on MBIs will support their integration within university programmes.
However, successful implementation requires addressing cultural and organizational barriers. In order for both educators and students to invest in and benefit from self-care practices, it is important that they feel confident that they can take care of themselves during work and study, and that they can also feel free to share emotional difficulties among peers, dispelling the fear that adherence to such practices could influence the achievement of goals. Unfounded concerns that associate self-care practices during study or work with lack of productivity must be refuted. If these factors are not addressed, engagement in the programme may be jeopardized [91]. Consistent with Waddell et al. [92], existing studies primarily target individual-level factors, often neglecting organizational and systemic dimensions. Therefore, future research should include feasibility studies to assess institutional readiness, educator and student attitudes, perceived barriers, and preferred delivery formats. Understanding these factors is essential to identifying which MBIs are most appropriate and sustainable within nursing education. The road to future research, therefore, still has a long way to go.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mortari L. La Pratica Dell’aver Cura, Ediz My Lab Milano/Torino, Italy 20229788891930996 B
- 2Mills J. Wand T. Fraser J.A. On self-compassion and self-care in nursing: Selfish or essential for compassion-ate care?Int. J. Nurs. Stud.20155279179310.1016/j.ijnurstu.2014.10.00925457876 · doi ↗ · pubmed ↗
- 3Chesak S.S. Morin K.H. Cutshall S.M. Jenkins S.M. Sood A. Feasibility and efficacy of integrating resiliency training into a pilot nurse residency program Nurse Educ. Pract.20215010295910.1016/j.nepr.2020.10295933454511 · doi ↗ · pubmed ↗
- 4Davidson J.E. Proudfoot J. Lee K. Terterian G. Zisook S. A longitudinal analysis of nurse suicide in the United States (2005–2016) with recommendations for action Worldviews Evid.-Based Nurs.20201761510.1111/wvn.1241932017434 · doi ↗ · pubmed ↗
- 5Xie W. Chen L. Feng F. Okoli C.T.C. Tang P. Zeng L. Jin M. Zhang Y. Wang J. The prevalence of compassion satisfaction and compassion fatigue among nurses: A systematic review and meta-analysis Int. J. Nurs. Stud.202112010397310.1016/j.ijnurstu.2021.10397334102372 · doi ↗ · pubmed ↗
- 6Ruiz-Fernández M.D. Pérez-García E. Ortega-GalánÁ.M. Quality of Life in Nursing Professionals: Burnout, Fatigue, and Compassion Satisfaction Int. J. Environ. Res. Public Health 202017125310.3390/ijerph 1704125332075252 PMC 7068555 · doi ↗ · pubmed ↗
- 7Zhang Y.Y. Han W.L. Qin W. Yin H.X. Zhang C.F. Kong C. Wang Y.L. Extent of compassion satisfaction, compassion fatigue and burnout in nursing: A meta-analysis J. Nurs. Manag.20182681081910.1111/jonm.1258930129106 · doi ↗ · pubmed ↗
- 8Lluch C. Galiana L. Doménech P. SansóN. The Impact of the COVID-19 Pandemic on Burnout, Compassion Fatigue, and Compassion Satisfaction in Healthcare Personnel: A Systematic Review of the Literature Published During the First Year of the Pandemic Healthcare 20221036410.3390/healthcare 1002036435206978 PMC 8872521 · doi ↗ · pubmed ↗