Role of Dynamic Contrast-Enhanced MRI in Detecting Post-Treatment Local Recurrence of Soft-Tissue Sarcomas: A Systematic Review and Meta-Analysis
Arash Azhideh, Howard Chansky, Peyman Mirghaderi, Sara Haseli, Bahar Mansoori, Navid Faraji, Chankue Park, Shakiba Houshi, Majid Chalian

TL;DR
This study shows that adding dynamic contrast-enhanced MRI improves accuracy in detecting soft-tissue sarcoma recurrence after treatment.
Contribution
The novel contribution is demonstrating that DCE-MRI combined with conventional MRI significantly improves diagnostic accuracy for local sarcoma recurrence.
Findings
DCE-MRI qualitative features and quantitative parameters consistently differentiate local recurrence from post-treatment changes.
Combined DCE-MRI and conventional MRI achieved 98% sensitivity and 83% specificity for recurrence detection.
The SROC area under the curve was 0.94, indicating high diagnostic accuracy.
Abstract
Background: The role of dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) in detecting soft-tissue sarcoma (STS) local recurrence (LR) following therapeutic intervention was evaluated. Method: PubMed, Embase, and Scopus were systematically searched from January 1990 to 1 February 2024 for studies evaluating DCE-MRI for LR detection in histologically confirmed STS following surgery. Two independent reviewers screened studies and extracted data, and a bivariate diagnostic test accuracy meta-analysis was performed to estimate pooled sensitivity, specificity, and the area under the summary receiver operating characteristic (SROC) curve. Results: Six studies, including 309 patients (110 with LR and 199 without LR), met the inclusion criteria. Across studies, DCE-MRI qualitative features (such as early rapid arterial enhancement and malignant time–intensity curves) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
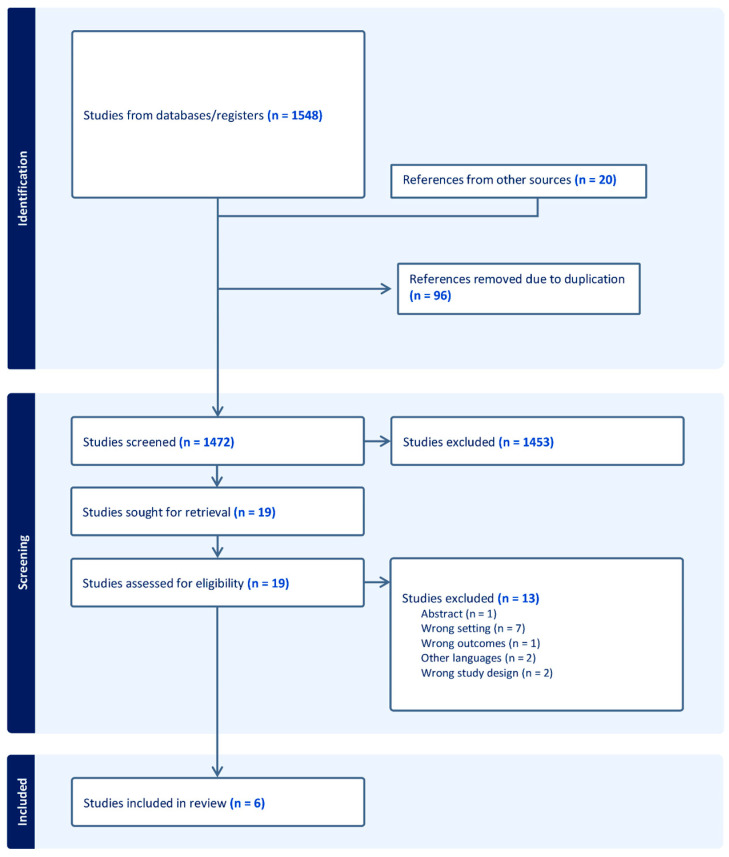 Figure 1
Figure 1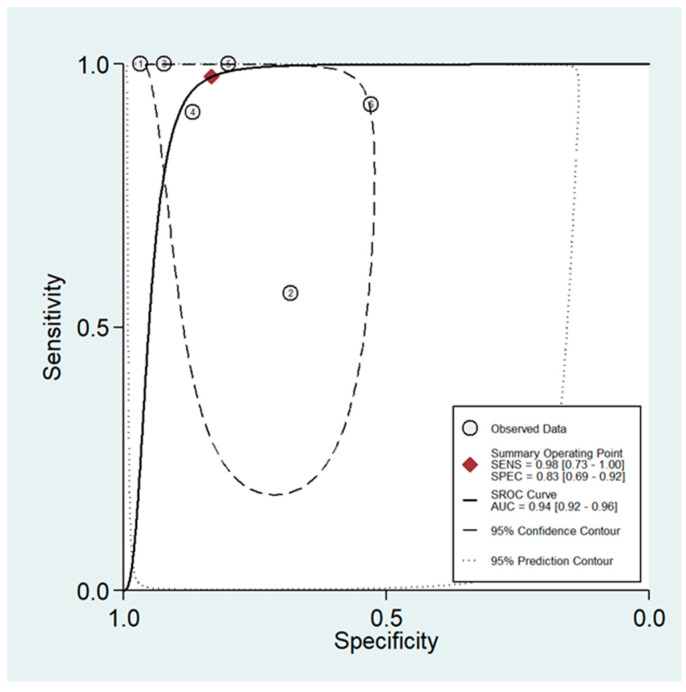 Figure 2
Figure 2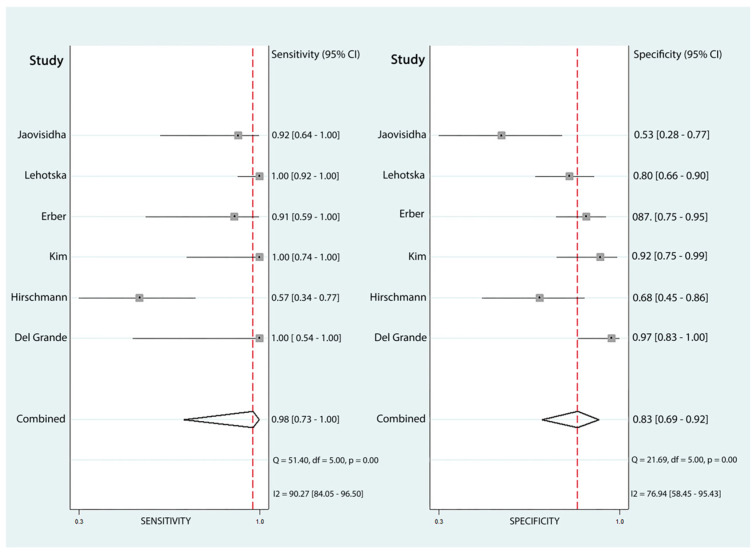 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · MRI in cancer diagnosis · Angiogenesis and VEGF in Cancer
1. Introduction
Soft-tissue sarcomas (STSs) are a rare but clinically significant group of mesenchymal neoplasms, accounting for less than 1% of adult malignancies [1]. Despite multimodal therapeutic strategies in the management of STS, the risk of local recurrence (LR) remains significant [2]. Risk factors for LR include patient age, tumor size, histological subtypes, absence of pre-operative radiotherapy, and positive surgical margins [3]. The incidence of LR has been documented to range from 6.5% to approximately 50%, with an average of about 20% [4]. Early detection of LR is critical to reduce morbidity and the need for extensive re-excisions and the development of further metastasis. Distinguishing LR from post-operative changes, such as scar tissue or fibrosis, poses a diagnostic challenge due to overlapping features in conventional MRI [5,6]. The complete absence of high signal intensity in the surgical bed in fluid-sensitive images has been suggested to be an excellent sign to exclude tumor recurrence, although LR might occasionally present with a hypointense signal in fluid-sensitive sequences. Other features like architectural distortion and signal intensity in both T1- and T2-weighted imaging are not typically distinguishing [5,6]. Functional MR techniques like dynamic contrast-enhanced MRI (DCE-MRI) have shown potential in improving diagnostic accuracy by providing additional qualitative and quantitative data regarding the pattern of enhancement, tissue vascularity, and perfusion based on time–intensity curves (TICs) [7,8].
In this systematic review and meta-analysis, we critically review the existing literature to assess the efficacy of DCE-MRI in detecting STS LR following surgical treatment.
2. Materials and Methods
2.1. Search Strategy
This systematic review and meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [9] (Table S1). Its objective was to evaluate the efficacy of DCE-MRI in identifying recurrent STS in post-treatment patients. This review extensively searched major databases, including PubMed, Scopus, Web of Science, Embase, and Google Scholar, starting from their inception, and without any limitations. We searched these databases from 1990 to 1 February 2024. The search strategy was crafted employing Medical Subject Headings (MeSHs) alongside additional search terms using the Boolean operators “AND” and “OR” with a combination of keywords, such as “soft tissue sarcoma”, “MRI”, “dynamic contrast”, “recurrence”, and their alternatives.
2.2. Study Selection
Two postdoctoral researchers with 3 and 5 years of experience independently screened the titles and abstracts identified in the search, followed by retrieval and evaluation of the full texts. The Patient, Intervention, Comparison Group, Outcome, and Study (PICOS) design was applied to select studies that met the following criteria: a. all patients diagnosed with STS by pathology and imaging findings; b. all patients who underwent surgery as treatment for STS; and c. all studies that used DCE-MRI in the follow-up period to assess the accuracy of detecting LR.
Studies were excluded if they used imaging modalities other than DCE-MRI, included fewer than ten patients in the study cohort (to avoid imprecise and unstable diagnostic estimates from very small series), or did not adequately report study endpoints. Animal studies, duplicate studies, conference abstracts, editorials, brief reports, book chapters, and dissertations were excluded.
2.3. Data Extraction
The same reviewers extracted data using standardized data abstraction templates designed with commercially available software (Excel, Microsoft, Redmond, WA). Disagreements at each screening or data extraction stage were first discussed to reach consensus between the two reviewers; if consensus could not be reached, a third reviewer (a fellowship-trained, board-certified radiologist with 9 years of experience) acted as an arbitrator. The data elements extracted from the included studies were as follows: the first author’s name, publication year, region, patient characteristics like age, gender (male/female), and DCE-based parameters, sample size (case/control), follow-up period, and performance metrics consisting of sensitivity and specificity.
2.4. Statistics
A bivariate diagnostic test accuracy (DTA) meta-analysis was conducted to evaluate the pooled sensitivity, specificity, and the summary receiver operating characteristic (SROC) curve. STATA version 14, using the MIDAS command, was employed to calculate the DTA parameters. This command uses a bivariate model that simultaneously considers both sensitivity and specificity.
All studies that reported sensitivity, specificity, case sample size, and control sample size, or provided data from which these metrics could be calculated, were included in this meta-analysis. These data were used to calculate true positives, false positives, true negatives, and false negatives, with the resulting values rounded to the nearest integer. The Cochran-Q test and I^2^ index were applied as indicators of heterogeneity within the meta-analysis, with significant heterogeneity defined as an I^2^ greater than 50% or a Cochran-Q test p-value < 0.10.
2.5. Quality Assessment
For the quality assessment of the included studies, we used the QUADAS-2 (Quality Assessment of Diagnostic Accuracy Studies 2) tool, a widely recognized instrument for evaluating the diagnostic accuracy of studies. It provides a structured approach for assessing the risk of bias and applicability concerns across four key domains: patient selection, index test, reference standard, and flow and timing (Table 1)
3. Results
3.1. Literature Search
The initial literature search identified 1548 studies, of which 96 studies were removed due to duplication. The remaining 1452 studies underwent screening of titles and abstracts, resulting in the exclusion of 1446 studies for reasons such as non-peer-reviewed status (e.g., conference abstracts and poster presentations), review articles, incomplete outcomes, studies involving patients with different pathologies, publications in languages other than English, or different outcome measurements. Ultimately, six unique peer-reviewed scientific studies met the inclusion criteria. The selection process for these studies is illustrated in Figure 1, which includes a flow diagram detailing the study selection methodology.
3.2. Patients’ Characteristics, STS Types, and Study’s Endpoint
The six studies were [5,7,10,11,12,13]. The study cohort, comprising 309 unique STS patients—ranging between 4 and 84 years old—[150 male (53%), 133 female (47%), and 26 (4.3%) unreported], included 110 patients in the case group and 199 in the control group. More characteristics of patients are provided in Table 2. Although different imaging sequences and features were investigated in each study, and not all included studies reported the accuracy of conventional MRI, all of them reported the sensitivity and specificity of DCE-MRI in detecting STS LR. Furthermore, several sequences with different protocols were used to assess the LR, with detailed information provided in Table 3.
Additionally, this review assessed the frequency of recurrent tumors in DCE-MRI in patients diagnosed with various STS types. The most frequently observed STS type across these studies was pleomorphic sarcoma (n = 44), followed by liposarcoma (n = 36), myxofibrosarcoma (n = 24), undifferentiated pleomorphic sarcoma (malignant fibrous histiocytoma) (n = 20), rhabdomyosarcoma (n = 10), malignant peripheral nerve sheath tumor (MPNST) (n = 8), and spindle cell sarcoma (n = 6). Less commonly observed types included myxoid liposarcoma (n = 4), chondrosarcomas (n = 3), and fibrosarcoma (n = 3).
3.3. DTA Meta-Analysis
Six papers with a total of 309 participants were included in this meta-analysis. The pooled sensitivity was 98% (95% CI: 73% to 100%), and the specificity was 83% (95% CI: 69% to 92%). Additionally, the area under the curve (AUC) for the SROC was 0.94 (95% CI: 0.92 to 0.96) out of 1, indicating the high accuracy of DCE-MRI in detecting LR of STS following surgical intervention (Figure 2). The forest plot of included studies evaluating the sensitivity and specificity of DCE-MRI is depicted in Figure 3. However, the heterogeneity of this analysis was high, potentially due to differences in the populations studied, variations in MRI readers, and the use of different imaging protocols and devices.
4. Discussion
This systematic review and meta-analysis evaluated the role of DCE-MRI in detecting LR of STS after surgical intervention, with an emphasis on its diagnostic accuracy and clinical applications. We found that, despite variations in the methods of DCE-MRI used, it demonstrates high sensitivity (98%) and specificity (83%) for LR detection. This suggests that DCE-MRI could potentially be one of the optimal methods for screening LR in cases of STSs. Although conventional MRI is often adequate for the initial evaluation of STS, it has limitations in LR detection, particularly in the early stages following neoadjuvant therapy [5,14,15]. Differentiating post-surgical changes, such as granulation tissue formation and fibrosis/scarring, from residual or recurrent tumors can be challenging [16,17,18,19]. In T1-weighted images, LR characteristically presents as hypointense areas of architectural distortion resembling scarring. Abnormal signal intensity in T2-weighted images may persist in the surgical bed for extended periods due to postsurgical fibrosis/scarring and/or LR. This distinction can be even more challenging when post-operative changes appear mass-like, with nodular areas greater than 5 mm or intramuscular architectural distortion, mimicking LR [5,11,20].
In the broader context of functional oncologic imaging, DCE-MRI provides perfusion and permeability information that is complementary to other advanced techniques such as diffusion-weighted imaging (DWI) and hybrid PET/MRI. DWI interrogates tissue cellularity via apparent diffusion coefficient (ADC) maps and may help distinguish a hypercellular recurrent tumor from predominantly fibrotic post-operative change, while PET/CT or PET/MRI can depict metabolically active disease and simultaneously assess for distant metastases [16]. However, DWI can be limited by susceptibility artifacts and heterogeneous post-operative tissue, and PET-based techniques are less widely available and associated with higher cost and exposure to ionizing radiation. DCE-MRI can be integrated into routine follow-up MRI protocols without additional radiation and, when combined with DWI as in the study by Erber et al., may further increase confidence in distinguishing LR from benign post-operative findings [8,16].
Del Grande et al. retrospectively studied 37 patients with histologically confirmed recurrent STS, most of which were high-grade sarcomas. Morphological characteristics with conventional MRI and the presence or absence of arterial enhancement in DCE-MRI using a time-resolved 3D volumetric sequence were recorded. The study reported a sensitivity of 100% and a specificity of 97% when DCE-MRI was added to conventional MRI. Their study demonstrated a high false-positive rate of conventional MRI in the false detection of LR, leading to nearly half of the cases without recurrence undergoing unnecessary biopsy of the post-operative scar. The authors concluded that DCE-MRI could significantly reduce the false-positive rate and unnecessary tissue sampling [5,15,21].
Both qualitative and quantitative methods can be used to assess tumor vascularity and the adjacent soft tissues. The presence of early arterial enhancement within the first seconds, which is defined by contrast enhancement of the nearby artery, is a common qualitative metric for assessment of STS LR [12,22,23,24,25]. Quantitative methods measure the pharmacokinetics of specific areas using parameters like the shape of the signal intensity curve, time to peak, and pharmacokinetic (PK) contrast enhancement [7,10,11,13,26,27].
Erber et al. prospectively and quantitatively evaluated the diagnostic accuracy of DCE-MRI in detection of LR in post-treatment extremity STSs. They used parameters such as relative plasma flow (rPF) and relative mean transit time (rMTT); their study revealed that rPF was significantly higher in LR compared with expected post-op changes, which makes it a strong indicator of LR [10,28].
Hirschmann et al. studied the role of MRI in detection of clinically silent LR; they focused on the findings of DCE-MRI and knowledge of surgical margins in identifying recurrence prior to the gross appearance of confirmed LR. They conducted a retrospective analysis comparing pre-operative MRI characteristics (both conventional and DCE) of 23 patients with post-treatment MRI taken before confirmed LR. The analysis consisted of morphological assessment in conventional MRI, and enhancement onset, dynamic enhancement pattern, and progression of enhancement type in DCE-MRI. A second analysis assessed LR visibility in post-operative MRI and subsequent third MRI to identify causes of false positives and false negatives. Since the majority of LR lesions were nodular, hyperintense, homogeneous in fluid-sensitive images, and centrally located in the surgical bed, conventional MRI was able to correctly detect 52% of patients, while one additional diagnosis was enabled by DCE-MRI. They also demonstrated that early enhancement—within six seconds—emerged as the most accurate imaging characteristic, which can improve the diagnostic accuracy of DCE-MRI. However, enhancement observed 5–7 months post-operatively may reflect persistent tissue remodeling secondary to increased vascularity [11,29].
Lehotska et al. evaluated the reliability of DCE-MRI in the detection of post-treatment LR of STSs in 95 patients. Post-contrast images were assessed in patients with diffuse hyperintensity in T2-weighted images (T2WIs) without a discrete mass. DCE-MRI was performed, followed by the subtraction method, and time–intensity curves (TICs) were analyzed. Biopsies were performed on 55 patients, including those with TIC types III, IV, and V (47 patients), and 8 patients with TIC type II. Among the 47 patients with TIC types III, IV, and V, 45 confirmed LR, while 2 demonstrated hypervascular granulation tissue. All eight patients with TIC type curve II were negative for recurrence in histology. DCE-MRI demonstrated a sensitivity of 100%, specificity of 80%, positive predictive value of 95.7%, and negative predictive value of 100%. These results indicate that DCE-MRI can accurately detect LR in patients based on TIC types [7]. DCE-MRI can provide detailed information about tissue characteristics by measuring parameters such as the volume transfer constant (Ktrans), rate constant (Kep), and initial area under the concentration curve (iAUC). Adding these parameters to conventional MRI has been shown to make DCE-MRI more reliable than conventional MRI alone in detecting STS LR [13,30].
This study is limited by sample size due to the rarity of STS and LR, which restricts the power of our analyses. In addition, our a priori decision to exclude very small case series with fewer than 10 patients may have further reduced the number of eligible studies, but was intended to minimize imprecision and potential small-study effects. Further studies comparing different parameters in the same cohorts with consistent results are required for validation and to increase the use of DCE-MRI in evaluating the LR of STS.
5. Conclusions
Conventional MRI has limitations in differentiating LR from post-surgical changes due to overlapping imaging features and technical limitations of the routine sequences. The accuracy of LR detection can be improved by combining conventional MRI with DCE-MRI. In our meta-analysis, adding DCE-MRI parameters to conventional MRI increased the pooled sensitivity and specificity to 98% and 83%, respectively. Among the parameters reported in the included studies, early arterial enhancement, TIC types III–V, higher Ktrans/Kep/iAUC values, and elevated rPF appeared to have the greatest clinical potential for distinguishing LR from expected post-treatment change. Future prospective studies should aim to standardize DCE-MRI acquisition (e.g., contrast administration protocol and temporal resolution) and analysis (e.g., pharmacokinetic modeling, ROI placement, and parameter thresholds) so that these metrics can be harmonized across institutions and translated into reproducible diagnostic criteria for routine clinical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1von Mehren M. Kane J.M. Agulnik M. Bui M.M. Carr-Ascher J. Choy E. Connelly M. Dry S. Ganjoo K.N. Gonzalez R.J. Soft tissue sarcoma, version 2.2022, NCCN clinical practice guidelines in oncology J. Natl. Compr. Cancer Netw.20222081583310.6004/jnccn.2022.003535830886 PMC 10186762 · doi ↗ · pubmed ↗
- 2Meyer M. Seetharam M. First-line therapy for metastatic soft tissue sarcoma Curr. Treat. Options Oncol.201920610.1007/s 11864-019-0606-930675651 · doi ↗ · pubmed ↗
- 3Hall K.S. BrulandØ.S. Bjerkehagen B. Zaikova O. Engellau J. Hagberg O. Hansson L. Hagberg H. Ahlström M. Knobel H. Adjuvant chemotherapy and postoperative radiotherapy in high-risk soft tissue sarcoma patients defined by biological risk factors—A Scandinavian Sarcoma Group study (SSG XX)Eur. J. Cancer 201899788510.1016/j.ejca.2018.05.01129929092 · doi ↗ · pubmed ↗
- 4Nagar S.P. Mytelka D.S. Candrilli S.D. D’Yachkova Y. Lorenzo M. Kasper B. Lopez-Martin J.A. Kaye J.A. Treatment Patterns and Survival among Adult Patients with Advanced Soft Tissue Sarcoma: A Retrospective Medical Record Review in the United Kingdom, Spain, Germany, and France Sarcoma 20182018546705710.1155/2018/546705729977133 PMC 5994280 · doi ↗ · pubmed ↗
- 5Del Grande F. Subhawong T. Weber K. Aro M. Mugera C. Fayad L.M. Detection of soft-tissue sarcoma recurrence: Added value of functional MR imaging techniques at 3.0 T Radiology 201427149951110.1148/radiol.1313084424495264 · doi ↗ · pubmed ↗
- 6Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ 20213727110.1136/bmj.n 71PMC 800592433782057 · doi ↗ · pubmed ↗
- 7Lehotska V. Tothova L. Valkovic L. The role of dynamic contrast-enhanced MRI in differentiation of local recurrence and residual soft-tissue tumor versus post-treatment changes Bratisl. Lek. Listy 2013114889210.4149/BLL_2013_02023331205 · doi ↗ · pubmed ↗
- 8Whiting P.F. Rutjes A.W.S. Westwood M.E. Mallett S. Deeks J.J. Reitsma J.B. Leeflang M.M.G. Sterne J.A.C. Bossuyt P.M.M. QUADAS-2 Group QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies Ann. Intern. Med.201115552953610.7326/0003-4819-155-8-201110180-0000922007046 · doi ↗ · pubmed ↗