Screening and Caring for Older Adults Affected by Sexual or Other Types of Violence: A Pilot Study at Three Belgian Geriatric Departments
Charlotte Boven, Anne Nobels, Nicolas Berg, Nele Van Den Noortgate, Nathalie Courtens, Ines Keygnaert

TL;DR
A new guide helps healthcare providers identify and support older adults who have experienced violence, showing that many are willing to share their experiences when asked.
Contribution
A trauma-informed guide was developed and pilot tested to screen for violence in older adults and improve healthcare provider responses.
Findings
One in five older adults disclosed experiences of violence during the pilot study.
Healthcare providers found the guide acceptable but noted the need for additional training.
Older adults did not find the screening questions intrusive and valued being listened to.
Abstract
What are the main findings? The guide was pilot tested in three geriatric departments with a total of 104 older adults. Older adults are willing to disclose experiences of violence to healthcare providers.A comprehensive trauma-informed guide was developed, including screening questions and referral pathways, to identify all forms of violence experienced by older adults, regardless of when the violence occurredThis guidance supports healthcare providers in engaging in these conversations; however, additional education and training are necessary. The guide was pilot tested in three geriatric departments with a total of 104 older adults. Older adults are willing to disclose experiences of violence to healthcare providers. A comprehensive trauma-informed guide was developed, including screening questions and referral pathways, to identify all forms of violence experienced by older…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
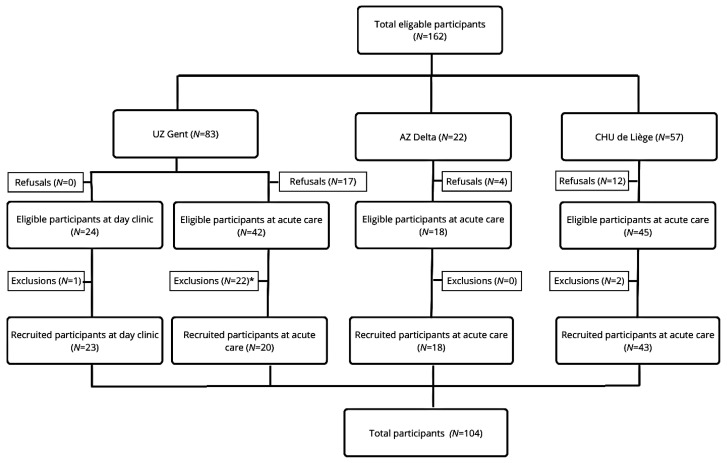 Figure 1
Figure 1 Figure 2
Figure 2- —Belgian Federal Public Service of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElder Abuse and Neglect · Workplace Violence and Bullying · Intimate Partner and Family Violence
1. Introduction
Violence in older adults is a growing public health and human rights concern [1] that affects many individuals worldwide [2,3,4]. Experiences of violence can severely impact older adults’ health, both in the short and long term [5,6], including physical and psychological morbidity [7,8], higher rates of suicidal thoughts [9], and premature mortality [10]. It can occur in the following contexts: homes, care institutions, public spaces, and the Internet [3,4]. Reliable prevalence data remain scarce due to factors such as inconsistent data collection [4,11], varying study methodologies [3], and underreporting [12]. The meta-analysis of Yon, Mikton, and Gassoumis [13] estimated that globally 15.7% of adults aged 60 and older experienced violence in community settings over the past year, but the actual magnitude is likely higher. Studies suggest that only one in 24 cases is reported [12]. As the global population ages, these numbers are expected to increase.
Violence takes various forms: physical, psychological, or sexual violence, material exploitation or financial violence, and neglect [14]. It may occur as a single incident, repeated incidents over a lifetime, or multiple forms simultaneously [15]. Violence in older adults, particularly sexual violence, remains underrecognized in research, policy, and clinical practice [2]. Older adults are often perceived by the public and healthcare providers as unlikely targets of sexual violence [16,17], which contributes to research gaps, a lack of evidence-based interventions, and the exclusion of older adults from policies, guidelines, and prevention programs [2]. Despite common misconceptions, sexual violence in older adults is relatively prevalent. In Belgium, a study found a 44.2% lifetime prevalence and 8.4% prevalence in the past year. Additionally, the recent establishment of Belgian Sexual Assault Care Centres (SACCs) in 2017 underscores the need to educate healthcare providers, as holistic care improves recovery outcomes and reduces the risk of revictimization [18].
The belief that older adults are unlikely victims of violence reflects ageism, which is understood as the stereotyping, discrimination, or holding of prejudices against a person based on their age. Ageism includes attitudes, behaviors, and policies that disadvantage or exclude older adults [19]. A European study found that one in four (24.9%) individuals aged 65 and older reported experiencing ageism [20]. This number is concerning, as ageism contributes to poorer health outcomes among older adults [21] and discourages professional help-seeking as older victims may feel undeserving of care [22,23]. Older adults, particularly those experiencing sexual violence, are often reluctant to disclose to healthcare professionals [17,22,23,24]. As a result, violence often remains unnoticed [3,4] and access to professional care is limited [22]. Previous research [8,25] has shown a clear link between lifetime sexual victimization and mental health issues in old age, and has indicated that older victims of sexual violence experience significant distrust toward others, which may influence how they interact with healthcare workers. Therefore, screening for both recent and non-recent (sexual) violence is an important intervention to improve the care of older victims of (sexual) violence. Healthcare providers are obliged to protect patients from continued harm, but often fail to recognize violence in older patients [26].
To address and prevent violence, clear protocols, adequate staffing and training, and a supportive environment are essential [27]. Most healthcare providers lack training and tools to identify and manage cases of sexual violence [17,28,29] or other forms of violence [30]. The high prevalence of violence, barriers to disclosure, and associated health consequences underscore the urgent need for increased awareness, improved screening, and enhanced care in hospital settings. Because forms of violence often co-occur, a broader screening approach is necessary [31]. Additionally, the potential long-term impact of violence and the increased risk of revictimization [32,33] reinforce the importance of assessing all forms of violence, regardless of when they occurred.
A number of screening tools exist, which cover all types of abuse or a specific form. A review by Gallione, Dal Molin, Cristina [34] shows four comprehensive detection tools: Vulnerability Abuse Screening Scale (VASS), Hwalek-Sengstock Elder Abuse Screening Test (H-S/EAST), Elderly Indicators of Abuse or Indicators of Abuse (E-IOA or IOA), and the Elder Abuse Suspicion Index (EASI). For older adults in Belgium, there is another screening tool available: Risk on Elder Abuse and Mistreatment-Instrument (REAMI or RITI), but this tool only exists in Dutch [11]. Currently, no screening tool specifically addresses sexual violence in older adults. Existing instruments, such as the Elder Abuse Suspicion Index, only tangentially address it. Literature suggests adapting these tools [35] and establishing effective care procedures to improve responses to disclosures [4,11,22].
This paper introduces a new guidance tool that helps healthcare providers identify older adults (without cognitive problems) who have experienced violence and ensure they receive appropriate care after disclosure. The feasibility of the selected population (people of ≥75 years and/or highly care dependent without cognitive problems) and setting (geriatric care), but also the feasibility and acceptability of guidance itself (the screening tool and care and referral pathways) was explored in a pilot, multicentric feasibility study in which a single-group intervention was implemented in three geriatric departments.
2. Materials and Methods
The guidance is part of the larger Operation Alert project, which is commissioned by the Belgian Federal Public Service of Public Health, and implemented by Ghent University Hospital (UZGent), Ghent University (UGent-ICRH/VIORESC), and an NGO on female genital mutilation (GAMS vzw). Operation Alert is a capacity-building project for all staff members in Belgian hospitals, boosting their capacities to detect signals of domestic and sexual violence and to improve their care for victims through e-learning tracks and hands-on care and referral pathways.
The guidance aims to identify older adults who have experienced sexual or other forms of violence (physical, including neglect, psychological, socio-economic, and economic violence), either recently (<one month) or in the past (>one month), in order to provide appropriate care upon positive screening. Definitions of the different types of violence are listed in Appendix A.
The aim of the study was to pilot test the guide, more specifically the screening tool and referral pathways, to assess the feasibility and acceptability of the selected population, setting, and guidance. Its focus was on improving holistic, trauma-sensitive care to older victims of violence, and not on reporting population-based prevalences or factors associated with violence. Prevalences of lifetime sexual violence in older adults are published elsewhere [17].
2.1. Participants
2.1.1. Intervention with Older Adults
Eligible participants were invited to receive the intervention. Participants were Dutch- or French-speaking individuals aged ≥75 or highly care-dependent, with reasonable cognitive functioning, admitted to the geriatric departments of AZ Delta, CHU de Liège, and UZ Gent between 16 December 2024 and 31 March 2025. The hospitals were selected based on their provision of acute geriatric care, their geographical distribution across Belgium, and their integration of a Sexual Assault Care Centre (SACC) where holistic, specialized care is provided to victims of acute sexual violence. Older adults admitted to one of the three participating geriatric departments were screened using the guidance, having first provided written informed consent. Patients were excluded if their health condition was too severe for study participation, worsened between informed consent and screening, or if cognitive issues (e.g., delirium) were noticed before or during the screening.
The age threshold of 75 years old or above and the level of care dependency align with the admission criteria for Belgian geriatric departments. Admissions include both acute care units, where patients stay for multiple days, and day clinics, where patients receive diagnoses (e.g., cognitive impairment) or treatments (e.g., intravenous therapy) within a single day. It is important that screening is conducted in professional care settings, such as hospitals, since older adults generally use healthcare services more often. The geriatric department was considered an ideal setting due to its multidisciplinary team meetings and comprehensive geriatric assessments. While other settings, such as residential care, may provide more time to build trusting relationships and facilitate such conversations, it is important to screen for violence in all care settings. Older adults who experience violence from a caregiver in one care setting may feel safer disclosing it in a different care environment where they are not dependent on the perpetrator.
2.1.2. Evaluation with Healthcare Providers
Participants were Dutch- or French-speaking healthcare providers working in the geriatric departments or Sexual Assault Referral Centers (SARC) of AZ Delta, CHU de Liège, and UZ Gent. We selected a variety of professional profiles to illustrate that the guide can be used across different roles. Because it is intended to be accessible to all healthcare providers working with older adults, we also wanted to assess whether involving different profiles was both feasible and acceptable. The healthcare providers in this study were a convenience sample of different profiles from participating settings. After having followed training, they implemented the guidance between 16 December 2024, and 31 March 2025. Healthcare providers, who carried out the screening, gave written consent and subsequently completed an evaluation on the guidance.
2.2. Study Materials
As mentioned in the background, several screening tools exist. However, the VASS and RITI are designed for use in home care, whereas the HS-EAST, EASI, and E-IO can be applied in a hospital setting. The IOA and E-IOA require a lengthy completion time of two to three hours, which may be burdensome for older adults with (acute) health problems admitted to the hospital. In contrast, the EASI can be administered in approximately two minutes [11]. However, it lacks behavior-specific questions (BSQ) related to sexual violence, which is an important limitation when working with older adults whose generational beliefs (e.g., about marital rape) may influence how they understand and report sexual violence. The BSQ uses specific, concrete descriptions to frame incidents, rather than broad labels such as ‘rape’, thereby limiting ambiguity in interpretation. Participants who may not recognize their own experiences of sexual victimization or link the questions to their own experiences may not disclose their experiences of lifetime sexual violence [36]. The BSQs were based on a previous study (UN-MENAMAIS) on sexual violence in older adults [28], and aligned with the WHO definition of sexual violence, which includes various forms of sexual violence, such as sexual harassment without physical contact, sexual abuse involving physical contact without penetration, and (attempted) rape. Another motivation for developing the guide was that the aforementioned screening tools rely solely on dichotomous questions, whereas we aimed to include open questions as well. Findings from our focus groups and expert consultations highlighted the need for such open questions, as they help create a safe and compassionate environment that allows space for patients to share their lifetime experiences of violence and talk about their network and underlying dynamics.
The development of the guidance was performed through an iterative process of literature reviews, input from national and international experts, and focus group discussions before piloting was conducted. Detailed information on the research process and results is available in Appendix B. The guidance encompasses three core components: a screening protocol, care and referral pathways, and a theoretical foundation on sexual violence. All study materials are available in both French and Dutch, in accordance with Belgium’s bilingual context.
2.2.1. Intervention with Older Adults
In addition to reviewing the guidance, healthcare providers completed a self-paced, evidence-based e-learning module developed for Operation Alert focused on the experiences of violence among older adults. SARC healthcare providers have extensive experience in talking about violence, and have followed the e-learning to learn more about violence in older adults. Those from the geriatric department have extensive experience in talking with older adults, and followed the e-learning to broaden their competencies on violence in older adults. Accessible between December 2024 and March 2025, the 45–60-min module addressed the dynamics of violence, including risk and protective factors, warning signs, and intervention strategies. It also supported professionals in initiating conversations about (suspected) violence with older adults, colleagues, and potentially abusive caregivers, while offering guidance on delivering holistic care to all involved.
The screening tool (see Appendix C) was integrated into routine geriatric assessments. Patients were informed through consent procedures that participation was voluntary, and they could decline or stop at any time. Screenings were conducted privately, without relatives present, in one or two phases by professionals from various backgrounds.
Providers had flexibility in administering the tool, including adapting the phrasing or sequence of questions. However, any modifications to the screening protocol or care pathways had to be documented in a brief interim questionnaire. This form also included sections for feedback on patient reactions and any issues with implementation, such as unclear items or missing referral contacts. If no changes or issues were observed, completion of the interim questionnaire was not required.
2.2.2. Evaluation with Healthcare Providers
The feasibility and acceptability of the newly developed guidance [37] were evaluated by healthcare providers using an online questionnaire (Qualtrics) based on the theoretical framework of acceptability by Sekhon, Cartwright, and Francis [38], which assesses seven constructs: affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness, and self-efficacy. Healthcare providers rated each construct on a five-point Likert scale with different response options. In addition to these closed-ended items, the questionnaire included open-ended questions, allowing healthcare providers to provide feedback on feasibility (e.g., required resources, implementation barriers, and suggestions for improvement). Older adults did not directly evaluate the feasibility or acceptability of the guidance, as relevant items were discreetly embedded in routine care (e.g., the geriatric assessment), making it difficult for patients to distinguish between the intervention and standard practice. Moreover, we wanted to limit the administrative burden associated with hospital admission, because some patients might not be able to complete the evaluation independently. They would need help from (potentially) abusive caregivers or from the researcher, which in the latter case could bias the results.
2.3. Ethics
The research protocol was approved by the Ethics Committee of Ghent University Hospital [ONZ-2024-0077]. Healthcare providers and older adults received verbal and written information about the study and gave their explicit and written consent to participate. The study was also registered in a publicly accessible database [NCT06780540] of the National Library of Medicine (NIH) and released on 13 January 2025.
The study was conducted in accordance with the WHO’s ethical and safety recommendations for conducting research on sexual violence. Participants received detailed information about the study in advance. Informed consent was obtained prior to participation, and participants could withdraw their consent at any time. They could also always pause or stop the conversation at any time. They were also informed that their participation or non-participation would not affect the care they received. Participating healthcare providers ensured that the screening was conducted in a safe, nonjudgmental environment, without other patients, relatives, or healthcare providers present. After the conversation, older adults were asked whether they wanted to receive any further support, and what type if they did. Informed consent also included contact information for both the geriatric department and the research team. The guide also included referral pathways depending on the nature and acuteness of the violence. The steps outlined for acute or non-acute violence were in accordance with Article 458 of the Belgian Criminal Code, and the flowchart was extensively reviewed by research and clinical experts in this field.
3. Results
3.1. Intervention with Older Adults (n = 104)
A total of 104 eligible participants were recruited from three different sites: CHU de Liège (n = 43), UZ Gent (n = 43), and AZ Delta (n = 18). Several patients refused to participate (n = 33) and/or were excluded from participation (n = 25). Some patients declined participation due to disinterest, ongoing treatments, providing only oral informed consent, but refusing to sign the paperwork, and some patients felt too ill or in too much pain to participate. A study flowchart with more information about the recruitment of participants on the different sites can be found in Figure 1.
Each hospital site faced specific challenges that complicated the recruitment process, including viral outbreaks, competing care priorities, and staff shortages or overburdened healthcare teams. Due to staffing constraints, the screening at AZ Delta was carried out by healthcare providers (nurses and psychologists) from the Sexual Assault Care Centre rather than the geriatric department. However, these healthcare providers took deliberate steps to build trust with patients before administering the screening questions.
Of the 104 participants included in the study, the majority were women (n = 62). Additionally, 45 participants lived with their partner. The mean age of the participants was 83 years [range: 75–102 years]. More information on the patients’ characteristics can be found in Table 1.
One in five participants (20.2%) disclosed experiences of violence, either recent or throughout their lives. The types of violence reported included economic violence (n = 7), of which six were burglaries, psychological violence (n = 6), sexual violence (n = 3), physical violence (n = 2), neglect (n = 2), and socio-economic violence (n = 1). A higher number of disclosures were reported by women (n = 13) than by men (n = 8), with this difference nearing statistical significance (Fisher’s Exact Test, p = 0.05).
3.2. Evaluation with Healthcare Providers (n = 12)
Twelve healthcare providers who implemented the screening with older adults at CHU de Liège, UZ Gent, and AZ Delta completed a questionnaire at the end of the intervention period. The questionnaire included both open- and closed-ended items rated on a five-point Likert scale (see Appendix D), and results indicated an overall positive evaluation of the guidance. Further details on the healthcare providers’ characteristics and their evaluation are presented in Table 2.
Responses to the closed-ended questions (see Table 2) highlighted several key strengths, such as its perceived positive contribution to the patient’s well-being, the patient’s acceptability of the screening protocol, healthcare providers’ confidence in using the protocol, and their recommendations for its use by others.
The open-ended questions revealed that healthcare providers believed it is important for the screening to be integrated into existing standards of care to avoid increasing their workload. They also emphasized that the guidance can raise awareness among healthcare providers, enhance their vigilance, and make conversations about violence more common. At the same time, they stated that implementing this approach will require a shared vision and regular ethical reflections within a team. The systematic incorporation of screening into routine practice, coupled with the initiative of healthcare providers, may increase the likelihood of disclosure by reducing barriers to reporting. Healthcare providers noted that the guidance helps patients to feel seen and heard; hence, their experiences of violence and the impact it has on them are acknowledged. They reported that patients responded very positively to the conversation and appreciated that healthcare providers took the time to listen to them. Older adults did not find the questions to be intrusive, but experienced them as ordinary. Disclosures provided the opportunity to offer tailored care, if desired by the older adult, which was often not the case. According to the healthcare providers, it was often sufficient for patients to be offered a sympathetic ear, rather than a formal intervention, emphasizing the need to refrain from falling into the trap of problem-solving.
The evaluation of the guidance also identified several areas for improvement. First, the phrasing of the screening questions needs to be adjusted to make them easier to understand. Additionally, there is a need for examples to clarify what constitutes different types of violence. Second, it was emphasized that the guidance should support more natural conversations with patients, rather than relying on a rigid screening protocol. Third, in addition to the screening protocol, further training and education are needed to help healthcare providers develop conversational skills that will enable them to engage with patients (e.g., trauma-sensitive care and adequate follow-up questions) and abusive caregivers (e.g., psycho education), but also adequately respond to disclosures of violence.
4. Discussion
Although several screening tools exist for detecting and supporting older adults affected by violence, there has been limited focus on sexual violence and non-recent experiences. This study led to the development of a comprehensive guidance designed to identify all forms of violence experienced by older adults, including sexual violence, regardless of when the violence occurred. The guidance is informed by trauma-informed care principles, which are crucial given the high likelihood of cumulative trauma in older populations, minimizing the risk of re-traumatization. The aim of the pilot study was to explore whether the guidance can be practically implemented on a larger scale within this specific setting (geriatric care) and population (people of ≥75 years and/or highly care dependent). The feedback from healthcare providers demonstrated its feasibility and acceptability among healthcare providers working in acute geriatric care settings. It was indicated that the guidance has the potential to enhance the identification and disclosure of sexual and other types of violence, ultimately facilitating timely and appropriate care. Healthcare providers also encountered challenges while screening, such as patients’ medical conditions (e.g., severe illness), early discharge, significant cognitive impairments, and temporary confusion (e.g., delirium).
A key strength of this study is the inclusion of a geriatric population with a mean age of 83 years, a demographic frequently underrepresented in research on violence. Whereas prior studies [39] have predominantly focused on younger, more active individuals aged 65 and older, this study specifically includes older adults characterized by higher levels of frailty and comorbidity. This inclusion enhances the clinical relevance of the findings and demonstrates that the guidance is applicable within a geriatric population, where advanced age and multimorbidity are common. Although the guidance proved feasible for cognitively intact older adults in an acute geriatric ward, its generalizability to other healthcare settings, such as different hospital departments, psychiatric units, primary care, or long-term residential facilities, remains to be established. Each setting presents distinct challenges related to patient profiles and healthcare provider roles, which can impact both implementation and effectiveness. A limitation of our study is the small sample size of the healthcare providers who conducted the screening and subsequently completed the questionnaire, which may have introduced bias. It is possible that the professional background (e.g., nurse versus psychologist) and level of experience in communicating with older adults may have influenced our findings.
Participants in our study underscored the importance of integrating screening protocols within existing care frameworks, notably the comprehensive geriatric assessment. However, such integrative assessments are not universally conducted across all healthcare environments, which may limit the guidance’s applicability. Moreover, cognitive impairment is prevalent in geriatric populations, yet current guidelines are primarily designed for those with sufficient cognitive capacity to engage in screening processes. Future research should investigate violence prevalence and characteristics among cognitively impaired individuals, including those with dementia, a known risk factor for victimization [40]. Further evaluation of the guidance through rigorous methodologies, such as cluster randomized controlled trials, is also warranted to assess its effectiveness compared to standard care. In this design, clusters begin in the control condition and are randomly assigned to sequences. They then cross over to the intervention condition at a predetermined time point until all clusters have received the intervention [41]. Overall, while this study focused on feasibility, acceptability, and identifying limitations, subsequent research should aim to confirm the guidance’s impact on initiating adequate support and ultimately reducing long-term mental health consequences for older adults affected by violence. It is also important to note that we encourage to gain input from older victims of violence. This will help to further reflect and substantiate the guide, as it is a living document that will need to be regularly updated in time (e.g., referral pathways to organizations and medical care, …).
In our study, one in five older adults disclosed having experienced violence, though the true prevalence is likely higher [12]. Social context significantly influences whether individuals choose to disclose such experiences or seek help [42]. Healthcare providers reported that older adults generally did not mind being asked about potential violence, highlighting the importance of creating a safe, supportive, and nonjudgmental environment to encourage disclosure [16,43,44]. Building trust, rapport, and practicing active listening are essential to facilitate openness [45]. However, research indicates that disclosure of sexual violence alone does not necessarily improve mental health outcomes. Instead, the response to disclosure plays a critical role [46]. Negative reactions, such as controlling behavior, dismissal, or differential treatment, are linked to worse psychological outcomes [47]. These findings emphasize the urgent need for training of healthcare providers aimed at reducing harmful social responses. Healthcare providers also noted that, in most cases, older adults simply wanted someone who listened to their story in a compassionate way. Many older adults do not always identify themselves as victims of sexual or other types of violence due to factors such as internalized ageism or a desire to protect family ties [16,23]. They may downplay their experiences by attributing behaviors to caregiver stress [43] or describing sexual violence as “just something that happened” [46]. Consequently, rigid screening protocols may be inadequate, as older adults might not recognize or label their experiences as violent. In these situations, healthcare providers can play a crucial role in helping older adults recognize their experiences as violent, which is an essential first step towards help-seeking behaviors [48]. The feedback from the pilot study informed the development of a broader and more flexible screening protocol (see Appendix E), designed to create space for older adults to speak freely. Individuals may be reluctant to disclose experiences of violence during initial screening, as they may need time and space to decide, and future research could explore whether readmitted patients might report such experiences at a later stage by implementing the guide for a longer period of time.
Finally, healthcare providers highlighted the critical need for comprehensive training and education to develop competencies necessary to address sexual and other forms of violence in older adults. Previous research shows that many healthcare professionals lack competencies in this area, largely due to limited educational opportunities [30,49]. Our findings, along with previous research, reinforce the urgency to invest in specialized training programs, which have been shown to enhance knowledge, increase the use of assessment tools, reduce reports of abusive actions by staff [50], and effectively reduce ageism [19]. Every healthcare provider working with potential victims of violence in hospital settings should be able to recognize signs of violence and provide basic support. In addition to the basic competences, we recommend that those who conduct the screening should also possess more advanced skills and knowledge (e.g., recognize ageist attitudes, understand cumulative trauma, navigate referral pathways). Therefore, the guide includes references to relevant international literature and e-learning modules that were specifically developed, as well as this guide, as part of a larger governmentally funded project called “Operatie Alert” (Operation Alert).
Additionally, healthcare providers emphasized the importance of collective responsibility and ongoing critical reflection within healthcare teams. Routine screening for violence can have a psychological impact on healthcare providers, as repeated exposure to traumatic accounts or direct encounters with violence may result in vicarious trauma, especially among those with personal histories related to the patients they treat [49]. Research estimates that between 40% and 85% of healthcare providers may experience vicarious trauma, compassion fatigue, or heightened trauma-related symptoms due to prolonged engagement with traumatized populations [51]. Therefore, it is equally important to incorporate guidance on managing vicarious trauma and promoting self-care in training programs.
5. Conclusions
The guidance developed for screening both recent and non-recent experiences of sexual and other forms of violence was found to be feasible and acceptable within a geriatric care setting. However, it is important to acknowledge that the pilot study included only a specific subset of the population, as individuals with major cognitive impairments and those who were too ill to participate were excluded. Additionally, healthcare providers reported that patients responded positively to the screening questions and did not find them intrusive. We recommend that future research conduct feasibility studies in other care contexts, such as additional hospital departments or primary care settings, and interventional studies with clear health-related outcome measures. Finally, we believe it would be valuable to gain direct input from older victims of violence to further reflect and substantiate the guide, as it is a living document that will need to be regularly updated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Choi M. Brownell P. Moldovan S. International movement to promote human rights of older women with a focus on violence and abuse against older women Int. Soc. Work.20156017018110.1177/0020872814559562 · doi ↗
- 2Bows H. Sexual Violence Against Older People: A Review of the Empirical Literature Trauma Violence Abus.20181956758310.1177/152483801668345529333969 · doi ↗ · pubmed ↗
- 3Hirst S.P. Majowski K. Elder Abuse: A Global Challenge and Canada’s Response J. Gerontol. Nurs.202248212510.3928/00989134-20220307-0135343841 · doi ↗ · pubmed ↗
- 4United Nations Violence and Abuse Against Older Persons Available online: https://www.ohchr.org/en/special-procedures/ie-older-persons/violence-and-abuse-against-older-persons#:~:text=Violence%20against%20older%20persons%20is,%2C%20cyberspace%2C%20and%20emergency%20settings(accessed on 18 March 2025)
- 5Mouton C.P. Rodabough R.J. Rovi S.L. Brzyski R.G. Katerndahl D.A. Psychosocial effects of physical and verbal abuse in postmenopausal women Ann. Fam. Med.2010820621310.1370/afm.109520458103 PMC 2866717 · doi ↗ · pubmed ↗
- 6Schofield M.J. Powers J.R. Loxton D. Mortality and disability outcomes of self-reported elder abuse: A 12-year prospective investigation J. Am. Geriatr. Soc.20136167968510.1111/jgs.1221223590291 · doi ↗ · pubmed ↗
- 7Rapsey C.M. Scott K.M. Patterson T. Childhood sexual abuse, poly-victimization and internalizing disorders across adulthood and older age: Findings from a 25-year longitudinal study J. Affect. Disord.201924417117910.1016/j.jad.2018.10.09530342377 · doi ↗ · pubmed ↗
- 8Nobels A. Lemmens G. Thibau L. Beaulieu M. Vandeviver C. Keygnaert I. “Time Does Not Heal All Wounds”: Sexual Victimisation Is Associated with Depression, Anxiety, and PTSD in Old Age Int. J. Environ. Res. Public Health 202219280310.3390/ijerph 1905280335270496 PMC 8910002 · doi ↗ · pubmed ↗