Prediction of Treatment Response by Thyroid Bed Uptake on Post-Ablative Whole-Body Scan in Intermediate-Risk Patients with Papillary Thyroid Cancer
Eunkyoung Choi, Yong-An Chung, Soo Jin Kwon, Jinkyoung Oh

TL;DR
This study shows that higher thyroid bed uptake on scans after radioactive iodine therapy is linked to worse treatment outcomes in intermediate-risk papillary thyroid cancer patients.
Contribution
The study identifies thyroid bed uptake on post-ablative scans as an independent predictor of treatment response in intermediate-risk papillary thyroid cancer patients.
Findings
14.9% of patients had non-excellent treatment responses, associated with higher thyroid bed uptake.
Higher thyroid bed uptake was an independent negative prognostic factor for achieving an excellent response.
Stimulated thyroglobulin levels also predicted treatment response.
Abstract
Background/Objectives: This study aimed to evaluate the prognostic significance of thyroid bed uptake on post-ablative whole-body scan (PAWBS) in predicting treatment response in intermediate-risk papillary thyroid carcinoma (PTC) patients undergoing high-dose radioactive iodine (RAI) therapy following total thyroidectomy. Methods: This retrospective study included 148 intermediate-risk PTC patients who underwent high-dose RAI therapy after total thyroidectomy. PAWBS was performed 7 days post-therapy, and thyroid bed uptake was visually graded. Treatment response was assessed using stimulated thyroglobulin (sTg) levels, imaging studies, and clinical follow-up. Responses were classified into excellent, indeterminate, biochemical incomplete, or structural incomplete categories. Logistic regression analyses were conducted to identify predictors of treatment response. Results: Among the 148…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
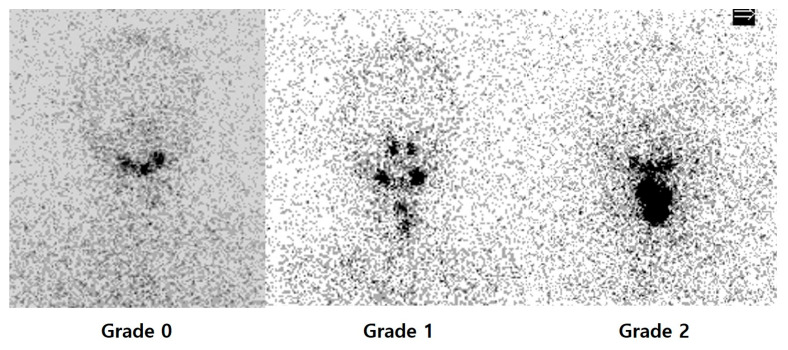 Figure 1
Figure 1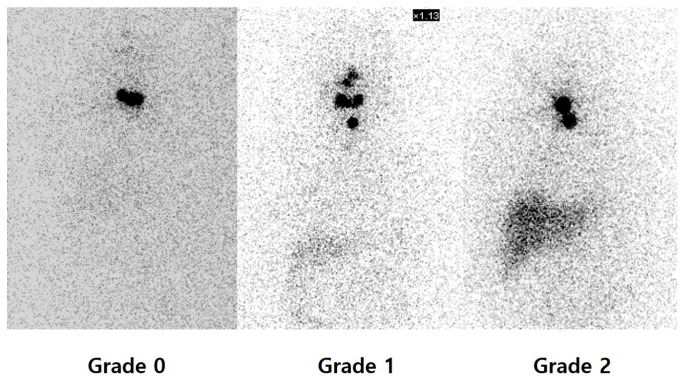 Figure 2
Figure 2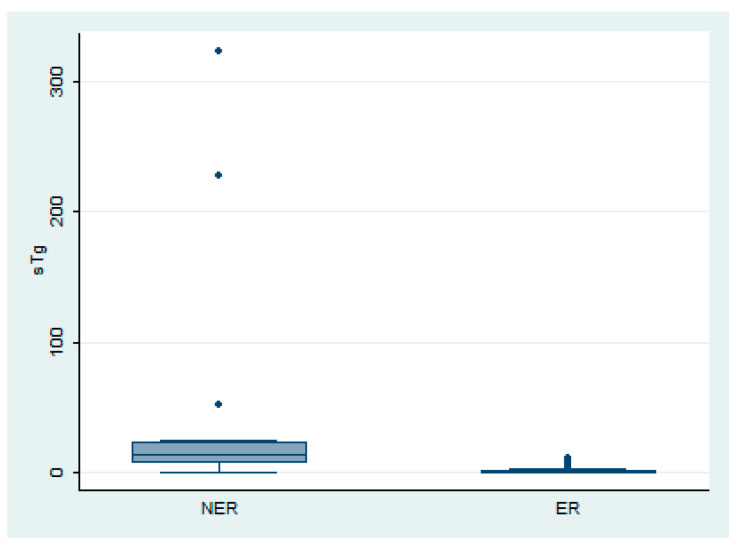 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid and Parathyroid Surgery · Thyroid Disorders and Treatments
1. Introduction
Thyroid cancer is one of the most common malignancies, with a rising incidence over recent decades. Papillary thyroid carcinoma (PTC) accounts for the majority of thyroid cancer and has a very favorable prognosis, with a 10-year survival rate of 85–93% [1]. Radioactive iodine (RAI) therapy is a standard treatment for PTC patients following total thyroidectomy, aimed at ablation of residual thyroid tissue and treatment of known or presumed residual or metastatic disease [2].
According to the 2015 American Thyroid Association (ATA) risk of recurrence stratification, thyroid cancer patients are categorized into low, intermediate, and high-risk groups [2,3]. High-risk thyroid cancer patients require higher doses of RAI therapy and additional treatments to improve outcomes, especially for those with distant metastasis. In contrast, low-risk patients have a low likelihood of recurrence and therefore are managed primarily with appropriate follow-up strategies, avoiding unnecessary treatments. However, managing intermediate-risk PTC patients remains challenging, as their clinical outcomes vary widely and require individualized treatment strategies to optimize prognosis.
Post-ablative whole-body scan (PAWBS) is recommended to be performed 5–10 days after RAI therapy. It plays a role in identifying lesions not detected prior to treatment and offers significant prognostic information related to treatment outcomes [4,5,6]. Although there have been reports suggesting that thyroid bed uptake in PAWBS is associated with prognosis, research in this area is still limited [5,6,7]. Furthermore, there was no information in the literature focusing on response evaluation in intermediate-risk PTC patients. Given the heterogeneity of this risk group and the need for individualized treatment approaches, assessing the prognostic significance of thyroid bed uptake on PAWBS may aid in optimizing patient management. The aim of this study was, therefore, to predict treatment response by evaluating thyroid bed uptake on PAWBS in intermediate-risk PTC patients who underwent high-dose RAI therapy after total thyroidectomy.
2. Materials and Methods
This study was approved by the institutional review board in the hospital. The requirement for written informed consent was waived due to the retrospective nature of the study and the use of anonymized data. We conducted a retrospective review of the medical records of PTC patients who underwent total thyroidectomy at our facility from January 2017 through December 2021. Clinicopathological data were obtained through an electronic medical record review, and the patients were classified as low, intermediate, or high risk using the 2015 ATA risk of recurrence stratification system [2]. Patients were included if they were classified as intermediate risk and had received high-dose RAI therapy after total thyroidectomy. Patients were excluded from the study based on the following criteria: (1) previous RAI therapy (low or high dose); (2) diagnosis of distant metastasis prior to receiving RAI therapy; (3) high antithyroglobulin antibody (TgAb) at the time of ablation; (4) presence of any significant liver disease; and (5) absence of available follow-up data. Pathological characteristics were evaluated in the surgical specimens obtained from the total thyroidectomy by an experienced pathologist: primary tumor size, presence of extrathyroid extension, multifocality, extranodal spread, and lymph node metastasis.
Treatment strategies were individualized based on a multi-disciplinary discussion with clinicians and nuclear medicine physicians, taking into account the clinical risk stratification for thyroid cancer. All patients received levothyroxine orally following total thyroidectomy. After withdrawal of thyroid hormone or injection of recombinant human thyroid-stimulating hormone (rh-TSH), the patients were given RAI therapy with doses ranging from 3.7 GBq to 5.55 GBq. Considering the higher iodine intake in South Korea compared with other countries, the patients were kept on a low-iodine diet for 2–3 weeks prior to I-131 ablation. For patients who received RAI therapy after thyroid hormone withdrawal, stimulated Tg (sTg) was measured in the third week of hormone withdrawal. For those who received I-131 treatment after injection of rh-TSH, sTg was measured on the third day (D3) following rh-TSH injection.
PAWBS is performed 7 days following RAI therapy using a dual-head gamma camera equipped with high-energy collimators. The main parameter assessed was the uptake in the thyroid bed with visual analysis into 3 grades according to the following semi-quantitative system, depending on intensity: grade 0 = no uptake; grade 1 = mild; grade 2 = moderate to intense, as independently rated by two nuclear medicine physicians (Figure 1) [5,6]. Image interpretation was independently performed by two board-certified nuclear medicine physicians (J.O. and E.C.), who were blinded to the patients’ clinical information, except for body weight, which was considered due to its potential impact on photon attenuation. Discrepancies between readers were resolved by consensus. Discrepancies between readers were resolved by consensus. In cases where uptake patterns appeared atypical—such as uptake outside the thyroid bed or linear midline uptake—additional imaging (e.g., neck ultrasonography or CT) was reviewed, and final interpretation was made by consensus. In addition, diffuse liver uptake was scored by visual assessment into 3 grades in the same way (Figure 2).
Therapy response was evaluated using sTg levels, neck ultrasound findings performed by an experienced radiologist, radioiodine scans, and any additional imaging conducted during the follow-up period, which ranged from 6 to 12 months. According to the 2015 ATA guidelines, therapy responses were classified as follows: (1) excellent response: negative imaging and either suppressed Tg < 0.2 ng/mL or TSH-stimulated Tg < 1 ng/mL; (2) indeterminate response: non-specific findings on imaging studies or suppressed Tg that is detectable but <1 ng/mL or stimulated Tg between 1 and 10 ng/mL; (3) biochemical incomplete response: negative imaging and suppressed Tg ≥ 1 ng/mL or stimulated Tg ≥ 10 ng/mL or increased TgAb values; (4) structural incomplete response: structural or functional evidence of disease with any Tg level. The response to RAI therapy was categorized into excellent response (ER) and non-excellent response (NER), which includes indeterminate response, biochemical incomplete response, and structural incomplete response. We analyzed the correlation between the intensities of thyroid bed and liver uptake on PAWBS and these response categories.
Statistical analyses were performed using Stata software (version 13.0; StataCorp, College Station, TX, USA). The normality of distribution for continuous variables was assessed using the Kolmogorov–Smirnov test. Parametric variables were expressed as mean ± standard deviation, whereas non-parametric variables were presented as median with range. Categorical variables are presented as frequencies with percentages. For comparisons between groups, the chi-square test or Fisher’s exact test was used for categorical variables. Continuous variables were analyzed using Student’s t-test for parametric data and the Mann–Whitney U test for non-parametric data. The correlation between variables was evaluated by Spearman’s rank correlation. Variables identified as significantly affecting treatment response in univariate analyses were entered into a multivariate logistic regression model to determine the independent predictors of remission. p-values < 0.05 were considered statistically significant.
3. Results
3.1. Patient Characteristics
A total of 148 patients were included in this study. Of these, 35 (23.5%) were men and 113 (76.5%) were women. The mean age at diagnosis was 46 years (range, 20–84 years). Based on the treatment response, 126 patients (85.1%) were classified as ER, and 22 (14.9%) as NER. Among the 22 NER patients, 18 had a biochemical incomplete response, and 4 had an indeterminate response. Detailed clinical and pathological characteristics at the time of RAI therapy are summarized in Table 1.
3.2. Relationship Between Uptake on PAWBS and Therapy Response
Thyroid bed uptake on PAWBS showed a significant association with treatment response. Among the 148 patients, 10 (6.8%) showed grade 0 intensity, 86 (58.1%) showed grade 1, and 52 (35.1%) showed grade 2 intensity. In the ER group, 10 patients had grade 0, 80 had grade 1, and 36 had grade 2 intensity. In contrast, in the NER group, none had grade 0, 6 had grade 1, and 16 had grade 2 intensity. The distribution of thyroid bed uptake differed significantly between ER and NER groups (p = 0.001, Table 1). Liver uptake on PAWBS did not show a significant association with treatment response. Five patients (3.4%) showed grade 0 intensity, 43 (29.1%) had grade 1, and 100 (67.6%) had grade 2. In the ER group, 4 had grade 0, 38 had grade 1, and 84 had grade 2 intensity. In the NER group, 1 had grade 0, 5 had grade 1, and 16 had grade 2 intensity. The difference between the groups was not statistically significant (p = 0.755, Table 1).
3.3. Relationship Between sTg and Thyroid Bed Uptake on PAWBS
The mean sTg level among all patients was 6.61 ng/mL. In the ER group, the mean sTg was significantly lower at 1.69 ng/mL (range, 0.01–37.51), compared to 36.88 ng/mL (range, 0.1–323.2) in the NER group (p < 0.001, Mann–Whitney U test, Figure 3). A positive correlation was observed between sTg levels and the intensity of thyroid bed uptake on PAWBS (Spearman r = 0.298, p < 0.001), suggesting that higher sTg levels are associated with stronger uptake on PAWBS.
3.4. Uni- and Multivariate Analyses
Univariate logistic regression analysis revealed that the intensity of thyroid bed uptake on PAWBS, sTg, lateral lymph node metastasis, and extranodal spread were significantly associated with therapy response (p < 0.001, p < 0.001, p = 0.049, and p = 0.005, respectively).
In the multivariate logistic regression analysis, thyroid bed uptake intensity and sTg remained significant independent predictors of therapy response (both p < 0.001, Table 2).
Other clinicopathological features, including primary tumor size, extrathyroidal extension, multifocality, extranodal spread, central lymph node metastasis, and lateral lymph node metastasis, showed no significant association with treatment response.
4. Discussion
This study demonstrated that the intensity of thyroid bed uptake on PAWBS and sTg level are significant predictors of treatment response in intermediate-risk PTC patients. These findings highlight the role of meticulous post-therapy evaluation, suggesting that patients exhibiting higher thyroid bed uptake on PAWBS and pre-RAI sTg level may benefit from closer surveillance and additional therapeutic interventions. The National Comprehensive Cancer Network (NCCN) guidelines advocate for the use of PAWBS following RAI therapy, emphasizing its utility in detecting previously unrecognized lesions and differentiating between iodine-avid and non-avid disease [8]. Expanding upon this established diagnostic utility, our findings propose that PAWBS also provides valuable prognostic information regarding therapy response, particularly within intermediate-risk patients.
Although previous studies have reported that intense thyroid bed uptake on PAWBS may serve as an independent predictor of treatment outcomes, the majority of these investigations have not specifically targeted intermediate-risk patients—a subgroup that constitutes a substantial proportion of PTC cases [5,6,9]. A significant challenge in managing this subgroup is the wide heterogeneity of clinical outcomes observed in intermediate-risk patients. This subgroup, which constitutes a substantial portion of PTC patients, requires individualized treatment and surveillance plans to optimize prognosis [10,11]. To the best of our knowledge, the present study is the first to systematically assess the prognostic significance of thyroid bed uptake intensity on PAWBS exclusively in intermediate-risk PTC patients. The degree of thyroid bed uptake may reflect the burden of remnant tumor or residual thyroid tissue, both of which have been identified as factors associated with unsuccessful outcomes following adjuvant therapy [6,12]. This was further supported by our analysis demonstrating a significant association between thyroid bed uptake intensity and sTg level.
sTg serves as a surrogate marker for the burden of remnant thyroid tissue, which is closely associated with treatment response [13]. A low sTg level at the time of remnant ablation may indicate a favorable prognosis. Similarly, thyroid bed uptake observed on PAWBS may indirectly reflect sTg levels and, therefore, function as a predictor of therapeutic outcomes. Integrating sTg with thyroid bed uptake findings on PAWBS may improve the accuracy of treatment response prediction and support more individualized therapeutic strategies for intermediate-risk PTC patients.
In this study, univariate analysis revealed that among various clinicopathological parameters, lateral lymph node metastasis and extranodal spread were significantly associated with a non-excellent treatment response. Extranodal spread, the extension of tumor cells beyond the lymph node capsule into surrounding tissue, is associated with a significantly higher risk of recurrence and compromised disease-specific survival [14,15]. This underscores the importance of a thorough pathological review of surgical specimens, as the presence of extranodal spread can have a profound impact on a patient’s long-term prognosis. Similarly, lateral lymph node metastasis has been repeatedly linked to unfavorable therapeutic outcomes and higher rates of locoregional recurrence or distant metastasis, supporting its role as a key prognostic marker in PTC [16,17].
Kim et al. demonstrated that both thyroid bed uptake and liver uptake on PAWBS were significant prognostic factors for treatment response in differentiated thyroid cancer patients [6]. A notable discrepancy in our study’s findings is the lack of a significant correlation between liver uptake on PAWBS and treatment response, contrasting with a previous study by Kim et al. This contrast may be attributed to differences in the patient populations included in each study. Kim et al. included advanced thyroid cancer patients with substantial residual thyroid tissue or metastatic disease, whereas our study excluded patients with overt thyroid cancer tissue or distant metastases prior to RAI therapy. Regarding the prognostic implications of liver uptake, previous research has suggested that diffuse hepatic visualization on PAWBS may reflect the degree of thyroid tissue destruction or the presence of functioning metastases [5,18]. It has been proposed that tissue binding of I-131-labeled iodoproteins contributes to diffuse hepatic uptake on PAWBS. Although liver uptake has been associated with poorer treatment responses in certain contexts, our findings suggest that, in intermediate-risk PTC patients without significant residual disease, liver uptake intensity may not serve as a reliable predictor of treatment response.
There are several limitations in this study. First, because of the retrospective nature of the study design, selection bias may have been introduced. A larger, multicenter cohort would strengthen the validity and applicability of the results across diverse populations and clinical settings, and allow for a more robust evaluation of recurrence and survival outcomes with longer follow-up. Second, the visual grading of thyroid bed uptake was performed on planar scans, which inherently lack the anatomical resolution and quantitative capability of hybrid imaging modalities such as single-photon emission computed tomography/computed tomography (SPECT/CT). Future studies employing quantitative SPECT/CT analysis could enhance the objectivity and reproducibility of thyroid bed uptake evaluation. Third, patient classification and treatment response categories were based on the 2015 ATA guidelines [2]. Future studies applying the 2025 criteria will be needed to ensure consistency with current clinical practice [19].
In conclusion, thyroid bed uptake on post-ablative whole-body scan is an independent negative predictor of treatment response in intermediate-risk PTC patients. Along with elevated sTg levels, increased thyroid bed uptake may reflect the extent of remnant tumor or residual thyroid tissue and help identify patients who require closer surveillance and tailored management following high-dose RAI therapy. These findings support incorporating post-therapy scan findings into treatment planning and follow-up strategies to improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hundahl S.A. Fleming I.D. Fremgen A.M. Menck H.R. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985–1995 Cancer 1998832638264810.1002/(SICI)1097-0142(19981215)83:12<2638::AID-CNCR 31>3.0.CO;2-19874472 · doi ↗ · pubmed ↗
- 2Haugen B.R. Alexander E.K. Bible K.C. Doherty G.M. Mandel S.J. Nikiforov Y.E. Pacini F. Randolph G.W. Sawka A.M. Schlumberger M. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer Thyroid 201626113310.1089/thy.2015.002026462967 PMC 4739132 · doi ↗ · pubmed ↗
- 3Luster M. Clarke S.E. Dietlein M. Lassmann M. Lind P. Oyen W.J. Tennvall J. Bombardieri E. Guidelines for radioiodine therapy of differentiated thyroid cancer Eur. J. Nucl. Med. Mol. Imaging 2008351941195910.1007/s 00259-008-0883-118670773 · doi ↗ · pubmed ↗
- 4Iwano S. Kato K. Nihashi T. Ito S. Tachi Y. Naganawa S. Comparisons of I-123 diagnostic and I-131 post-treatment scans for detecting residual thyroid tissue and metastases of differentiated thyroid cancer Ann. Nucl. Med.20092377778210.1007/s 12149-009-0303-z 19787312 · doi ↗ · pubmed ↗
- 5Jun S. Lee J.J. Park S.H. Kim T.Y. Kim W.B. Shong Y.K. Ryu J.S. Prediction of treatment response to 131I therapy by diffuse hepatic uptake intensity on post-therapy whole-body scan in patients with distant metastases of differentiated thyroid cancer Ann. Nucl. Med.20152960361210.1007/s 12149-015-0983-525980591 · doi ↗ · pubmed ↗
- 6Kim K. Kim S.J. Kim I.J. Kim Y.K. Kim B.S. Pak K. Clinical significance of diffuse hepatic visualization and thyroid bed uptake on post-ablative iodine-131 whole body scan in differentiated thyroid cancer Onkologie 201235828610.1159/00033680522414970 · doi ↗ · pubmed ↗
- 7Torlontano M. Crocetti U. Augello G. D’Aloiso L. Bonfitto N. Varraso A. Dicembrino F. Modoni S. Frusciante V. Di Giorgio A. Comparative evaluation of recombinant human thyrotropin-stimulated thyroglobulin levels, 131I whole-body scintigraphy, and neck ultrasonography in the follow-up of patients with papillary thyroid microcarcinoma who have not undergone radioiodine therapy J. Clin. Endocrinol. Metab.200691606310.1210/jc.2005-118516219716 · doi ↗ · pubmed ↗
- 8Haddad R.I. Bischoff L. Ball D. Bernet V. Blomain E. Busaidy N.L. Campbell M. Dickson P. Duh Q.Y. Ehya H. Thyroid Carcinoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology J. Natl. Compr. Canc Netw.20222092595110.6004/jnccn.2022.004035948029 · doi ↗ · pubmed ↗