Emerging Technologies for Exploring the Cellular Mechanisms in Vascular Diseases
Debasis Sahu, Treena Ganguly, Avantika Mann, Yash Gupta, Logan R. Van Nynatten, Douglas D. Fraser

TL;DR
New technologies like single-cell sequencing and AI are helping researchers better understand vascular diseases at the cellular level, paving the way for more precise diagnostics and treatments.
Contribution
The paper reviews emerging technologies and their translational potential for understanding and treating vascular diseases at the cellular and molecular level.
Findings
Single-cell and spatial transcriptomics enable high-resolution mapping of cellular heterogeneity in vascular diseases.
AI and multi-omics approaches improve data integration and identification of disease-driving cell types and gene programs.
Organ-on-chip and optogenetics provide physiologically relevant models for studying vascular pathology.
Abstract
Vascular diseases (VDs) and cardiovascular diseases (CVDs) are the leading causes of morbidity and mortality worldwide. Current diagnostic and therapeutic approaches are limited by insufficient resolution and a lack of mechanistic understanding at the cellular level. Traditional imaging and clinical assays do not fully capture the dynamic molecular and structural complexities underlying vascular pathology. Recent technological innovations, including single-cell and spatial transcriptomics, super-resolution and photoacoustic imaging, microfluidic organ-on-chip platforms, Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)/CRISPR-associated protein 9 (Cas9)-based gene editing, and artificial intelligence (AI), have created new opportunities for investigating the cellular and molecular basis of VDs. These techniques enable high-resolution mapping of cellular heterogeneity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
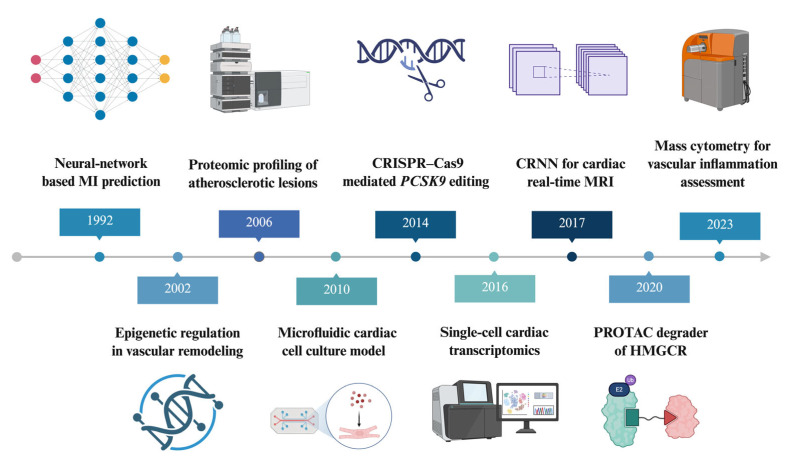 Figure 1
Figure 1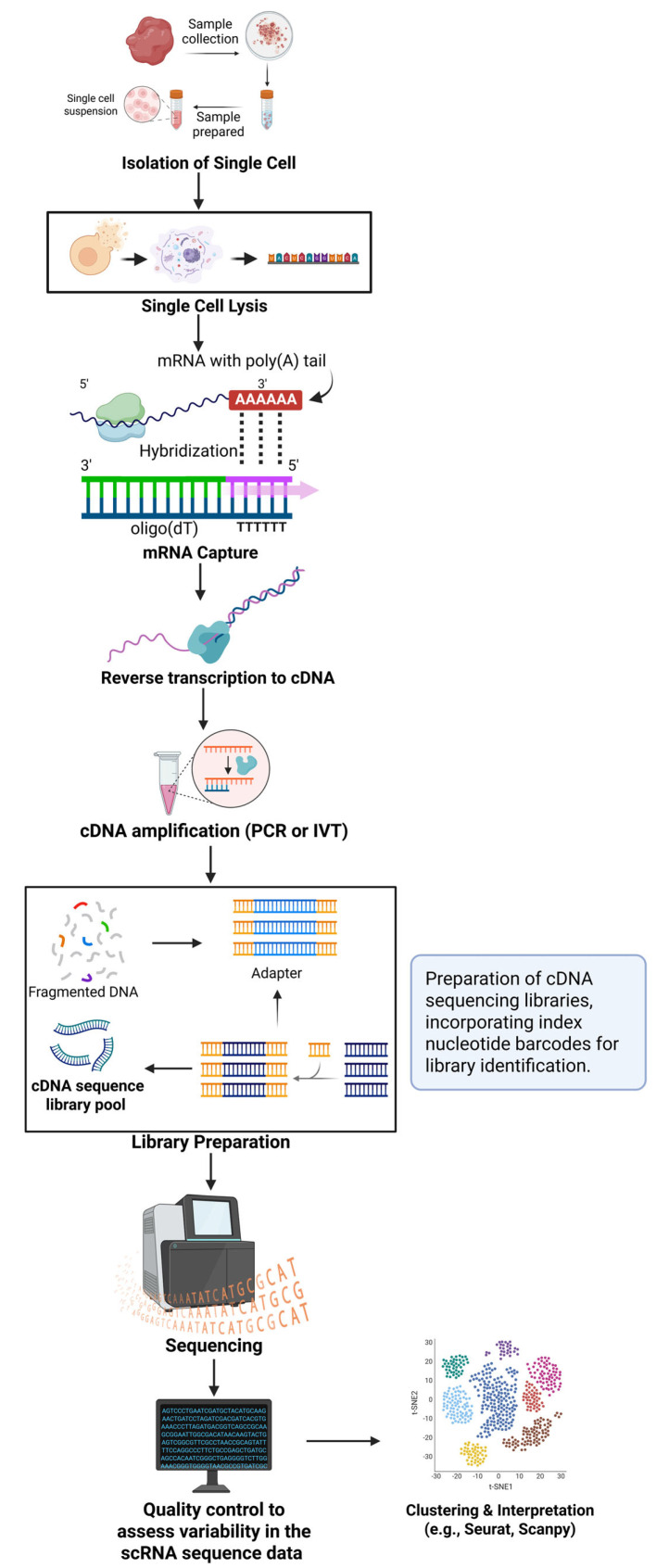 Figure 2
Figure 2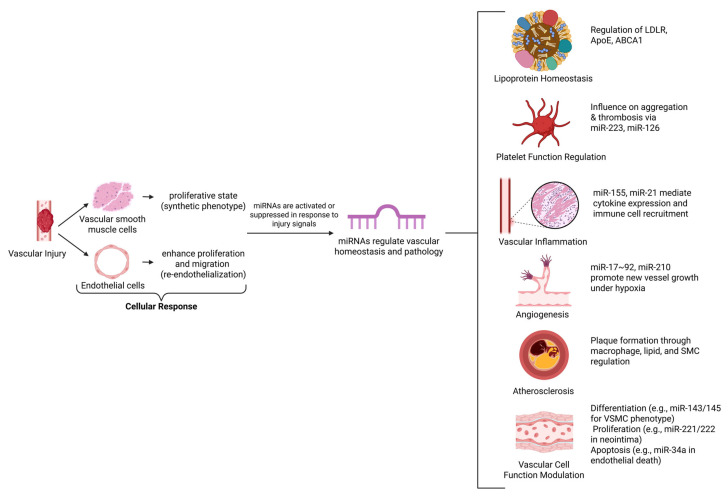 Figure 3
Figure 3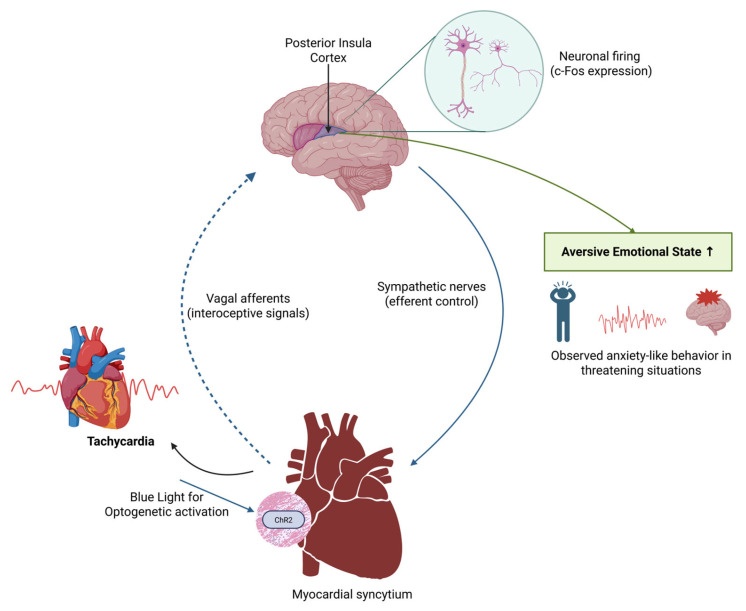 Figure 4
Figure 4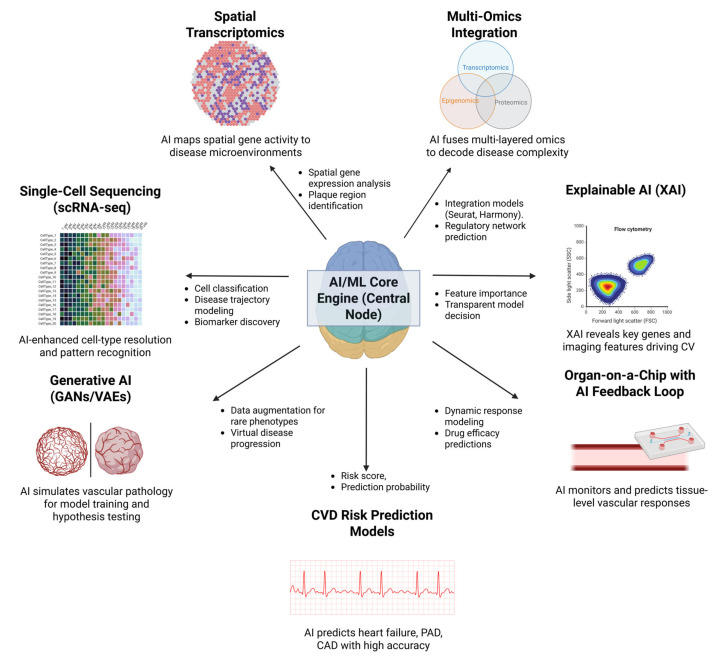 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSingle-cell and spatial transcriptomics · Angiogenesis and VEGF in Cancer · Cell Image Analysis Techniques
1. Introduction
Vascular diseases (VDs) continue to be a major cause of morbidity and mortality worldwide, contributing significantly to the global burden of cardiovascular diseases (CVDs). According to the World Health Organization (WHO), approximately 18 million people die each year from CVDs, with ischemic heart disease and stroke being the leading contributors [1]. The underlying pathology of most CVDs is atherosclerosis, a chronic inflammatory and degenerative process of the vascular wall that leads to events such as myocardial infarction, stroke, aneurysm rupture, and peripheral arterial disease [2]. Established risk factors, including smoking, obesity, hyperlipidemia, hypertension, and advancing age, accelerate vascular injury and maladaptation [3,4]. Despite advances in surgery, endovascular procedures, and pharmacological strategies, treatment options remain limited, and outcomes are unsatisfactory for many patients [5]. Conventional diagnostic and research tools, such as angiography, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), have provided invaluable insights into vascular pathology; however, they are limited by their resolution, sensitivity, and inability to capture dynamic molecular processes [6]. Addressing these limitations requires novel methodologies that interrogate vascular disease at the cellular and subcellular levels, offering mechanistic insights and translational opportunities [7,8,9].
In recent years, an array of new technologies has reshaped the study of vascular biology. Single-cell RNA sequencing (scRNA-seq) and spatial transcriptomics have enabled unprecedented resolution of cellular heterogeneity and tissue architecture in vascular lesions [10,11]. Microfluidic organ-on-chip platforms replicate physiological shear forces and multicellular interactions, bridging the gap between reductionist in vitro models and animal studies [11,12,13]. Optical and acoustic imaging approaches, including optogenetics, super-resolution microscopy, and photoacoustic tomography, provide spatiotemporal access to vascular dynamics [14]. At the genetic level, Clustered Regularly Interspaced Short Palindromic Repeats (CRISPR)/CRISPR-associated protein 9 (Cas9) or CRISPR/Cas9 enables precise perturbation of candidate pathways implicated in endothelial dysfunction and smooth muscle cell plasticity [15]. Computational frameworks, particularly machine learning (ML) and explainable artificial intelligence (AI), facilitate the integration of complex omics and imaging datasets for biomarker discovery, disease modeling, and risk prediction [16].
In this review, we focus on emerging technologies that provide cellular or near-cellular resolution and physiologically relevant modeling of vascular systems, and that have been applied to vascular or cardiovascular disease contexts or show a clear translational pathway. Specifically, we include single-cell and spatial omics, advanced imaging modalities, microfluidic and organ-on-chip systems, genetic perturbation tools such as CRISPR/Cas9 and optogenetics, and AI-based computational frameworks, including multiscale models and digital twins. Our central question is how these platforms deepen mechanistic understanding of vascular disease and how close each is to clinical translation, from discovery to early human applications. This review presents a timeline perspective on these emerging assays and platforms, highlighting their contributions to unraveling the cellular mechanisms underlying VDs. Figure 1 presents the evolutionary history of the techniques reviewed.
We discuss the key applications, strengths, limitations, and translational potential of each approach, emphasizing how technology integration can accelerate the development of clinically actionable biomarkers and therapies.
This study highlights emerging methodologies for understanding vascular disease mechanisms, emphasizing their historical development and translational potential.
Literature Selection
We identified relevant studies through searches of PubMed and Web of Science using combinations of terms related to vascular disease (e.g., “atherosclerosis,” “aneurysm,” “pulmonary hypertension,” “peripheral artery disease”), emerging technologies (e.g., “single-cell RNA sequencing,” “spatial transcriptomics,” “photoacoustic imaging,” “organ-on-chip,” “digital twin”), and translational keywords (e.g., “biomarker,” “clinical trial,” “validation”). We prioritized human studies and clinically relevant animal or in vitro models that provided mechanistic insight or translational implications. When describing technologies, we emphasize applications that directly address vascular biology, rather than generic technical capabilities.
2. Cellular and Molecular Resolution Approaches
2.1. Single-Cell RNA Sequencing
Over the past decade, advances in scRNA-seq technologies have enabled transcriptomic profiling at the individual cell level. Numerous studies have demonstrated that scRNA-seq is valuable for exploring epigenetics and cellular heterogeneity in VDs [26,27,28]. Significant differences in DNA methylation and histone modification patterns have been observed between cells from healthy and diseased aortic tissues. Researchers have identified several differentially methylated or modified genes related to inflammation and smooth muscle cell function, highlighting considerable heterogeneity in epigenetic modifications within both healthy and diseased samples [29]. These epigenetic changes may occur in specific cell types or subpopulations, which could have implications for the development of targeted therapies for CVDs. Further studies have explored the role of epigenetics in vascular disease [30]. For example, notable differences in DNA methylation patterns between atherosclerotic and non-atherosclerotic arteries suggest that epigenetic changes may contribute to atherosclerosis. Studies of histone modifications in vascular calcification have demonstrated that these modifications regulate gene expression. Additionally, research on abdominal aortic aneurysms has shown substantial differences in DNA methylation patterns between aneurysmal and non-aneurysmal tissues. Investigations of pulmonary arterial hypertension have revealed how histone modifications can influence gene expression related to this condition [31,32,33].
Interactions between different cell types are crucial for the development and progression of VDs, and scRNA-seq can elucidate these interactions. For example, the interplay between endothelial cells and smooth muscle cells is essential for normal vascular function, and dysfunction in this interaction can lead to disease. The scRNA-seq technology enhances our understanding of the cellular mechanisms underlying these diseases by identifying involved cell types, gene expression patterns, and their interactions, providing new insights into pathogenesis. Identifying novel cell types and gene expression signatures is critical for developing targeted therapies that address specific cellular mechanisms in vascular diseases [34,35]. The first scRNA-seq study was published in 2009 [36]. This powerful technique enables the identification of previously unknown cell subtypes, whole-transcriptome profiling, elucidation of phenotypic transitions, and confirmation or expansion of knowledge about various organs and systems. scRNA-seq has now been successfully applied to multiple organs and organ systems [11,36]. Its general workflow includes cell isolation, mRNA extraction, cDNA synthesis, and sequencing (see Figure 2). An integration of scRNA-seq data from 44,120 immune cells in 17 human atherosclerosis samples identified key immune cell types, such as pro-inflammatory CD4+ CD28null T cells and dysfunctional TREM2-SPP1+ foamy macrophages, linked to atherosclerosis progression and poor outcomes, suggesting these as potential therapeutic targets for precision medicine [37]. Therefore, scRNA-seq can identify specific disease mechanisms and therapeutic targets that may improve patient outcomes. As sequencing costs continue to decrease, scRNA-seq analysis of millions of cells per study will become more accessible. The development of centralized data repositories will further facilitate access to valuable cellular-level information. Improvements in mRNA capture efficiency are also anticipated, enhancing the sensitivity of gene expression analyses [38,39,40,41]. Integrating scRNA-seq with other modalities, such as proteomics and epigenomics, provides a holistic view of cellular biology. Sc RNA-seq is thus a vital diagnostic tool, aiding the detection of rare cells and informing treatment decisions across various diseases. Based on the results of genome-wide association studies (GWAS) and single-cell transcriptomics of vascular disease, specific genes and pathways implicated in VSMC and fibroblast cell transitions have been identified. Most of these single-cell studies are based on relatively small cohorts or preclinical models, and many of the identified cell states and gene signatures remain candidate biomarkers that require validation in larger, independent vascular datasets.
Using scRNA-seq, researchers were able to detect a correlation between vascular inflammation symptoms in Kawasaki disease and those associated with B-lymphocytes [42,43]. Transcriptomic profiling via scRNA-seq identified three palmitoylated genes, suggesting a role for S-palmitoylation in coronary artery disease (CAD) [38]. Bioinformatics analysis of the CMD rat model, based on scRNA-seq findings, indicated reductions in endothelial cells, an increase in fibroblast cells, oxidative stress, and an inflammatory response. Essential transcription factor-1 (ETF-1) has been identified as a primary target for vascular endothelial injury in diabetic cardiac disease using scRNA-seq [44,45]. A transcriptomic study employing clinical samples from patients with pulmonary arterial hypertension (PAH) identified primary glycolysis genes (CASP3, IGF1, CDKN2A, and KARS) associated with PAH through combined analysis of scRNA-seq and bulk transcriptomic data [46]. Two potential biomarkers (COL1A1 and C1QC) were identified for their association with atherosclerosis using scRNA-seq in combination with machine learning [47]. Enhanced expression of circular RNA during vascular cell differentiation has also been reported, suggesting it may serve as a potential biomarker for VD [48].
2.2. Epigenetic and Chromatin Accessibility Methods
Beyond transcriptional profiling, epigenetic mechanisms such as DNA methylation and histone modifications critically regulate gene expression programs in vascular cells. Epigenetic remodeling in endothelial cells, vascular smooth muscle cells (VSMCs), and infiltrating immune cells has been linked to the development and progression of atherosclerotic plaques, aneurysm formation, and vascular remodeling [49]. For example, altered promoter methylation and histone acetylation patterns in genes controlling inflammation, matrix remodeling, and contractile function have been associated with unstable plaque phenotypes and maladaptive VSMC transitions [50].
Recent advances in single-cell chromatin accessibility profiling, such as single-cell transposase-accessible chromatin using sequencing (scATAC-Seq) assay, allow the mapping of open chromatin regions at the level of individual vascular cells [51]. This provides complementary information to scRNA-seq by identifying enhancers and promoters that are active in specific cell states, including disease-associated macrophages, modulated VSMCs, and activated endothelial cells. In vascular disease models, integrating chromatin accessibility with gene expression has begun to reveal regulatory elements and transcription factors that drive pathogenic phenotypes. However, single-cell epigenomic assays remain technically demanding, and most applications in vascular biology are still in the discovery phase, with limited multi-center validation.
2.3. Proteomic and Single-Cell Proteomic Approaches in Vascular Disease
Whereas transcriptomic and epigenomic assays capture regulatory potential, proteomic technologies provide a direct readout of the effector layer that executes cellular programs in vascular disease [52]. Mass spectrometry–based proteomics enables unbiased quantification of thousands of proteins within vascular tissues, circulating blood, or isolated cell populations, revealing pathways involved in inflammation, extracellular matrix remodeling, thrombosis, and metabolic stress [53]. In atherosclerotic plaques, aneurysmal walls, and pulmonary vascular lesions, proteomic profiling has highlighted dysregulated complement components, matrix metalloproteinases, coagulation factors, and adhesion molecules that may contribute to plaque instability, aneurysm rupture, or microvascular dysfunction [54].
Targeted and discovery proteomics have also been applied to plasma and serum, where they support the identification of candidate circulating biomarkers for VDs, including proteins linked to endothelial injury, smooth muscle cell phenotypic switching, and immune activation [55]. These circulating signatures can complement imaging and clinical risk scores and may help stratify patients according to inflammatory burden or vascular remodeling activity [56]. In parallel, advances in high-dimensional single-cell proteomic platforms, such as mass cytometry (CyTOF), imaging mass cytometry, and oligo-tagged antibody panels integrated with scRNA-seq (e.g., CITE-seq), permit simultaneous measurement of dozens to hundreds of protein epitopes per cell. In vascular research, these approaches enable fine-grained mapping of endothelial, vascular smooth muscle, fibroblast, and immune cell phenotypes, including activation states and receptor–ligand expression profiles that are not fully captured at the transcript level.
Metabolomic profiling, often combined with proteomic data, further refines our understanding of vascular pathophysiology by characterizing bioactive lipids, amino acid derivatives, and energy metabolites associated with endothelial dysfunction, oxidative stress, and vascular inflammation [57]. However, most proteomic and metabolomic studies in vascular disease still involve modest cohort sizes, heterogeneous sample processing, and variable analytical pipelines. As a result, many proposed protein and metabolite signatures remain at the discovery or early validation stage, with limited multi-center replication and uncertain incremental value over established clinical risk factors.
2.4. Strategies and Challenges of Multi-Omics Integration
It is increasingly clear that single-layer molecular analyses are insufficient to capture the complexity of vascular remodeling, calcification, and inflammatory activation [58]. Multi-omics strategies that combine single-cell RNA sequencing (scRNA-seq), single-cell chromatin accessibility profiling (e.g., ATAC-seq), and proteomic or metabolomic readouts offer a more holistic view of cellular states and regulatory networks in vascular disease [59]. By jointly interrogating gene expression, chromatin accessibility, and protein abundance, these approaches enable the reconstruction of gene regulatory circuits, the identification of disease-associated transcription factors, and the linkage of upstream regulatory changes to downstream effector pathways within specific endothelial, smooth muscle, fibroblast, or immune cell subsets [60].
In atherosclerosis, aneurysm formation, and pulmonary vascular remodeling, multi-omics integration has been used to refine cell-state taxonomies and to dissect transitions such as vascular smooth muscle cell (VSMC) phenotypic switching, endothelial–mesenchymal transition, and macrophage polarization [61]. For example, pairing scRNA-seq with scATAC-seq allows assignment of active enhancers and promoters to lineage-defining transcription factors in modulated VSMCs or lesional macrophages, while proteomic measurements validate whether predicted signaling pathways are implemented at the protein level [61]. Such “vertical” integration across transcriptomic, epigenomic, and proteomic layers increases confidence that identified pathways are not artifacts of a single assay and supports the nomination of more robust therapeutic targets.
Advances in computational pipelines have improved the feasibility of these studies by enabling alignment and joint analysis of heterogeneous data types from the same or closely matched cell populations [62]. Tools such as Seurat, Signac, and Harmony support multi-modal integration, allowing researchers to embed cells in shared low-dimensional spaces, infer gene regulatory networks, reconstruct cell-fate trajectories, and model intercellular communication within vascular lesions. Network-based and machine-learning approaches further prioritize features that are conserved across modalities and cohorts and can begin to link multi-omics signatures to imaging phenotypes or clinical outcomes [63].
Despite this promise, multi-omics integration in vascular disease faces substantial challenges. Tissue availability is often limited, especially for human vascular specimens, leading to small sample sizes and reduced statistical power. Differences in tissue handling, library preparation, and platform chemistry introduce batch effects that complicate cross-study comparisons. At the analytic level, issues such as data sparsity, modality-specific noise, missing features across assays, and the risk of overfitting high-dimensional datasets remain significant obstacles. Furthermore, most published multi-omics studies in vascular disease rely on retrospective or cross-sectional cohorts, with only preliminary evidence that integrated molecular signatures improve prediction beyond clinical and imaging variables [64]. Addressing these limitations will require standardized protocols, larger multi-center datasets, transparent reporting of integration workflows, and prospective validation of multi-omics-derived biomarkers and targets in independent vascular cohorts.
3. Experimental and Engineering Platforms
Optogenetics
Optogenetics is a technique for controlling cellular activity using light, enabling precise manipulation of specific cell populations within heterogeneous tissues through genetic engineering. In recent years, optogenetics has become increasingly popular among researchers, enabling fine control over the expression of light-sensitive proteins. It has been used to investigate cell signaling, gene expression, and cell migration [65,66,67]. Optogenetics has been applied to study vascular smooth muscle cells (VSMCs), which undergo contractility changes that contribute to atherosclerosis in vascular disease [61,68]. Given the central role of VSMCs in VDs, optogenetics is now used to modulate their activity, providing new insights into underlying mechanisms. Optogenetic approaches control VSMC contractility and explore cellular mechanisms involved in VDs [69,70]. This technology has greatly enhanced our ability to study disease processes with unparalleled precision, revealing complex interactions between different cell types (Figure 3). Endothelium-targeted optostimulation has shown promise as an intervention for the vascular system. Optogenetics uses opsins to modulate cellular activity in response to light. Channelrhodopsins (e.g., ChR2), activated by 470 nm blue light, depolarize cells via sodium and calcium influx, enabling activation on the millisecond scale. Inhibitory opsins, such as halorhodopsins (NpHR, 590 nm yellow light) and archaerhodopsins (ArchT, 530 nm green light), hyperpolarize cells by pumping chloride or protons, effectively silencing activity [71]. Red-shifted variants like ChrimsonR (590 nm) enhance tissue penetration for deeper vascular targeting. Cell-type specificity is achieved using promoters (e.g., Myh11 for VSMCs, Tie2 for endothelial cells) delivered via adeno-associated viruses (AAVs) or lentiviral vectors, with Cre-lox systems allowing temporal control [72,73,74]. Light can be delivered by fiber optics or two-photon microscopy, providing 10–100 µm resolution, as demonstrated by 473 nm laser-induced calcium transients in murine carotid arteries [75].
While optogenetic approaches have yielded precise control of vascular and cardiac activity in preclinical models, including modulation of vascular tone and cardiac sympathetic nerve activity, no routine clinical applications in human vascular disease currently exist [76]. Major translational barriers include challenges in delivering light to deep vascular structures, safe and efficient gene delivery of opsins, potential immunogenicity, and the need for long-term safety data [77]. Consequently, most proposed therapeutic applications of optogenetics in vascular medicine remain speculative extensions of the experimental work described above.
Optogenetic regulation of cardiac sympathetic nerve (CSN) activity effectively prevents myocardial ischemia (MI)-induced ventricular arrhythmias [76]. However, optogenetics faces limitations, notably the requirement for light to activate light-sensitive proteins, which is a significant obstacle in vivo since light cannot always penetrate deep tissues [78]. A clinically applicable version of optogenetics remains under development. Combining optogenetics with systems biology approaches (e.g., transcriptomics, proteomics) helps elucidate network-level responses in cardiovascular disease (CVD). Organ-on-a-chip platforms integrated with optogenetics mimic vascular physiology and enable studies of mechanical stress or drug responses in human-relevant models [79]. These approaches enhance the translational relevance of optogenetic findings. The specific applications of optogenetics across various cardiovascular cell types and disease models, along with their associated mechanisms, challenges, and proposed future directions, are summarized in Table 1.
4. Imaging Innovations
Modern imaging technologies are transforming the study of vascular biology by extending the limits of resolution, penetration depth, and temporal fidelity beyond those of conventional modalities such as ultrasound, CT, and MRI. These advances have enabled visualization of vascular processes at scales ranging from nanometers to intact tissue, providing mechanistic insights previously inaccessible.
4.1. Super-Resolution Microscopy/Nanoscopy
Conventional imaging techniques such as X-rays, CT, and MRI have limitations in resolution and sensitivity. Recent advances in imaging techniques have enabled researchers to study VDs at the cellular level, offering insights into their mechanisms [80]. Super-resolution microscopy or nanoscopy techniques, including super-resolution ultrasound (SRU), multimodal ultrafast sonography microscopy (MUSM), ultrasound localization microscopy (ULM), photoacoustic tomography (PAT), intravital microscopy (IVM), SRμT (synchrotron radiation micro-tomography), and E-uPIV (enhanced ultrasound particle image velocimetry), allow visualization of intracellular structures beyond the diffraction limit of light [81]. In VDs, the breakdown of the endothelial glycocalyx compromises vascular permeability, increasing leukocyte access to the arterial intima, promoting inflammation, and disrupting protective endothelial signaling. Advanced imaging methods, such as super-resolution microscopy and intravital microscopy, provide real-time, high-resolution visualization of cellular processes, including leukocyte-endothelial interactions and platelet activation, in vascular disease.
Optical coherence tomography also provides detailed imaging of the arterial wall, aiding in assessing atherosclerosis progression and the effectiveness of interventions such as stenting. These technologies improve our understanding of vascular pathology and support the development of innovative diagnostic and therapeutic strategies [82]. Photoacoustic imaging, a noninvasive super-resolution microscopy technique, enables visualization of blood vessels and tissues with high resolution and sensitivity. Microvascular imaging of tumors and other diseases has been achieved using photoacoustic tomography [83]. In another study, photoacoustic imaging was used to assess the effects of high-fat diets on atherosclerosis development [84,85]. A recent investigation demonstrated that a high-fidelity 3D-PAT scanner is a promising tool for obtaining in vivo 3D images of vascular anatomy. High-resolution PAT enables visualization of deep-seated blood vessels across different body positions [86]. Three-dimensional photoacoustic imaging visualizes foot vasculature using multi-element (~128-element) transducers. SRμT refers to super-resolution microscopy techniques using synchrotron radiation to generate high-resolution 3D images beyond the diffraction limit [87]. SRμT provided high-resolution images of vascular calcification that were not achievable with other imaging methods.
A study using a murine model of Alzheimer’s disease detected microvascular dysfunction (MVD) with IVM, suggesting a role for MVD in the progression of Alzheimer’s disease pathology. Another investigation developed an intravital heart micro-imaging protocol enabling real-time imaging of cardiac tissue in a live animal model. Super-resolution ULM detects changes in blood flow by visualizing deep-seated restricted vessels. Human blood vessels can be resolved 5.7 times better with super-resolution ULM compared to contrast-enhanced power Doppler [86]. SRU facilitates visualization of vascular reorganization in the neonatal brain at depths of a few microns [88]. It also enables measurement of vascular flow dynamics and offers a sevenfold improvement in vascular imaging over traditional contrast ultrasound [89,90]. SRU is a reliable tool for obtaining high-resolution vascular images, including spatiotemporal images. In the L-NAME (Nω-nitro-L-arginine methyl ester) and angiotensin-II-induced hypertension mouse model, MUSM provides high-resolution images of vascular dynamics. E-uPIV allows visualization of microvasculature and accurate measurement of blood flow [91].
Intravital microscopy (IVM) adds a dynamic dimension by enabling direct visualization of the vascular microenvironment in living organisms. This technique allows real-time tracking of leukocyte–endothelial interactions, platelet adhesion, and thrombus formation under physiological shear forces. Intravital imaging has been indispensable for dissecting the spatiotemporal organization of inflammation, coagulation, and vascular remodeling, providing insights that cannot be gained from static tissue sections. Its versatility spans multiple organ systems, including the brain, heart, and peripheral vasculature, making it a powerful tool for studying how systemic diseases manifest at the microvascular level [92,93].
These imaging modalities complement one another; super-resolution microscopy excels at subcellular resolution, PAT offers label-free molecular contrast at tissue depth, and IVM reveals dynamic interactions in real time [94,95]. Together, they form a powerful imaging toolbox that links molecular events to functional outcomes in vascular disease. The translational trajectory is already emerging, especially with PAT, which is being piloted in clinical trials for vascular diagnostics. However, several challenges remain, such as the need for standardized protocols, miniaturization of imaging hardware, cost reduction, and robust validation across diverse patient populations.
4.2. Photoacoustic Imaging and Tomography
Photoacoustic imaging (PAI), including multispectral optoacoustic tomography (MSOT) and volumetric photoacoustic tomography, combines optical contrast with ultrasonic detection to enable high-resolution visualization of hemoglobin, lipids, and other chromophores in deep tissues. In preclinical vascular disease models and early human studies, PAI has been used to assess peripheral perfusion, microvascular remodeling, and plaque composition, providing functional information that complements Doppler ultrasound and conventional angiography. By capturing dynamic changes in tissue oxygenation and vascular density, photoacoustic techniques offer mechanistic insight into ischemia, neovascularization, and microvascular dysfunction. Recent clinical translation studies demonstrate that MSOT can discriminate symptomatic peripheral arterial disease (PAD) from healthy volunteers using hemoglobin-related calf-muscle biomarkers, while new all-optical three-dimensional PAI scanners deliver clinically useful microvascular images with acquisition speeds suitable for pilot clinical evaluations. Collectively, these advances highlight PAI’s potential as a bedside adjunct to Doppler ultrasound and angiography for functional perfusion assessment and plaque microenvironment phenotyping in PAD, diabetic microangiopathy, and related vascular disorders [96].
5. Microfluidic and Organ-on-Chip Systems
5.1. Hemodynamic Modeling
Microfluidic technologies and organ-on-chip (OoC) systems have emerged as powerful experimental platforms for modeling vascular biology in controlled environments that recapitulate key physiological conditions. Unlike conventional static culture systems, these devices utilize microscale channels lined with endothelial or smooth muscle cells. They are perfused with fluid to mimic the mechanical and biochemical cues experienced in vivo. This approach enables precise investigation of how hemodynamic forces, cellular interactions, and biochemical gradients contribute to vascular health and disease [94,97,98].
One of the most significant advantages of these systems is their ability to model hemodynamics and shear stress. Endothelial cells cultured under laminar flow conditions in microfluidic channels align in the direction of flow and exhibit anti-inflammatory, antithrombotic phenotypes, closely resembling the behavior of vascular endothelium in vivo [99]. In contrast, disturbed flow patterns, such as those at arterial bifurcations, can be replicated in microfluidic devices and have been shown to promote endothelial dysfunction, oxidative stress, and pro-atherogenic signaling [100]. These models enable researchers to dissect mechanotransduction pathways and test how pharmacological interventions might restore protective endothelial responses.
5.2. Thrombosis-on-Chip and Patient-Derived Platforms
Microfluidic platforms have also advanced thrombosis research. “Thrombosis-on-chip” devices simulate blood flow across surfaces coated with collagen or tissue factor, enabling real-time visualization of platelet adhesion, aggregation, and fibrin formation [101]. These systems have proven invaluable for studying the mechanisms of clot initiation, evaluating patient-specific coagulation profiles, and screening novel antithrombotic agents under physiologically relevant shear conditions. By replicating arterial or venous flow rates, these chips enable a more accurate assessment of thrombosis risk than static assays.
Another innovation is the incorporation of patient-derived induced pluripotent stem cells (iPSCs) into vascular chips. These iPSC-derived endothelial or smooth muscle cells allow modeling of genetic vascular disorders, such as aneurysm syndromes or inherited thrombophilias, in a personalized context. Using cells from affected individuals, OoC platforms can replicate disease-specific phenotypes and serve as testbeds for evaluating targeted therapeutic interventions. This personalized approach offers exciting opportunities for precision medicine, where therapies can be tailored and tested in vitro before clinical application [102,103,104].
Despite their promise, microfluidic and OoC technologies face important limitations. Variability in device design and fabrication complicates reproducibility across laboratories. Throughput remains limited compared to high-content screening methods, and standardization of culture conditions, readouts, and validation criteria is still evolving. Furthermore, while these systems approximate vascular physiology more closely than static cultures, they cannot fully replicate the complexity of whole-organ or systemic interactions. Nevertheless, these platforms have considerable potential. By bridging the gap between reductionist cell culture and animal models, microfluidic and organ-on-chip technologies provide a versatile and physiologically relevant environment for vascular research. As engineering approaches mature and protocols become standardized, these systems will likely play an increasingly central role in drug discovery, disease modeling, and personalized medicine for VDs.
5.3. Vascular Organoids and Organ-on-a-Chip Systems
Organ-on-a-chip platforms enhance physiological relevance by integrating microfluidic channels and controlled biomechanical cues (e.g., shear stress, pulsatile flow) into engineered vascular constructs. These systems mimic organ-level functions and vascular microenvironments, allowing real-time observation and manipulation of cell behavior under near-physiological conditions [105,106]. For example, models simulating blood–brain barrier (BBB) permeability have been developed to study vascular leakage in stroke and neurodegenerative conditions [107]. Vascular chips that mimic hypertensive microcirculation enable the investigation of endothelial barrier disruption and remodeling under elevated pressure gradients. These organ-on-a-chip systems allow modeling of disease-specific phenotypes, including inflammatory endothelial activation, thrombogenesis, and oxidative stress. Additionally, these technologies are highly amenable to high-throughput drug screening and personalized medicine, as they can incorporate patient-derived induced pluripotent stem cells (iPscRNA-seq) to generate genetically matched vascular tissues for therapeutic testing [108].
Importantly, vascular organoids and chips support multicellular integration, enabling the study of complex interactions among endothelial cells, vascular smooth muscle cells, immune cells, and fibroblasts. These cellular interactions are critical in processes such as atherosclerosis, restenosis, and vascular calcification. Furthermore, these platforms provide a controlled environment for assessing the effects of therapeutic agents on vascular permeability, tone regulation, and inflammatory responses, making them valuable tools for preclinical drug development and toxicology assessment.
5.4. Limitations, Reproducibility, and Ethical Considerations
Despite their promise, microfluidic and organ-on-chip technologies face essential limitations. Device design, fabrication protocols, and surface treatments vary across laboratories, leading to substantial variability in readouts and complicating reproducibility. Endothelial cells and supporting stromal cells exhibit marked heterogeneity across vascular beds, donors, and culture conditions, and capturing this diversity in simplified chip systems remains challenging. Long-term culture under flow is technically demanding, and maintaining stable, physiologically relevant phenotypes over extended periods is difficult. Moreover, current platforms often lack the full systemic context of human vascular disease, including interactions with the immune, nervous, and endocrine systems. The use of patient-derived iPSCs raises logistical and ethical questions related to consent, data protection, and equitable access to these personalized models. As a result, vascular microfluidic and organ-on-chip systems should be viewed as intermediate models that complement, rather than fully replace, animal studies and clinical investigations.
6. Computational and Genetic Approaches
6.1. CRISPR/Cas9 Gene Editing
CRISPR/Cas9 is a novel technology that utilizes cut-and-paste mechanisms to enable gene modifications. This approach provides a better understanding of underlying disease mechanisms and opens new avenues for developing treatments [109,110]. Evidence from investigations has shown that CRISPR/Cas9 is a useful tool for studying CVDs. The involvement of the ATP-binding cassette transporter (ABC)A1 gene in atherosclerosis development has been documented using CRISPR/Cas9 technology. Various microRNAs implicated in the development of atherosclerosis and hypertension include miR-126, miR-155, and miR-21 (Figure 4). MiR-126 is an endothelial-specific microRNA that plays a critical role in vascular homeostasis, and its deletion using CRISPR/Cas9 leads to impaired angiogenesis and increased susceptibility to atherosclerosis [111]. In a CRISPR/Cas9 gene editing study on mouse models, miR-145 ablation increased atherosclerotic plaque formation. One study demonstrated that deletion of miR-33 led to reduced atherosclerosis and improved lipid metabolism. Another study designed a CRISPR/Cas9 gene editing model to analyze the functional aspects of missense variants identified in CHD [112]. Additionally, a CRISPR/Cas9 study found that Cas9 expression did not impact cardiac function [113]. Several studies have examined the role of various genes and proteins in the development mechanisms of genetic heart disease.
These underscore the precision of single-cell approaches in identifying functional genetic elements. But to date, most CRISPR/Cas9 applications in vascular biology have been confined to in vitro systems or animal models, providing mechanistic insights into gene function and disease pathways. No CRISPR-based therapies are yet approved specifically for vascular indications, and major challenges remain regarding off-target effects, safe and efficient delivery to vascular tissues, immune responses, and long-term safety assessment.
The key molecular targets, including specific genes and microRNAs explored in cardiovascular disease using functional studies and genome-editing approaches, are further summarized in Table 2.
6.2. Machine Learning (ML) and Explainable AI (XAI)
While machine learning (ML) and artificial intelligence (AI) have shown substantial promise in predicting CVD risk, patient outcomes, and treatment response, a significant limitation of traditional models is their “black-box” nature. These models often lack interpretability, making it difficult for clinicians to understand the rationale behind predictions. Explainable artificial intelligence (XAI) addresses this challenge by providing tools and frameworks that elucidate the decision-making process of AI models, thereby enhancing their transparency, interpretability, and clinical trust, In the vascular domain, ML models have been developed to automatically segment vessels, quantify plaque burden, and predict outcomes such as stroke or limb ischemia from CT angiography, MRI, and ultrasound data. XAI approaches, including feature attribution methods, have begun to reveal which imaging-derived features and clinical variables most strongly drive these predictions, providing potential mechanistic clues and highlighting candidate biomarkers.
XAI techniques allow researchers and clinicians to identify key features, such as specific genes, signaling pathways, imaging-derived variables, or clinical biomarkers, that most significantly contribute to model predictions. For instance, when applied to large-scale patient data in vascular disease contexts, XAI can reveal which molecular signatures (e.g., pro-inflammatory cytokines or extracellular matrix-related genes) are most associated with plaque instability or vascular remodeling [114,115]. These insights go beyond mere classification, providing mechanistic clues into disease progression and patient heterogeneity.
The application of XAI in cardiovascular research is a critical advancement for bridging the gap between computational model outputs and actionable clinical knowledge. XAI frameworks, such as Shapley Additive exPlanations (SHAP), Local Interpretable Model-agnostic Explanations (LIME), and counterfactual reasoning, can be applied to diverse data modalities, including transcriptomics, imaging, and electronic health records. For VDs specifically, these tools facilitate the dissection of complex, nonlinear relationships between risk factors (e.g., hypertension, lipid levels, genetic variants) and disease phenotypes, such as arterial stiffness, aneurysm formation, or calcific lesion burden.
Importantly, XAI improves model transparency and supports the development of clinically actionable models. Identifying influential features facilitates risk stratification, prioritization of therapeutic targets, and refinement of personalized treatment strategies. For example, if an AI model predicts a high risk for atherosclerotic events, XAI can specify whether the prediction was driven primarily by inflammatory gene expression, vascular imaging patterns, or metabolic profiles, enabling more precise interventions. Furthermore, XAI can help validate novel hypotheses derived from omics data in translational research settings. When integrated with multi-omics approaches, XAI can trace how gene regulatory changes translate into phenotypic outcomes and link them with clinically measurable features, such as ankle-brachial index or carotid intima-media thickness. This cross-validation improves both model robustness and biological relevance.
A persistent challenge is that many models are trained and validated on single-center datasets with limited demographic diversity, which raises concerns about generalizability and bias. Performance can deteriorate when models are applied to new scanners, imaging protocols, or patient populations. Robust external validation, prospective testing, and monitoring of failure modes are therefore essential before ML and XAI tools can be safely integrated into routine vascular care.
6.3. Generative AI Models: VAEs and GANs
Generative artificial intelligence (AI) models, particularly variational autoencoders (VAEs) and generative adversarial networks (GANs), represent a powerful advancement in deep learning and are increasingly applied in CVD research. Unlike discriminative models, which focus solely on classification or regression, generative models learn the underlying data distribution, enabling them to generate new synthetic data that closely mimics real-world biological variation. These capabilities are leveraged to simulate disease progression, augment limited datasets, and support virtual experimentation in vascular biology.
Variational autoencoders (VAEs) combine Bayesian inference principles with neural encoding-decoding architectures to learn compressed, low-dimensional representations of complex datasets. In vascular research, VAEs can be applied to high-dimensional omics or imaging data to identify latent variables that describe the progression from healthy vasculature to pathological states such as atherosclerosis, arterial stiffness, or aneurysm formation. These latent variables can serve as interpretable biomarkers or be used to simulate disease trajectories under different genetic or environmental conditions [116,117,118]. For example, VAEs trained on time-series omics data can model smooth transitions in cell states during vascular remodeling or endothelial-to-mesenchymal transition.
GANs consist of a generator and a discriminator network trained in a competitive framework, making them particularly adept at producing high-fidelity synthetic data. In the cardiovascular domain, GANs have been employed to generate synthetic vascular images (e.g., CT angiography, ultrasound, histopathology) that preserve the structural and pathological features of real data [119,120,121]. This approach is especially valuable when annotated clinical datasets are scarce or imbalanced. GAN-generated data can augment training sets for downstream AI tasks such as vessel segmentation, plaque detection, or phenotype classification, thereby improving model robustness and generalizability.
Advanced applications of GANs also include disease progression modeling, in which the generator is conditioned to simulate vascular changes over time, such as calcification accumulation, lumen narrowing, or wall thickening under various risk scenarios. Conditional GANs (cGANs) and style-transfer GANs can further transform healthy tissue images into synthetic diseased states, providing insights into early pathological changes that may not be apparent in limited clinical samples [122,123].
Furthermore, generative models can assist in in silico experimental design, allowing simulated vascular datasets to be used for hypothesis testing, treatment response prediction, and modeling patient-specific disease risk. Integrating multi-omics and imaging data enables these models to generate biologically plausible outputs that reflect the interplay between gene regulation, protein expression, and structural remodeling. While generative AI models offer substantial promise, challenges remain, including ensuring biological plausibility, avoiding mode collapse in GANs, and validating synthetic data against empirical findings. As training frameworks, interpretability tools, and validation protocols advance, generative models are poised to become integral to predictive vascular research and precision cardiovascular medicine. The technologies ranging from single-cell omics and advanced imaging to organ-on-chip platforms and CRISPR/Cas9 systems represent a profound shift in vascular research. While each offers unique strengths in resolution or physiological relevance, they all face shared and distinct limitations concerning scalability, cost, in vivo applicability, and regulatory approval. To provide a comparative assessment and set the stage for discussing multimodal integration, Table 3 offers a synthesis of the key features, applications, strengths, limitations, and overall translational potential of the emerging techniques.
6.4. Multiscale Modeling: Linking Physics, AI, and Omics
Multiscale modeling integrates mathematical and computational approaches that span different biological and physical scales, from molecular dynamics and gene regulatory networks to cell–cell interactions, tissue biomechanics, and whole-organ hemodynamics [124]. Traditionally, computational fluid dynamics (CFD) models have been used to study vascular flow patterns, shear stress, and pressure distributions in arteries. Recent advances connect these physics-based models with ML algorithms and omics data, enabling a more comprehensive understanding of how molecular changes manifest as measurable hemodynamic outcomes [125,126].
CFD models simulate blood flow using the Navier–Stokes equations, applied to patient-specific anatomical geometries derived from CT or MRI angiography. When integrated with omics data (such as endothelial gene expression profiles under disturbed flow), these models can predict how shear stress influences inflammatory activation, plaque formation, or endothelial dysfunction [127]. ML and AI are increasingly used to optimize model parameters, reduce computational burden, and uncover nonlinear relationships between local flow environments and disease phenotypes.
Despite significant advances, multiscale models are still limited by high computational costs, complex boundary condition requirements, and uncertainties in integrating molecular data with macroscopic hemodynamics [28,128]. Model validation remains challenging because it is difficult to obtain simultaneous ground-truth hemodynamic and molecular measurements in humans. Furthermore, interoperability among datasets, imaging, omics, and biomechanical models is not yet standardized, which hampers reproducibility across studies.
6.5. Digital Twins: Toward Personalized Vascular Simulations
A digital twin is a virtual replica of a patient’s vascular system that is continuously updated with imaging, physiological, and molecular data to simulate disease progression and treatment outcomes. This concept, originally applied in aerospace and manufacturing, is gaining momentum in biomedicine. In cardiovascular contexts, digital twins integrate high-resolution anatomical models derived from imaging with patient-specific biomarkers, risk factors, and sometimes omics profiles [129].
The digital twin functions as a dynamic computational model. For example, patient-derived coronary CT angiograms are used to reconstruct arterial geometry, while hemodynamic simulations predict fractional flow reserve (FFR) [130]. As longitudinal data, such as repeat imaging or blood biomarkers, are incorporated into the model, it can forecast plaque progression or response to therapy. Integration of omics data adds further personalization by predicting how an individual’s transcriptomic or proteomic signature may influence vascular remodeling under hypertensive stress [131,132].
The main limitations are the data intensity required and regulatory uncertainty. Creating accurate digital twins demands high-quality longitudinal datasets, which are seldom available in clinical practice [133]. The computational requirements are substantial, and models are only as reliable as the assumptions underlying them. Furthermore, digital twins are still considered investigational tools; their clinical utility must be demonstrated in prospective trials before widespread adoption. Issues related to data privacy and model interpretability also remain unresolved.
6.6. Targeted Protein Degradation
PROTACs (proteolysis targeting chimeras) are innovative molecules that induce targeted protein degradation by recruiting E3 ubiquitin ligases to specific substrates. Unlike gene editing, which changes DNA sequences, PROTACs adjust protein levels directly. In 2020, a study reported the first PROTAC degrader targeting transmembrane HMGCR (3-Hydroxy-3-Methylglutaryl-CoA Reductase). This PROTAC overcomes statin resistance by inhibiting cholesterol biosynthesis without causing HMGCR upregulation [24].
7. Integration and Translational Outlook
7.1. scRNA-Seq Spatial Transcriptomics: Illuminating Gene Expression Within Vascular Architecture
Spatial transcriptomics (ST) marks a revolutionary advancement in transcriptomic profiling by preserving the spatial context of gene expression within intact tissue architecture. Unlike bulk or scRNA-seq, which disrupts tissue organization, ST preserves transcript localization, enabling researchers to visualize gene expression patterns alongside histological features. This approach is particularly transformative for cardiovascular and vascular disease studies, where the cellular microenvironment and spatial organization play crucial roles in disease pathogenesis [96,97,98].
In VDs such as atherosclerosis, aneurysms, and vascular remodeling, ST enables detailed mapping of transcriptional activity across specific regions within diseased tissue [99]. For example, a study using spatial transcriptomics to analyze atherosclerotic plaques revealed distinct zones of inflammation, necrosis, and fibrous tissue, each characterized by unique gene expression signatures linked to immune activation, extracellular matrix remodeling, and lipid metabolism. This level of resolution helps identify disease-driving cell types and interactions otherwise masked in dissociated single-cell analyses. ST clarifies the complex crosstalk between endothelial cells, vascular smooth muscle cells (VSMCs), fibroblasts, and immune cells in spatially confined regions by overlaying transcriptomic data on histological images [100]. For instance, macrophage subtypes enriched in pro-inflammatory cytokines can be mapped adjacent to lipid cores in plaques. At the same time, smooth muscle cell-derived foam cells may localize to fibrous cap regions, highlighting potential targets for intervention.
Spatial transcriptomics has also shown promise in characterizing aneurysmal walls, where gene signatures related to matrix degradation, angiogenesis, and immune cell infiltration are distributed heterogeneously. Understanding these spatial dynamics reveals mechanisms of disease progression and provides a basis for designing region-specific drug-delivery strategies or identifying tissue zones susceptible to rupture. Integrating ST with other omics technologies, such as scRNA-seq and proteomics, can further advance our understanding of vascular pathology. Such multimodal datasets support cross-validation of findings and help dissect the relationships among gene expression, protein localization, and functional changes in situ [98]. Additionally, the development of high-throughput spatial barcoding and advanced imaging platforms continues to enhance ST’s resolution and scalability, making it increasingly suitable for large-scale studies of human cardiovascular disease.
7.2. Multi-Omics Integration (scRNA-Seq, ATAC-Seq, and Proteomics)
Figure 5 presents a schematic of an AI/ML-centered framework integrating multi-omics, single-cell sequencing, spatial transcriptomics, generative AI, explainable AI, organ-on-a-chip systems, and risk prediction models to enhance cardiovascular disease modeling, prediction, and therapeutic optimization.
8. Clinical Translation and Regulatory Science
Several emerging technologies discussed in this review are already progressing from bench to bedside, with early-phase human studies and developing regulatory frameworks shaping their clinical adoption. In this section, we differentiate technologies that have already entered clinical workflows or early human studies from those that remain preclinical or exploratory, and we highlight key regulatory, validation, and implementation challenges specific to vascular disease.
8.1. Spatial Transcriptomics in Vascular and Oncologic Specimens
While spatial transcriptomics remains primarily a research tool, it has been successfully applied to resected human atherosclerotic plaques and to surgical vascular tissues. These studies have mapped region-specific immune, fibro-calcific, and angiogenic signatures, providing spatially anchored biomarkers that distinguish stable from rupture-prone plaques. Similar approaches have been incorporated into translational oncology trials, establishing methodological precedents and pipelines that can be adapted for cardiovascular research. The convergence of these efforts will accelerate biomarker discovery and may eventually support patient stratification in clinical trials of anti-inflammatory or plaque-stabilizing therapies [134,135]. Despite its power, spatial transcriptomics is currently restricted to research settings. No spatial transcriptomics-based assays are approved for clinical vascular diagnostics, and substantial barriers related to tissue handling, cost, standardization, and data interpretation must be addressed before clinical deployment.
8.2. Integration of Artificial Intelligence into Imaging Workflows
Machine learning tools for vessel segmentation, automated plaque burden quantification, and risk stratification are already being introduced into clinical practice. The U.S. Food and Drug Administration (FDA) maintains a growing list of AI-enabled imaging devices authorized for vascular and cardiovascular applications, and prospective validation studies are underway to assess their impact on diagnostic throughput and prognostic accuracy. These developments indicate that AI has moved beyond proof-of-concept to regulated clinical deployment in imaging-heavy fields relevant to vascular disease [136,137]. As these tools move from development to deployment, stringent external validation across institutions, imaging platforms, and patient demographics, along with continuous post-implementation performance monitoring, will be essential to ensure safety and mitigate bias.
8.3. Regulatory Science and Harmonization
Successful translation of these platforms requires alignment with evolving regulatory frameworks. The FDA has outlined a lifecycle approach for software as a medical device (SaMD), emphasizing good machine learning (GML) practices, predetermined change control plans, and post-market monitoring. The European Medicines Agency (EMA) has issued a work plan aligned with the forthcoming EU AI Act, emphasizing risk-based oversight, transparency, and traceability when AI informs patient care [138]. Parallel efforts by the U.S. National Institutes of Health (NIH), such as the Bridge2AI program, and international initiatives like the Human Cell Atlas provide community standards, ML-ready datasets, and metadata conventions that strengthen reproducibility and support regulatory acceptance [139]. Regulatory agencies increasingly emphasize not only analytical performance but also clinical utility, transparency of algorithms, and robust mechanisms for updating and revalidating models over time, particularly for adaptive AI-based devices.
8.4. Implications for Vascular Research
Several principles are emerging for investigators and developers. First, intended use and risk classification should be defined early, as regulatory expectations differ for decision-support versus interventional guidance. Second, both analytical validity (e.g., reproducibility, sensitivity, robustness to batch effects) and clinical utility (e.g., correlation with outcomes such as revascularization or event-free survival) should be demonstrated in multicenter studies. Third, continuous performance monitoring and harmonized metadata capture are increasingly non-negotiable requirements. By incorporating these considerations into experimental design, vascular technologies can advance beyond proof-of-concept to become validated tools with real clinical impact [140].
8.5. Emerging Hotspots in Vascular Disease Research
Several emerging research domains are poised to reshape how VDs are studied and managed. Multiscale modeling frameworks that couple hemodynamics, wall biomechanics, and biologically informed remodeling rules offer the potential to simulate disease trajectories and virtual interventions in silico [24]. Digital twins extend this concept to patient-specific virtual replicas that integrate anatomy, physiology, and, in some implementations, molecular or lifestyle data [133]. In parallel, high-dimensional proteomics and metabolomics are expanding the catalog of circulating and tissue-derived biomarkers beyond what can be captured by transcriptomics alone, while advances in nanotechnology and smart biomaterials are enabling increasingly sophisticated platforms for targeted drug delivery, molecular imaging, and local biomechanical modulation [141]. Epitranscriptomic profiling adds an additional regulatory layer by revealing how RNA modifications modulate vascular cell responses to inflammatory, mechanical, and metabolic cues [142].
Increasingly, these domains are being combined in integrated frameworks. Spatial omics and advanced imaging can be jointly analyzed to create multi-modal atlases that link microscopic cell states and molecular programs to macroscopic lesion phenotypes [143]. Multi-omics discovery pipelines are being coupled with organ-on-chip and organoid platforms to functionally test candidate pathways under physiologically relevant flow and cellular configurations [144]. Continuous physiological monitoring from wearables or implantable sensors is being explored as an input for digital twins and predictive models, enabling dynamic, patient-specific risk assessment and treatment adaptation [145]. These emerging combinations are largely at an exploratory or proof-of-concept stage and will require coordinated, multidisciplinary efforts to achieve clinical impact.
8.6. Proteomics and Metabolomics: Expanding Beyond Transcriptomics
Proteomics and metabolomics offer complementary perspectives to transcriptomics by directly measuring the abundance and modifications of proteins and metabolites, the functional molecules driving vascular physiology. Advances in high-resolution mass spectrometry (MS), tandem MS (LC–MS/MS), and targeted assays (ELISA, MRM panels) now enable systematic profiling of circulating proteins and metabolites in vascular disease cohorts [146,147].
Proteomic studies in vascular disease typically analyze plasma, serum, or tissue samples to identify dysregulated proteins associated with endothelial dysfunction, inflammation, and extracellular matrix remodeling [148]. For example, proteomic profiling has detected upregulation of osteogenic proteins (RUNX2, osteopontin) in vascular smooth muscle cells undergoing calcification. Metabolomics, by contrast, captures systemic metabolic shifts linked to vascular disease risk, such as elevated trimethylamine-N-oxide (TMAO) levels related to atherosclerosis or altered amino acid metabolism in hypertension. Integrating proteomics, metabolomics, and transcriptomics enables multi-omics network construction, revealing mechanistic pathways and identifying candidate biomarkers for risk stratification.
Several limitations hinder clinical translation. Proteomic data may be biased by sample handling, the dynamic protein range (where abundant proteins mask rare events), and inter-laboratory variability [149]. Metabolomic profiles are influenced by diet, microbiome, and medication, which complicates reproducibility [150]. Standardization of assay protocols, normalization strategies, and reference ranges is still in development. Large, prospective, multi-ethnic cohorts are needed to establish robust biomarker panels that provide predictive value beyond traditional risk factors.
To date, most proteomic and metabolomic signatures associated with vascular disease remain at the discovery or early validation stage, with limited multi-center replication and sparse evidence for incremental clinical value beyond established risk factors.
8.7. Nanotechnology and Smart Biomaterials
Nanotechnology has rapidly emerged as a tool for targeted drug delivery, vascular imaging, and tissue engineering. Liposomes, polymeric nanoparticles, and inorganic nanostructures can be functionalized with ligands to target diseased vascular sites, such as inflamed endothelium or lipid-rich plaques [151,152]. Innovative biomaterials, including bioresorbable scaffolds and stimuli-responsive stents, represent another frontier by enabling drug release or responding to local hemodynamic cues.
Nanoparticles exploit the enhanced permeability and retention (EPR) effect or ligand–receptor interactions, for example, by targeting vascular cell adhesion molecule-1 on inflamed endothelium, to localize selectively within vascular lesions [153]. They can deliver anti-inflammatory agents, siRNA, or imaging contrast agents. Smart stents and hydrogels can be engineered to release drugs in response to environmental triggers such as pH, reactive oxygen species, or shear stress [154,155]. The integration of these devices with sensors and wireless monitoring systems enables AI-guided feedback loops for vascular implants.
The main limitations involve safety, scalability, and regulatory hurdles. Nanoparticles can accumulate in non-target organs, such as the liver and spleen, which raises toxicity concerns. Long-term biocompatibility and the degradation products of novel biomaterials require rigorous evaluation. Manufacturing reproducibility at a clinical scale also remains a barrier, as does navigating the regulatory classification of combination products (drug + device + diagnostic) [156]. Despite promising preclinical data, these challenges have slowed clinical adoption. Although several nanotechnology-based formulations are clinically approved in oncology and other fields, vascular-specific nanotherapeutics and imaging agents are largely preclinical, and issues of long-term safety, biodistribution, manufacturing scalability, and regulatory classification remain major obstacles.
8.8. Epitranscriptomics: RNA Modifications as Regulators of Vascular Biology
Epitranscriptomics refers to chemical modifications of RNA molecules, such as N6-methyladenosine (m6A), pseudouridine, or 5-methylcytosine, that alter RNA stability, splicing, translation, or localization without changing the underlying sequence [157,158]. These modifications are mapped using high-throughput sequencing methods such as MeRIP-seq (m6A RNA immunoprecipitation sequencing), miCLIP (m6A crosslinking immunoprecipitation), or direct RNA sequencing with nanopore technologies [159].
m6A is the most abundant internal mRNA modification in eukaryotes and is dynamically regulated by “writers” (methyltransferases such as METTL3), “erasers” (demethylases like FTO), and “readers” (YTH domain proteins) [160,161]. In vascular biology, m6A influences endothelial cell proliferation, smooth muscle phenotypic switching, and inflammatory responses. For example, altered m6A modification can destabilize mRNAs encoding protective endothelial genes, exacerbating vascular injury [162]. Epitranscriptomic regulation thus represents a finely tuned mechanism that links environmental stressors to transcriptomic remodeling in vascular disease.
This field is nascent, with few studies directly linking RNA modifications to clinical vascular outcomes. Technical challenges include antibody specificity in immunoprecipitation assays, low resolution in mapping modifications, and variability across sequencing platforms [163,164]. Additionally, the causal role of RNA modifications, rather than merely correlative associations, remains to be clarified. Pharmacological targeting of epitranscriptomic regulators is an emerging, yet untested, strategy in cardiovascular disease.
8.9. Strengths and Limitations of These Assays
Strengths of single-cell and spatial omics include single-cell resolution, ability to uncover rare cell states and spatial niches, and power to generate mechanistic hypotheses about cell–cell communication. Limitations include high cost, complex workflows, sensitivity to tissue quality, batch effects, modest cohort sizes, and the fact that most derived biomarkers remain research-grade [165].
Imaging innovations include advanced modalities such as super-resolution microscopy, intravital imaging, photoacoustic imaging, and super-resolution ultrasound, which provide detailed structural and functional information beyond conventional imaging. However, trade-offs between resolution and penetration depth, technical complexity, and the need for specialized equipment and expertise limit their availability and standardization [166].
Table 4 summarizes the limitations of imaging modalities, along with representative depth and spatial resolution, and their current applications.
The above table compares the principal imaging modalities discussed in Section 4, focusing on their penetration depth, temporal resolution, and limitations in vascular disease imaging. It also summarizes the current preclinical and clinical readiness for each technique.
The microfluidic and organ-on-a-chip systems enable controlled manipulation of flow, shear stress, and cellular composition, thereby improving mechanistic modeling compared with static cultures. Their limitations include variability in device design, difficulty capturing full vascular heterogeneity and systemic interactions, long-term stability issues, and relatively low throughput [173].
CRISPR/Cas9 and optogenetic methods provide precise perturbations for the mechanistic dissection of gene function and cellular behavior. Concerns about off-target effects, delivery challenges, immunogenicity, and ethical and regulatory considerations constrain their clinical translation [174].
Machine learning, generative AI, multiscale modeling, and digital twins can integrate heterogeneous datasets, simulate complex vascular dynamics, and generate predictions at the patient level. Key limitations include data requirements, risk of bias, limited transparency and interpretability in some models, and uncertain performance when applied outside the training distribution [175]. To connect these emerging technologies to real-world clinical needs, Table 5 summarizes major vascular diseases, associated risk factors, diagnostic approaches, and current treatment strategies.
An overview of the current translational positioning of each major technology, ranging from discovery-stage mechanistic tools to emerging early clinical applications in vascular disease, is provided in Table 6.
8.10. Strength of Evidence and Approach to Study Quality Assessment
The evidence base supporting emerging vascular imaging technologies is heterogeneous, with considerable variation in study design, sample size, technical maturity, and the level of independent validation [176]. Several modalities included in this review, such as photoacoustic imaging, super-resolution ultrasound, optogenetic vascular modulation, and microfluidic vascular models, are represented predominantly by feasibility studies or isolated reports conducted in limited preclinical settings [177]. In these areas, conclusions remain preliminary because protocols, acquisition parameters, and analytical workflows are not yet standardized across laboratories. Small datasets, single-center implementations, and unreplicated experimental configurations also contribute to uncertainty, making it difficult to determine the reproducibility and generalizability of reported effects [178].
Evidence is also inconsistent in domains where studies employ different imaging platforms, contrast agents, or biological models. Discrepancies in microvascular perfusion measurements, plaque-level characterization metrics, or endothelial signaling readouts often arise from variations in hardware sensitivity, reconstruction algorithms, or biological preparation rather than from true biological divergence [80]. We emphasized the need for larger, harmonized studies to clarify whether these observations reflect genuine physiological mechanisms or technology-dependent artifacts.
To assess the quality of each study, we examined multiple aspects, including the robustness of the experimental design and the clarity of the imaging methodology. We also considered whether the approach was validated against recognized reference standards. Studies that met these criteria and demonstrated consistent effects across multiple models or cohorts were given greater interpretive weight. Conversely, results derived from preliminary or single-study evidence were contextualized as early signals rather than established trends. This approach allowed us to distinguish robust, convergent findings from those that remain provisional and to identify areas where methodological refinement, multicenter validation, and standardized reporting would substantially strengthen the evidence base. Several advanced imaging modalities are now used to investigate vascular structure and function, yet each technology carries characteristic limitations that can influence data quality, interpretation, and reproducibility. Reports from preclinical and clinical studies describe depth-related signal loss, motion-sensitive acquisition artifacts, inconsistent hardware performance, and variability introduced by device design or analytical workflows [80]. These issues are particularly relevant in microvascular imaging, endothelial dynamics, plaque characterization, and vascular-on-chip platforms, where measurements depend heavily on spatial resolution, temporal stability, and standardized acquisition protocols [179]. To provide a clear overview, Table 7 below summarizes documented failure modes and reproducibility concerns for commonly used vascular imaging approaches, along with their specific applications and supporting primary references.
9. Conclusions and Future Prospects
VDs are driven by complex interactions among endothelial cells, vascular smooth muscle cells, fibroblasts, immune cells, and circulating factors within a dynamic hemodynamic environment. Emerging technologies reviewed here, including single-cell and spatial omics, advanced imaging, microfluidic and organ-on-chip systems, genetic perturbation tools, and AI-based computational frameworks, have substantially deepened our understanding of these processes. They have revealed previously unappreciated cellular heterogeneity, transitional cell states, and spatially confined microenvironments that contribute to atherosclerosis, aneurysm formation, pulmonary vascular remodeling, and microvascular dysfunction.
Some of these technologies are beginning to influence clinical practice. AI-supported imaging tools for vessel segmentation, plaque characterization, and risk prediction, as well as early photoacoustic imaging studies, are moving toward integration in vascular diagnostics. In contrast, most multi-omics platforms, microfluidic and organ-on-chip systems, CRISPR- and optogenetics-based perturbations, and digital twins remain in the preclinical or exploratory stages, where they primarily serve as engines for mechanistic discovery and hypothesis generation. Recognizing these different maturity levels is essential to set realistic expectations and prioritize translational investments.
Major bottlenecks in translation include technical complexity, cost, limited standardization, and the lack of large, diverse, multi-center datasets. For omics and imaging assays, reproducibility, protocol harmonization, robust quality control, and demonstration of incremental clinical utility over existing standards are critical. For organ-on-chip and genetic tools, issues of reproducibility, long-term stability, delivery, and safety need to be addressed. For AI and multiscale models, transparent reporting, external validation, fairness across populations, and explicit characterization of failure modes are essential prerequisites for regulatory approval and clinical trust.
Future efforts should prioritize the development of integrated pipelines that link discovery to application: multi-omics and spatial profiling to identify candidate mechanisms; AI and network analysis to prioritize and model these mechanisms; physiologically relevant microfluidic and organ-on-chip systems to test interventions; and multiscale models and digital twins to translate insights to patient-specific prediction and decision support. Multi-center consortia, shared reference datasets, and close collaboration between clinicians, biologists, engineers, and regulatory agencies will be indispensable. If these challenges are addressed, the technologies described here have the potential to enable more precise diagnostics, targeted therapies, and ultimately, personalized vascular medicine.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Cardiovascular Diseases 2025 Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1(accessed on 12 November 2025)
- 2Pahwa R. Jialal I. Atherosclerosis Rutherford’s Vascular Surgery and Endovascular Therapy 10th ed.Stat Pearls Publishing St. Petersburg, FL, USA 20231–24150.e 4
- 3Ramanathan A.S. Senguttuvan P. Prakash V. Vengadesan A. Padmaraj R. Budding adult hypertensives with modifiable risk factors: Catch them young J. Fam. Community Med.201623384210.4103/2230-8229.172232 PMC 474520026929728 · doi ↗ · pubmed ↗
- 4Shah H. Altaf A. Salahuddin M. Jan M.U. Khan A. Cardiovascular risk factors of hypertension, smoking and obesity: Emerging concerns among Pathan and Persian young adults?Med. J. Islam. Repub. Iran 20183212910.14196/mjiri.32.12930815424 PMC 6387808 · doi ↗ · pubmed ↗
- 5Tsuchiya T. Hirano Y. Miyawaki S. Koizumi S. Ogawa S. Torazawa S. Hongo H. Ono H. Saito N. Outcomes and Complications of Endovascular Treatment in Patients with Moyamoya Disease: A Systematic Review World Neurosurg.202519612378310.1016/j.wneu.2025.12378339947318 · doi ↗ · pubmed ↗
- 6Christie A. Roditi G. Vascular imaging: The evolving role of the multidisciplinary team meeting in peripheral vascular disease Semin. Interv. Radiol.20143132032910.1055/s-0034-139396825435657 PMC 4232423 · doi ↗ · pubmed ↗
- 7Kim K.J. Li B. Winer J. Armanini M. Gillett N. Phillips H.S. Ferrara N. Inhibition of vascular endothelial growth factor-induced angiogenesis suppresses tumour growth in vivo Nature 199336284184410.1038/362841 a 07683111 · doi ↗ · pubmed ↗
- 8Laal M. Innovation Process in Medical Imaging Procedia-Soc. Behav. Sci.201381606410.1016/j.sbspro.2013.06.388 · doi ↗