Do Akkermansia mutants underlie the global metabolic disease epidemic?
Heenam Stanley Kim

TL;DR
Mutations in Akkermansia muciniphila caused by antibiotics may be linked to rising metabolic diseases worldwide.
Contribution
Identifies antibiotic-induced Akkermansia mutants as a potential driver of metabolic disease epidemics.
Findings
Antibiotic-induced Akkermansia mutants survive better but harm host interactions.
These mutants are widespread and may contribute to metabolic disorders.
They could serve as biomarkers and therapeutic targets if validated in global studies.
Abstract
Antibiotic-induced mutations in Akkermansia muciniphila promote bacterial survival while compromising beneficial host interactions, revealing a potential new link between antibiotic-driven microbiome disruption and metabolic disease. The widespread presence of these mutants suggests that they may contribute to the increasing prevalence of metabolic disorders. If validated in diverse global human cohort studies, these mutants could serve as biomarkers of disease susceptibility and as targets for therapeutic intervention.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
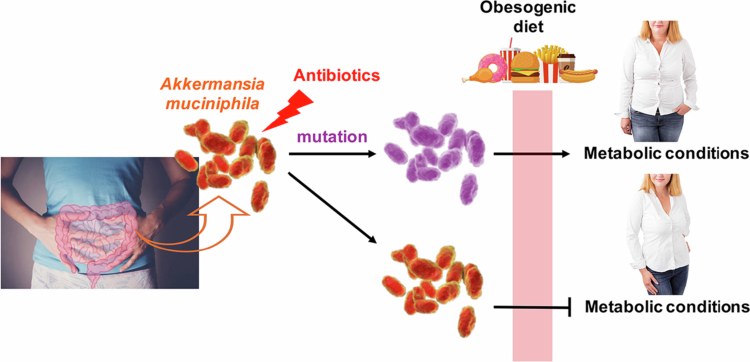 Figure 1
Figure 1- —National Research Foundation of Korea10.13039/501100003725
- —National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGut microbiota and health · Microbial Community Ecology and Physiology · Antibiotic Resistance in Bacteria
The global rise in chronic diseases in recent decades has been linked to alterations in the gut microbiome.1 Industrialization and urbanization are believed to have profoundly and cumulatively reshaped the human microbiota across generations through factors such as dietary shifts—especially reduced fiber intake—enhanced hygiene practices, increased rates of Cesarean delivery, and widespread antibiotic use.1^,^2 Although antibiotic-induced disruption is recognized as a major contributing factor,1^,^3^,^4 the precise nature of this damage and its connection to chronic disease remains poorly understood. Several fundamental questions persist: How does antibiotic-induced damage linger for years? What governs microbiome recovery after disruption? And, in a related context, how does low-dose antibiotic use in livestock promote weight gain? These unresolved issues suggest that taxonomic shifts alone cannot explain the full extent of antibiotic damage, underscoring the need to investigate physiological changes within the gut microbiota, particularly in key bacterial species that exert disproportionate effects on host health.
A recent study by Han et al. provides important insights. They demonstrated that Akkermansia muciniphila, a core member of the human gut microbiota, can acquire survival-enhancing mutations in response to antibiotic exposure—while simultaneously losing intrinsic host-beneficial functions.5 In a mouse model of metabolic conditions, wild-type Akkermansia strains—including the reference strain BAA-835 (MucT) and strain HMI that can be classified as Akkermansia massiliensis under a new classification system)—protected against diet-induced metabolic abnormalities, whereas mutant strains did not.5 This finding reveals a missing link between antibiotic-induced microbiota alterations and host health, with potential relevance to humans given the widespread and repeated use of antibiotics since World War II (Figure 1).
Epidemiological evidence suggests that maternal antibiotic exposure before or during pregnancy, as well as antibiotic exposure in early childhood, can have lasting effects on human health, including an increased risk of early-onset obesity in infants and children.6‐8 Such persistence may be explained by the low reversion rates of antibiotic-induced mutations.9^,^10 Consistent with this view, mutations in A. muciniphila appear stable and transmissible across human populations, as reflected by their widespread global prevalence.5 Notably, antibiotic exposure is not the only factor causing long-lasting effects; Cesarean section birth has also been associated with an increased risk of chronic diseases such as asthma and obesity later in life.11^,^12 However, because Cesarean delivery is invariably accompanied by antibiotics, it remains unclear whether the observed effects are due to the delivery mode itself or to the antibiotics. It is therefore highly plausible that these mutants have contributed not only to the long-term consequences of antibiotic-induced damage but also to the global rise in metabolic diseases, including obesity, type II diabetes, and nonalcoholic fatty liver disease. Nonetheless, confirming these hypotheses will require studies across diverse human cohorts worldwide.
Within this context, one factor underlying microbiome recovery after disruption may be the gradual replacement of mutant strains with their wild-type counterparts. Moreover, the results from the mouse model shed light on the long-standing puzzle of how low-dose antibiotics promote weight gain in livestock13—by favoring the persistence of functionally impaired strains.
Mechanistically, the primary target of mutation in A. muciniphila following exposure to penicillins—the most widely prescribed class of antibiotics worldwide14—was the de novo purine biosynthesis pathway. Frequent mutations were observed in purF, a key gene in this pathway.5 Notably, PurF is also a target of the stringent response alarmone (p)ppGpp, which inhibits its activity and blocks purine synthesis, as observed in Escherichia coli.15^,^16 Given the central role of the stringent response in bacterial antibiotic tolerance,16 its activation through purine synthesis inhibition may represent a molecular mechanism underlying acquired antibiotic insusceptibility in A. muciniphila. However, the mechanisms underlying the concomitant loss of host-beneficial functions remain unclear and are likely multifactorial, involving both broader microbiota interactions and host responses. In particular, potential effects on gut barrier function or glucagon-like peptide‑1 (GLP‑1) secretion—which are normally positively regulated by A. muciniphila and contribute to improved metabolic health17—warrant careful investigation.
The risks associated with antibiotic exposure extend beyond metabolic disorders.6 Epidemiological studies link antibiotic use to heightened susceptibility to allergic, autoimmune, and psychiatric conditions, as well as colon cancer—all associated with microbiota disruption and impaired intestinal barrier function.6 Intriguingly, A. muciniphila has been implicated in protecting against many of these same conditions.18 This suggests that mutant A. muciniphila strains may also influence disease outcomes beyond metabolic disorders, highlighting their broader relevance for human health.
This emerging mechanism—where antibiotics influence host health by selecting for functionally impaired mutants of essential gut microbes such as A. muciniphila—has far-reaching implications for understanding chronic disease susceptibility. If validated in human populations, these findings could open new avenues for diagnostic and therapeutic strategies against metabolic conditions and related disorders, particularly in the context of personalized medicine. Beyond A. muciniphila, future research should determine whether similar antibiotic-driven mutations in other keystone microbes, such as Faecalibacterium prausnitzii and Bacteroides thetaiotaomicron, likewise impair beneficial functions and influence human health.
Ultimately, this study demonstrates that non-taxonomic changes in the microbiota—namely, functional mutations—can exert substantial effects on host physiology. A deeper understanding of the so-called ‘altered gut microbiome’ will bring us closer to unraveling the mechanisms of chronic disease and, ultimately, to developing more effective therapeutic interventions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blaser MJ. The past and future biology of the human microbiome in an age of extinctions. Cell. 2018;172:1173–1177. doi: 10.1016/j.cell.2018.02.040.29522739 · doi ↗ · pubmed ↗
- 2Bello MGD, Knight R, Gilbert JA, Blaser MJ. Preserving microbial diversity. Sci. 2018;362:33–34. doi: 10.1126/science.aau 8816. · doi ↗
- 3Becattini S, Taur Y, Pamer EG. Antibiotic-induced changes in the intestinal microbiota and disease. Trends Mol Med. 2016;22:458–478. doi: 10.1016/j.molmed.2016.04.003.27178527 PMC 4885777 · doi ↗ · pubmed ↗
- 4Ramirez J, Guarner F, Bustos Fernandez L, Maruy A, Sdepanian VL, Cohen H. Antibiotics as major disruptors of gut microbiota. Front Cell Infect Microbiol. 2020;10:572912. doi: 10.3389/fcimb.2020.572912.33330122 PMC 7732679 · doi ↗ · pubmed ↗
- 5Han Y, Teng TM, Han J, Kim HS. Antibiotic-associated changes in Akkermansia muciniphila alter its effects on host metabolic health. Microbiome. 2025;13:48. doi: 10.1186/s 40168-024-02023-4.39920776 PMC 11804010 · doi ↗ · pubmed ↗
- 6Queen J, Zhang J, Sears CL. Oral antibiotic use and chronic disease: long-term health impact beyond antimicrobial resistance and Clostridioides difficile. Gut Microbes. 2020;11:1092–1103. doi: 10.1080/19490976.2019.1706425.32037950 PMC 7524332 · doi ↗ · pubmed ↗
- 7Ajslev TA, Andersen CS, Gamborg M, Sørensen TI, Jess T. Childhood overweight after establishment of the gut microbiota: the role of delivery mode, pre-pregnancy weight and early administration of antibiotics. Int J Obes (Lond). 2011;35:522–529. doi: 10.1038/ijo.2011.27.21386800 · doi ↗ · pubmed ↗
- 8Mor A, Antonsen S, Kahlert J, Holsteen V, Jørgensen S, Holm-Pedersen J, Sørensen HT, Pedersen O, Ehrenstein V. Prenatal exposure to systemic antibacterials and overweight and obesity in Danish schoolchildren: a prevalence study. Int J Obes (Lond). 2015;39:1450–1455. doi: 10.1038/ijo.2015.129.26178293 · doi ↗ · pubmed ↗