Age and Clinical Outcomes of Immune Checkpoint Inhibitor Toxicities in Portugal: A Decade of Pharmacovigilance
Tiago Pina-Cabral, José Pereira, João Paulo-Fernandes, Márcia Silva, Mário Fontes-Sousa, Mariana Anacleto, Soraia Lobo-Martins, Ana Mirco, Helena Miranda, Ana Martins, Patrícia Cavaco

TL;DR
This study uses a decade of Portuguese data to show that while older adults don't report more serious immune checkpoint inhibitor side effects, they face higher fatality rates when severe toxicity occurs.
Contribution
The study provides real-world evidence on age-related differences in ICI toxicity outcomes and patterns using national pharmacovigilance data.
Findings
Serious adverse drug reactions were equally reported in older and younger adults, but older adults had higher fatality rates.
Toxicity patterns differed by age, with older adults more likely to experience nervous and immune system events.
Combination therapy increased the likelihood of serious adverse reactions, but not fatal outcomes.
Abstract
Immune checkpoint inhibitors (ICIs) are widely used across many cancer types, yet their real-world safety in older adults is not well studied. Using a decade of national pharmacovigilance data from Portugal, we examined adverse drug reactions (ADRs) reported in patients treated with ICIs, focusing on whether age impacts the seriousness or pattern of toxicities. We found that serious ADRs were not more frequently reported in older adults than younger adults; however, when severe toxicity occurred, fatal outcomes were more common in patients aged 70 years or older. The types of organ systems affected also differed by age, with nervous and immune system events more frequently reported in older adults and hepatic or hematologic events more commonly in younger patients. Treatment regimen, particularly combination therapy, also influenced the likelihood of being classified as serious. These…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
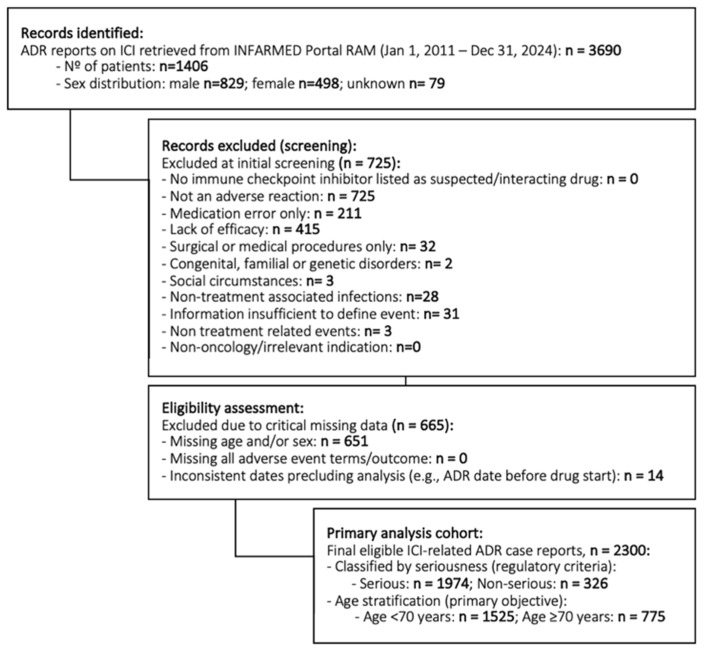 Figure 1
Figure 1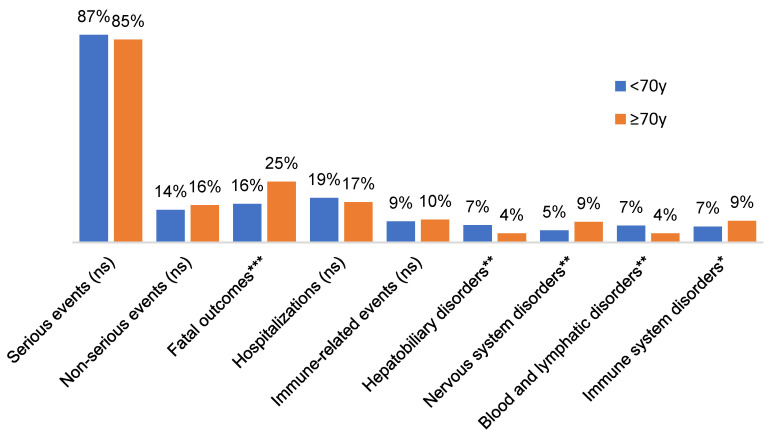 Figure 2
Figure 2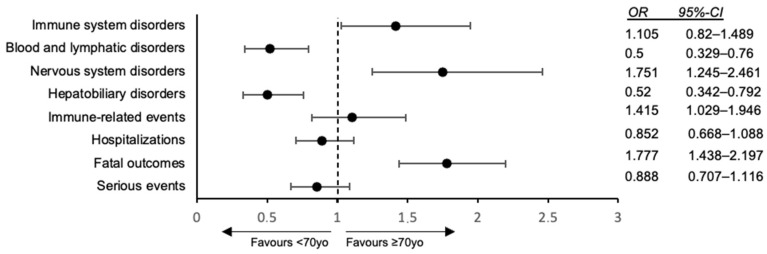 Figure 3
Figure 3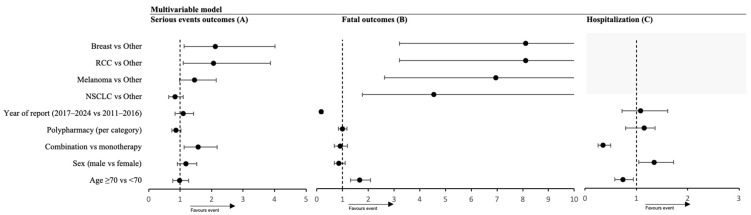 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Pharmacovigilance and Adverse Drug Reactions · CAR-T cell therapy research
1. Introduction
The advent of immune checkpoint inhibitors (ICIs) has redefined the therapeutic landscape of oncology, yielding survival benefits across diverse malignancies [1,2,3,4,5]. By targeting key regulatory pathways, such as cytotoxic T-lymphocyte–associated antigen 4 (CTLA-4), programmed death 1 (PD-1), programmed death ligand 1 (PD-L1), and more recently, lymphocyte-activation gene 3 (LAG-3), ICIs enhance the intrinsic ability of the immune system to recognize and eliminate malignant cells. They have been approved for use in both (neo)adjuvant and metastatic settings, offering unprecedented prospects for patients with historically poor prognoses. Since the approval of ipilimumab (anti-CTLA-4) in Europe in 2011, the therapeutic arsenal has steadily expanded. Notably, subsequent approvals of nivolumab and pembrolizumab (anti-PD-1) in 2015, atezolizumab and avelumab (anti-PD-L1) in 2017, durvalumab (anti-PD-L1) in 2018, and more recently, cemiplimab (anti-PD-1) along with novel combination regimens such as nivolumab/relatlimab (anti-PD-1/LAG-3) and durvalumab/tremelimumab (anti-PD-L1/CTLA-4), have markedly broadened treatment options.
Unlike traditional cytotoxic therapies, ICIs unleash the full potential of the immune system, offering substantial therapeutic benefit against malignancies. However, this enhanced immune activity may inadvertently result in non-tumor immune-mediated damage, producing a unique spectrum of toxicities termed immune-related adverse events (irAEs) that can affect virtually any organ system [6,7,8,9,10,11,12,13]. Of these, the most commonly affected systems include the skin, lungs, colon, and endocrine glands [4,9,13,14,15]. The clinical spectrum of irAEs ranges from mild dermatologic eruptions or thyroid dysfunction to severe and potentially fatal conditions, such as pneumonitis, myocarditis, colitis, and neuroinflammatory syndromes. In clinical trials, grade 3 or higher, irAEs occur in approximately 15–20% of patients treated with anti-PD-1/PD-L1 monotherapy, whereas this rate escalates to over 50% within combination regimens involving anti-CTLA-4 [16,17]. Early recognition and prompt management, typically with corticosteroids or other immunosuppressive agents, are critical for mitigating morbidity and mortality, although these interventions can potentially compromise antitumor efficacy and influence long-term outcomes [15,18]. Beyond direct toxicities, emerging data reveal that concomitant medications, particularly antibiotics, may disrupt the gut microbiome and thereby diminish ICI efficacy [19]. Electrolyte imbalances, notably among lung cancer patients, further complicate clinical management, underscoring the necessity for proactive monitoring during immunotherapy.
Despite the robustness of clinical trial data, translating these findings into routine clinical practice remains challenging, largely due to disparities in patient demographics and comorbidities. Real-world data in ICI toxicity are relatively limited, since clinical trial populations are often highly selective and may under-represent older adults and those with comorbidities. Notably, patients over 80 years of age comprise approximately 16% of cancer cases but only constitute approximately less than 4% of trial participants [20,21,22], raising concerns regarding the generalization of trial-derived safety and efficacy data to real-world geriatric populations. Despite the high burden of comorbidity and polypharmacy in older adults, the more favorable safety profile of ICIs compared with cytotoxic chemotherapy has enabled their increasing adoption in this age group [20,23,24,25]. On the other hand, immunosenescence, the age-related remodeling of the immune system, does not simply attenuate immune responses but can paradoxically promote dysregulated immunity. Age-associated thymic involution, expansion of autoreactive memory T-cell clones, and chronic low-grade inflammation (“inflammaging”) may increase susceptibility to certain immune-mediated toxicities rather than protect against them [26,27,28]. In this context, the frailty, multimorbidity and reduced physiological reserve characteristic of older adults can further amplify the clinical impact of irAEs, contributing to the higher case-fatality observed in this population [26,27]. The existing literature remains inconclusive: while some studies have found no significant difference in overall irAE frequency between older and younger adults, whereas others, including pharmacovigilance analyses, suggest older patients may have higher reporting rates of specific irAEs [6,22,23]. A large cohort study of 19,177 patients aged ≥ 75 years reported no significant difference in irAEs incidence compared to younger cohorts, a finding corroborated in an analysis of 928 patients aged ≥80 years, where 41.3% experienced at least one irAE with consistent patterns across age groups [25]. Nonetheless, geriatric syndromes such as frailty, polypharmacy, and multimorbidity have emerged as critical modifiers of risk, with frail patients demonstrating heightened susceptibility to irAEs, thus emphasizing the need for comprehensive geriatric assessments to inform clinical decision-making [25,29,30]. The toxicity profile also seems to shift with age; for example, some studies indicate that endocrine irAEs (such as thyroiditis/hypophysitis) appear more commonly in younger patients, while dermatologic irAEs occur more frequently in patients ≥ 75 years old [31]. Additionally, elderly patients might have higher mortality rates and longer hospital stays when severe irAEs occur [13,14,15,22]. It is largely unknown whether elderly patients experience different incidences or patterns of irAEs compared to younger patients. Given these uncertainties, real-world data focusing on older adults are crucial to better characterize toxicity risks and inform clinical decision-making in this growing population.
Recognizing the limitations of clinical trial data, pharmacovigilance systems capture real-world safety profiles in heterogeneous populations. In Portugal, adverse drug reactions are reported to the National Pharmacovigilance System (Portal RAM), which collects spontaneous notifications from healthcare professionals and patients. These data enable the early detection of safety signals, characterization of toxicity in underrepresented groups, and identification of risk factors for severe irAEs, particularly in older or comorbid patients. Despite international evidence supporting real-world analyses, no systematic evaluation of ICI-related events has been conducted in Portugal to date.
The Immunotherapy Monitoring in Portugal: Age and Clinical Toxicity Profiling (The IMPACT Study) was designed to assess the frequency, seriousness, and organ-specific distribution of irAEs reported to INFARMED, with an emphasis on age and clinical determinants. By including all European Commission authorized ICIs, the IMPACT Study aimed not only to supplement evidence from clinical trials but also to promote safer, more individualized use of immunotherapy among vulnerable patient populations in routine practice.
2. Materials and Methods
This study was designed as a national, retrospective observational cohort of ICI reported adverse events, utilizing Portugal’s pharmacovigilance database. All spontaneous adverse drug reaction (ADR) reports submitted to INFARMED’s “Portal RAM” system from 1 January 2011, through 31 December 2024, were screened. In Portugal, ADRs are reported to the National Pharmacovigilance System by healthcare professionals, pharmaceutical companies, and patients/caregivers, through the online Portal RAM. Reports are anonymized by INFARMED before release for research purposes, ensuring that no directly identifiable information is accessible to investigators. The system does not retain a variable indicating whether a notification originated from a clinical study or routine care; therefore, all ICSRs in this dataset were operationally considered spontaneous reports, consistent with the absence of mandatory prospective reporting in Portal RAM during the study period. To minimize duplication, INFARMED applies internal quality control procedures before database extraction; however, because the dataset does not include patient identifiers beyond age and sex, we could not independently verify duplicate submissions. Potential clustering due to multiple ADRs per individual was addressed analytically by conducting sensitivity analyses restricted to the first ADR per patient, which yielded results concordant with the primary case-level analyses. Reports were eligible if they involved at least one EMA-approved ICI, such as anti-PD-1 (e.g., nivolumab, pembrolizumab and cemiplimab), anti-PD-L1 (atezolizumab, avelumab and durvalumab), anti-CTLA-4 (ipilimumab and tremelimumab), or other agents approved in Europe. Each individual case safety report (ICSR) corresponded to a single patient who experienced one or more reported ADR associated with ICI treatment. We excluded entries that did not represent a safety related adverse reaction (e.g., reports of medication error, lack of efficacy, or unrelated medical issues) and those with critical missing data. After applying the inclusion criteria, a total of 2300 eligible ICI-related ADR cases were identified, corresponding to 925 unique patients, as some individuals contributed more than one ADR report.
2.1. Data Sources and Variables
For each ADR report, we extracted patient demographics, such as age at ADR, sex, cancer type/indication, ICI drug(s) administered, and concomitant medications. Age was treated as a continuous variable (for summary statistics) and dichotomized into two groups (<70 vs. ≥70 years) for the primary subgroup analyses. Tumor types were categorized into major groups (non-small cell lung cancer (NSCLC), melanoma, renal cell carcinoma, breast cancer, and “other” malignancies) based on the indications listed. The treatment regimen was classified as monotherapy, a single ICI agent, or combination therapy, defined as an ICI administered in combination with at least one other anticancer agent (such as another ICI or chemotherapy). Additionally, we specifically flagged CTLA-4-containing regimens to examine their risk profiles. The number of concomitant medications at the time of the ADR was counted and stratified into three categories: ≤2, 3–5, and >5 concurrent noncancer treatment drugs. Each ADR was coded using MedDRA terminology. We collated the involved primary System Organ Classes (SOCs) to characterize the affected organ systems. Events were further labeled as irAEs when the notifier indicated an immune-mediated mechanism. The ‘immune-related’ label reflects the notifier’s clinical judgement rather than an adjudicated or algorithm-based irAE classification; all ADRs were first coded as specific MedDRA Preferred Terms and then mapped to System Organ Classes, but a given clinical entity (e.g., thyroiditis, hepatitis, colitis) may or may not have been explicitly designated as immune-mediated by the reporter, leading to under-capture of irAEs within this variable. The outcomes of each ADR case were recorded in terms of seriousness and specific serious outcome criteria. Seriousness was defined according to standard pharmacovigilance criteria (death, life-threatening event, hospitalization, disability, or other medically important condition). For the primary endpoint of this study, we operationally defined severe irAEs as any ADR meeting the serious criteria, focusing on cases involving hospitalization, life-threatening conditions, or fatal outcomes. Accordingly, fatal outcomes and hospitalizations were analyzed as key subcategories of seriousness of AE. Reporter characteristics (healthcare professional vs. patient) and timing variables were also collected. The calendar year of ICI start and of ADR occurrence were noted, and when available, the time-to-onset of the toxicity was calculated (interval from ICI initiation to ADR onset). All data were de-identified; each case was indexed only by a coded ID with no personal identifiers, in compliance with national data protection regulations. The analytic unit was the ADR case (i.e., a unique report fulfilling the inclusion criteria). Multiple ADRs can originate from the same patient. For transparency, we conducted: (i) a primary case-level analysis; and (ii) a sensitivity analysis restricted to the first eligible ADR per patient (de-duplicated patient-level dataset). Analyses were performed at the case level (ADR reports). Because some patients contributed >1 ADR, we performed a prespecified sensitivity analysis restricted to each patient’s first eligible ADR; the results were concordant. Cluster-robust standard errors by patient were not universally feasible due to incomplete linkage; therefore, we present conservative case-level CIs and first-event results. Given the spontaneous-reporting nature of the INFARMED pharmacovigilance system, all events coded by the notifier as “death” were retained without re-adjudication of causality, in accordance with standard pharmacovigilance procedure. As such, these figures represent the frequency of ADR reports labelled as fatal, not the incidence or prevalence of treatment-related mortality, and are subject to well-recognized severity-reporting inflation. Each fatal entry was counted once per ICSR, and internal data-cleaning procedures removed within-report duplicate entries; however, misclassification between ADR-related and co-occurring deaths cannot be fully excluded in spontaneous notification systems. Although the dataset includes whether death was reported as an outcome, the Portal RAM system does not record a structured date of death; therefore, the interval between ADR onset and fatal outcome could not be computed, and time-to-death analyses were not feasible.
2.2. Ethical Considerations
The study was approved by the Unidade Local de Saúde Lisboa Ocidental Ethics Committee, with authorization for use of anonymized INFARMED pharmacovigilance data; informed consent was not required under national regulations and the Declaration of Helsinki.
2.3. Statistical Analysis
All statistical analyses were performed using a contemporary software environment (SPSS Statistics version 26) on the final dataset of 2300 ADR cases. We first performed descriptive analyses to summarize the cohort characteristics. Continuous variables are reported as means with standard deviations or medians with interquartile ranges. Categorical variables are presented as frequencies and percentages of the total. The primary comparison of interest was between the younger (<70 years) and older (≥70 years) patient groups. We used chi-square tests (or Fisher’s exact test when expected cell counts were <5) to compare proportions between these age strata for categorical endpoints. Key comparisons included the proportion of cases classified as serious versus non-serious, the occurrence of fatal outcomes, hospitalizations, and the distribution of organ-specific irAEs in older versus younger patients. For continuous or ordinal outcomes (e.g., time-to-onset of an ADR), we assessed group differences using non-parametric tests (Mann–Whitney U) given the skewed distributions; for instance, the time-to-onset variable was not normally distributed. A two-sided α-level of 0.05 was used to determine statistical significance for all hypothesis tests. We evaluated multiple secondary comparisons across the other subgroups. These included analyses by sex (male vs. female), tumor group, treatment type, regimen (monotherapy vs. combination), CTLA-4 use, polypharmacy category, and calendar period (early vs. late cohort). For each of these, contingency tables were constructed for outcomes such as serious vs. non-serious rates, fatality, hospitalization, and immune-related event frequency, and tested using the chi-square test. Given the number of comparisons, we interpreted p-values with caution; the findings were highlighted as exploratory. No formal adjustment for multiple testing was applied because the analyses were largely descriptive; however, we emphasized consistent patterns over isolated p-value significance.
To identify independent predictors of severe toxicity, we performed multivariable logistic regression modeling of the odds of a report being serious versus non-serious. Candidate predictors were chosen a priori based on clinical interest and the univariate results. The final model included age group (≥70 vs. <70), sex, treatment regimen (combination vs. monotherapy), CTLA-4 regimen (whether the ICI regimen included a CTLA-4 inhibitor), polypharmacy (treated as an ordinal variable by category), tumor type (with dummy indicators for melanoma, NSCLC, renal cell carcinoma, and breast cancer, using all other tumors as the reference category), and calendar period (2017–2024 vs. 2011–2016). These variables were entered simultaneously into the logistic model to adjust for potential confounding factors and to estimate each factor’s independent association with severe irAE occurrence. The results are reported as odds ratios (OR) with 95% confidence intervals and p-values for each covariate. Model fit was assessed using the pseudo R-squared and Hosmer–Lemeshow goodness-of-fit tests. In a second multivariable analysis, we examined predictors of fatal outcomes using logistic regression on a subset of serious cases (outcome: death vs. non-fatal outcome), incorporating the same covariates. Similarly, a model for hospitalization was explored. These additional models were considered to be exploratory. We checked for multicollinearity among predictors (for example, CTLA-4 use is largely encompassed by combination therapy status) and found acceptable variance inflation factors. No interaction terms were included in the final models, given the limited sample size for higher-order interactions; however, we specifically examined whether age might modify the effect of the regimen in stratified analyses. The results of the subgroup analyses are described to corroborate the main findings. All statistical tests were performed using two-tailed tests. Analyses and data visualization followed the ESMO recommendations for real-world evidence reporting, and all figures and tables were generated directly from the analyzed dataset.
2.4. Missing Data
We quantified the variable-level missingness prior to the analysis. Time-to-onset was available for 542/2300 ADR cases (23.6%); thus, 76.4% were missing. Missingness was low for core covariates used in the multivariable models (tumor type, ICI class/regimen, age group, sex, calendar period, and polypharmacy), and these records were excluded from the relevant models. Therefore, all regression analyses were conducted as complete-case analyses, and no imputation was performed. Descriptive percentages were reported using non-missing denominators and footnoted accordingly. Sensitivity analyses excluding the “unknown/not reported” categories (where present) yielded estimates consistent with the primary results.
3. Results
Of the 3690 ADRs screened, from 1406 patients, 2300 unique ICI-related ADRs met the inclusion criteria, corresponding to 925 patients (Figure 1). The patients’ ages ranged from 20 to 93 years, with a median age of 65. One-third of the ADR cases (33.7%, n = 775) involved older adults (≥70 years), while the remaining 66.3% (n = 1525) were younger than 70 years. Men accounted for most of the reports (62.8%). The most common cancer type was lung cancer (31.3%), followed by melanoma (15.5%) and breast cancer (8.1%), respectively. Other malignancies accounted for 45% of the reports (including genitourinary, gastrointestinal, head-neck cancers, and others not enumerated). Regarding ICI treatments, PD-1 inhibitors were implicated in 77.5% of the reports (n = 1783), PD-L1 inhibitors in 15.2%, and CTLA-4 inhibitors in 4.9%, either alone or in combination (2.4% involved dual ICI combinations, such as anti–PD-1 plus anti–CTLA-4). In 72.9% of cases, ICI was administered as monotherapy, whereas 27.1% were combination regimens. Regarding the burden of comorbid pharmacology, over one-fifth of patients (11.2%) were on >5 concomitant medications at the time of the ADR, with an additional 11.8% on 3–5 other drugs, and 77.0% on 0–2 concomitant medications (Table 1).
The majority of ICI-related ADRs were categorized as “serious”: 1974 out of 2300 reports (85.8%) met the regulatory definition of a serious ADR, and 326 (14.2%) were classified as non-serious events. Among serious cases, the specific outcomes varied according to clinical seriousness. Fatal outcomes were reported in 19.1% of all cases (n = 440), corresponding to a 1:5 ratio of deaths associated with ICI-induced ADRs. Similarly, hospitalizations were reported in 17.9% of the cases (n = 412). “Important medical event” was the most frequently selected seriousness criterion (53.7%). A breakdown of cases by CTCAE-equivalent grade extrapolation illustrates this distribution: 19.1% of cases corresponded to Grade 5 (death), approximately 6.7% to life-threatening (Grade 4) events, and 6.3% to serious events leading to hospital stay or disability (Grade 3), while the remaining serious reports were categorized as medically important significant events not immediately life-threatening, 53.7% (Grade 2). Only 14.2% of reports were truly mild (non-serious, roughly corresponding to CTCAE grade 1). Detailed cross-tabulations of seriousness, immune-related labeling, hospitalization, and CTCAE-equivalent grades by age group are provided in Supplementary Table S1, with graphical grade distributions shown in Supplementary Figure S1. irAEs were further differentiated in immune-mediated, those considered triggered by immune activation from checkpoint blockade, versus non-immune-mediated events; overall, 9.0% of the reports (n = 207) were judged to represent immune-mediated toxicities (such as autoimmune pneumonitis, colitis, hepatitis and endocrinopathies), whereas the vast majority (91.0%) were classified as “other” events that are either not typical irAEs or not clearly immune in origin (for example, infusion reactions, infections, diarrhea, ataxia, or other complications). The median time from treatment initiation to ADR onset was 30 days (0–90 days) in the subset of reports with available timing data (n = 542); however, a large fraction of reports had an onset within the first few days of therapy, resulting in an overall median of 0 days in both age groups.
Age-stratified comparisons of outcomes between patients ≥ 70 years and those younger revealed that elderly patients did not experience a higher overall frequency of serious ADRs: the proportion of reports classified as serious was 84.5% in the ≥70 group (655/775) versus 86.5% in those <70 (1319/1525), a difference that was not statistically significant (p = 0.22) (Figure 2). However, fatal irAEs were markedly more common in elderly patients than in younger patients. Among the ≥70 group, 25.3% of cases were fatal, compared to 16.0% in <70 adults. This 1.6-fold increase in fatal outcome frequency in the elderly was highly significant (p < 0.001) and corresponded to an excess risk of death attributable to irAEs in older patients. In absolute terms, 196 of 775 reports in the ≥70 cohort involved patient death versus 244 of 1525 reports in younger patients. In contrast, the rate of hospitalization did not differ appreciably by age: 16.6% of older patients had an ADR leading to hospital admission vs. 18.5% of younger patients (p = 0.21), indicating a similar likelihood of requiring inpatient care for managing toxicity. The fraction of events deemed immune-related (9% in ≥70 vs. 8.7% in <70) was also similar (p = 0.56). Thus, aside from mortality, the overall seriousness and broad categories of events were comparable between the age groups. Despite comparable aggregate serious-event rates, the organ-system distribution differed modestly by age. Older adults had a higher representation of events coded under Immune system disorders (9.0% vs. 6.6%, p = 0.039), largely driven by immune-mediated endocrinopathies (e.g., thyroiditis), immune-mediated skin disorders, and a relative enrichment of myocarditis, patterns consistent with the age-related shift observed in prior studies. Conversely, younger patients contributed proportionally more cases of immune-mediated colitis and hepatitis They also had significantly more nervous system disorders reported (8.5% vs. 5.0%, p = 0.002), suggesting neurologic irAEs (such as immune-related neuropathies or encephalitis) were relatively more frequent in older individuals. In contrast, younger patients showed higher rates of hepatic and biliary ADR (7.2% of <70 reports vs. only 3.7% in ≥70, p = 0.001) and more blood or lymphatic disorders (7.0% vs. 3.7%, p = 0.003) (Figure 3). There was no significant age difference in several other common organ categories: for example, endocrine disorders were numerically more frequent in older patients (11.1% vs. 8.7% in <70), but this did not reach significance (p = 0.07); skin-related irAEs occurred in 9% of cases in both groups (p = 0.31). Gastrointestinal (colitis) and respiratory (pneumonitis) event rates were also similar by age (8% in both groups) (Table 2). The median time-to-onset of toxicity did not differ by age: both groups had a median of 0 days from ICI start to event (with an identical proportion of events occurring on day 0, likely infusion reactions or acute events). Considering the non-zero events, the distribution of onset timing was broad and showed no clear shift between age groups (p = 0.65 for difference in time-to-onset). A global overview of age-related organ-system involvement across all MedDRA System Organ Classes is shown in Supplementary Figure S2. Age-related shifts in MedDRA System Organ Classes are presented in Supplementary Figure S3, and the most frequently reported adverse events and immune-related events by age group are summarized in Supplementary Table S2. Graphical representations of these age-stratified adverse event patterns are provided in Supplementary Figure S4.
In addition to the age-stratified analyses, we performed exploratory evaluations by sex, tumor type, treatment regimen, polypharmacy, temporal trend and reporter type. Given their descriptive nature, the full cross-tabs and model outputs are provided in Supplementary Materials.
Overall safety outcomes were comparable by sex, with similar rates of serious events (p = 0.89) and fatal outcomes (19.8% in males vs. 18.0% in females, p = 0.31). Men, however, were more frequently hospitalized (p = 0.002) and showed a non-significant trend toward more immune-related events (9.8% vs. 7.7%, p = 0.11). Sex-specific patterns emerged, with women reporting more endocrine (11.7% vs. 8.4%, p = 0.001) and hematologic disorders, while men had higher frequencies of respiratory and vascular toxicities (1.9% vs. 0.6%; p = 0.014); onset timing did not differ. Toxicity patterns varied by tumor type. Melanoma cases had the highest burden, with 89.3% serious events, 36.5% hospitalizations, and 29.8% fatality, while NSCLC (n = 719) showed lower seriousness rate (81.6% serious, 14.9% fatal) but the highest frequency of immune-related events (12.9%). Renal cell carcinoma (21.1% fatal, only 2% hospitalized) and breast cancer (93% serious but only 2.7% fatal and no hospitalizations) illustrated marked heterogeneity, with breast cancer patients experiencing the most favorable outcomes. Combination regimens were associated with a higher proportion of serious events than monotherapy (91.0% vs. 84.3%, p < 0.001), but paradoxically with lower fatality (13.6% vs. 21.2%, p < 0.001) and hospitalization rates (7.5% vs. 21.8%, p < 0.001), as well as fewer immune-mediated events (6.1% vs. 10.1%, p = 0.004). In contrast, CTLA-4–containing regimens (n = 168, predominantly ipilimumab-based) carried a markedly worse profile: although the proportion of serious ADRs was similar to non-CTLA-4 (89.9%), fatality reached 40.5% versus 17.4% (p < 0.001) and hospitalizations 43.5% versus 15.9% (p < 0.001). Immune-mediated events were also more frequent with CTLA-4 (14.3% vs. 8.6%, p = 0.012), despite these regimens being more often used in younger (34% <70 vs. 24% ≥70) and male (61%) patients. Polypharmacy influenced outcomes, as patients on 3–5 concomitant drugs had the highest hospitalization rate (28.7% vs. 16.7% with ≤2 drugs; p < 0.001) but the lowest fatality (11.0% vs. 20% in other groups; p < 0.001). In contrast, those on >5 medications experienced the highest mortality (22.9%, above the 19.8% baseline; p < 0.001) despite a lower overall rate of serious events (80.6%). ADR seriousness reporting declined over time: serious events (91.7% to 85.3%), hospitalizations (32.0% to 16.7%), and fatal outcomes (58.6% to 15.8%) were all significantly less frequent in 2017–2024 compared to 2011–2016. In contrast, the proportion of immune-related events increased (9.5% vs. 3.3%), reflecting improved recognition and reporting. The seriousness of ADRs was consistent across reporter types (p = 0.31), with healthcare professionals submitting the majority and patient reports representing 3.5% of cases. Notably, patient-reported events were not less severe, and over half involved fatal outcomes, though absolute numbers were small.
To disentangle the contributions of various factors to severe toxicity, we built a multivariate logistic regression model for the outcome of serious vs. non-serious ADR. In this adjusted analysis, age ≥ 70 was not an independent predictor of severe irAE occurrence (OR = 0.98, 95% CI 0.76–1.27, p = 0.89), confirming that older patients, after accounting for other variables, were not more likely than younger patients to experience a reportable event meeting seriousness criteria (Figure 4). Sex likewise had no significant effect on seriousness (male vs. female OR = 1.18, 95% CI 0.91–1.53, p = 0.20). In contrast, combination immunotherapy had an adjusted OR of 1.57 (95% CI 1.13–2.18, p = 0.007) for producing a serious ADR compared to monotherapy. Combination therapy conferred 57% higher odds of a severe reaction. Neither polypharmacy (OR = 0.87 per category, 95% CI 0.73–1.03, p = 0.11) nor calendar period (2017–2024 vs. 2011–2016; OR = 1.09, 95% CI 0.83–1.42, p = 0.54) were significant predictors of a serious events. Tumor type was an independent predictor of seriousness: renal cell carcinoma (OR = 2.06, 95% CI 1.09–3.87, p = 0.025) and breast cancer (OR = 2.12, 95% CI 1.06–4.02, p = 0.021) both showed higher odds of severe ADRs compared with “other” tumors. Melanoma showed a non-significant trend toward increased seriousness (OR = 1.45, p = 0.06), while NSCLC did not differ significantly (OR = 0.84, p = 0.20). Using breast cancer as the reference confirmed these findings, with lung cancer showing significantly lower odds of seriousness and melanoma marginally lower, underscoring the unexpectedly high seriousness classification in breast cancer despite low fatality. The model’s pseudo-R^2^ was 0.02, indicating that most variability in ADR seriousness remained unexplained, likely reflecting unmeasured toxicity patterns or reporting practices.
In the multivariable model for fatal outcomes, advanced age independently increased the odds of death (OR = 1.66, 95% CI 1.3–2.1, p < 0.001). Tumor type had a strong effect: relative to breast cancer, melanoma (OR = 7.1, p < 0.001), other tumors (OR = 7.9, p < 0.001), and NSCLC (OR = 4.5, p = 0.002) carried markedly higher risks, while treatment regimen was not an independent predictor (OR = 0.90 for combination vs. monotherapy, p = 0.45). CTLA-4 use trended toward higher fatality (OR = 1.5, p = 0.09), whereas later calendar period (2017–2024) was protective (OR = 0.16 vs. 2011–2016, p < 0.001). A parallel hospitalization model showed male sex (OR = 1.35, p = 0.018), younger age (OR = 0.74, p = 0.014), CTLA-4 use (OR = 2.9, p < 0.001), and non-combination regimens (OR = 0.35 for combination, p < 0.001) as independent predictors. Sensitivity analyses restricted to each patient’s first ADR were concordant with the main findings (Supplementary Figure S5).
4. Discussion
In this national pharmacovigilance cohort (n = 2300), chronological age was not associated with increased odds of reporting a serious ICI-related adverse event or with higher rates of hospitalization; however, older adults (≥70 years) had a substantially higher case-fatality (25.3% vs. 16.0%; adjusted OR 1.66, 95% CI 1.31–2.09). Age was further associated with a shift in toxicity phenotype: older patients experienced proportionally more nervous and immune system events and fewer hepatobiliary and hematological events, whereas the overall frequency of explicitly immune-mediated events remained similar across age groups. These findings suggest that age might primarily influence outcomes and toxicity phenotypes rather than the incidence of adverse events.
Patients aged ≥70 years comprised approximately one-third of the cohort, with the proportion of serious ADRs being essentially identical to those <70 years (84.5% vs. 86.5%). In adjusted analyses, age was not an independent predictor of a report being serious (OR 0.98; 95% CI 0.76–1.27; p = 0.89). Taken together, these data indicate that chronological age alone does not increase the incidence of immunotherapy toxicities, consistent with prior reports showing comparable any-grade and high-grade irAEs rates in older adults [21,24,32], including a series of patients ≥ 80 years [25]. However, when toxicity does occur in older populations, the prognosis is notably poorer, with fatality rates among reported irAEs being 1.77-fold higher in patients aged ≥70 compared to younger counterparts, and advanced age persisting as an independent predictor of mortality in multivariable modeling. This suggests that chronological age, rather than elevating the incidence of toxicity, may amplify its clinical consequences. Plausible contributors include biological frailty and reduced physiological reserve (e.g., an immune-mediated pneumonitis or colitis that is survivable at younger ages may be lethal with limited cardiopulmonary or metabolic reserve), as well as comorbidity burden (e.g., underlying interstitial lung disease) that magnifies organ-specific injury [21,22,24,25,32]. Differences in management may also play a role: clinicians may be more conservative with escalation or high-dose corticosteroids in the very old, influenced by concerns about treatment complications or perceived lower survival potential and higher care burden [20,22]. Notably, hospitalization was not more frequent in ≥70 years (slightly lower, non-significant), which could reflect outpatient/hospice management, under-notification of admissions in the elderly, or deterioration preceding admission. Overall, these data align with clinical experience that older adults are more vulnerable to the consequences of severe irAEs despite a similar baseline risk of experiencing them. This increased vulnerability is biologically plausible in the context of immunosenescence, characterized by thymic involution, reduced naïve T-cell output, expansion of autoreactive memory clones, and dysregulated immune homeostasis, which alters how the aging immune system responds to immune activation and may impair recovery from tissue injury [24,26,27,28]. Interestingly, we observed distinct SOC patterns by age: older adults had relatively more immune system and nervous system disorders, whereas younger patients showed higher hepatobiliary and hematologic events. These distributions are consistent with the organ-specific profiles shown in Supplementary Figure S3 and Supplementary Table S2. Prior work also suggests age-linked shifts in irAE spectra, e.g., more dermatologic/rheumatologic toxicities in older adults and more colitis/hepatitis in younger cohorts, although findings have been heterogeneous [22,25,32,33]. Our data are partly concordant: fewer hepatic events in ≥70 years (consistent with a less reactive hepatic immune milieu) and a numerical increase in endocrine events with age, albeit non-significant [9,26,32]. The higher neurologic irAEs signal in the elderly is notable; given their seriousness and relative rarity, this could reflect greater biological susceptibility (frailty of neural/blood–brain barrier repair) or differential recognition/reporting [14,15,20,22,34]. Conversely, younger patients’ excess hematologic events may align with a more vigorous immune repertoire capable of autoimmune cytopenias. Mechanistically, immunosenescence, with dampened effector responses but expansion of autoreactive memory clones, could shift organ vulnerability and clinical expression [22,24,32,33,35]. Clinically, these patterns argue for age-attuned surveillance (e.g., higher suspicion for encephalitis in the elderly vs. hepatitis in younger adults) [25,26]. Importantly, the overall irAE frequency was comparable across ages; the difference lies in the proportions, not presence, of organ-specific toxicities.
In further exploratory, adjusted analyses, combination therapy independently increased the odds of an ADR being classified as serious (aOR 1.57), although it did not raise mortality rates within the cohort. Regimens containing CTLA-4 inhibitors were associated with the most unfavorable crude outcomes, including higher rates of fatality and hospitalization, consistent with established toxicity profiles of these agents [14,15,36,37]. Tumor type remained associated with seriousness/fatality (e.g., higher seriousness in renal cell carcinoma (RCC) and breast vs. “other”), likely reflecting regimen mix and case-mix. Sex showed little difference for overall seriousness or death, but phenotype diverged, more endocrine events in women; more respiratory/vascular toxicities and higher hospitalization in men, aligning with prior sex-immune literature [38,39,40]. Polypharmacy and calendar period were not independent drivers of serious vs. non-serious after adjustment, although 2017–2024 was associated with lower fatality, consistent with the transition to PD-(L)1 agents and maturing irAE management [14,15,36]. Full coefficients and forest plots are provided in the Supplementary Materials.
This analysis is constrained by the well-recognized biases of spontaneous pharmacovigilance data. First, severity bias and under-reporting likely inflate the proportion of serious and fatal cases captured: 86% of reports in our cohort were classified as serious and 19% as fatal, figures that far exceed trial-based estimates of fatal irAEs (<1%) and large real-world series (0.6%), reflecting selective reporting rather than population risk [36,41,42,43]. Spontaneous systems miss most ADRs (median under-reporting 94%; even serious ADRs 80–85% under-reported), so mild/moderate toxicities are under-ascertained [44,45]. Second, event misclassification and incomplete granularity are probable. The designation “immune-mediated” versus other ADRs relied on reporter judgment/MedDRA coding; classical irAEs may have been filed under organ SOCs (e.g., hepatitis, colitis) or, conversely, non-immune events over-attributed to ICIs. Timing data were sparse and sometimes imprecise (frequent “day-0” entries), precluding robust latency analyses [42,45]. Third, residual confounding cannot be excluded. Indication and regimen (e.g., CTLA-4 exposure) correlate with both toxicity and reporting; multivariable adjustment attenuated but did not remove confounding. The model for serious vs. non-serious had low explanatory power (pseudo-R^2^ 0.02), suggesting unmeasured determinants (toxicity phenotype, management thresholds, reporter behavior). Given the very low pseudo-R^2^ (0.02), the seriousness model has limited predictive power and should be interpreted as identifying the direction rather than the magnitude of associations. Fourth, missing covariates and unknown denominators limit inference. We lacked performance status, comorbidities, laboratory values, and treatment setting; polypharmacy was an imperfect proxy for comorbidity. The number of ICI-treated patients in Portugal is unknown, so incidence cannot be estimated; findings characterize risk patterns within reported ADRs, not absolute rates. Finally, age was modeled primarily as <70/≥70 (chosen a priori); while consistent with sensitivity analyses, very-old-age effects may be obscured, and differential reporting across subgroups cannot be excluded.
Taken together, these real-world findings suggest that chronological age, per se, should not preclude immunotherapy. Older adults (≥70 y) were no more likely than younger patients to experience an ADR classified as “serious”, yet, once a toxicity occurred, the risk of death was higher in the older group. This pattern supports equitable access to ICIs for fit older people, paired with age-attuned safety nets to mitigate consequence-of-toxicity risk [14,15,20,25,33,34]. The age signal we observed was phenotypic rather than incidence-based: older adults had relatively more nervous-system and immune-system disorders, whereas younger adults showed more hepatobiliary and blood/lymphatic events. Clinically, this warrants a lower threshold in ≥70 y for urgent evaluation and early immunosuppression (e.g., corticosteroids per ESMO/ASCO guidance) when facing encephalopathy, neuropathy, myasthenic syndromes, aseptic meningitis/encephalitis, or multisystem immune activation; for <70 y, maintaining routine liver chemistries and complete blood counts through early cycles remains high yield to detect immune hepatitis and cytopenias at presentation [14,15,20,22]. Regardless of age, new dyspnea, diarrhea, chest pain or severe fatigue should trigger protocolized same-day work-ups. To operationalize vigilance, centers should front-load monitoring in cycles 1–2, the window in which many irAEs declare, by (i) pre-authorizing rapid-access irAEs clinics with same-day labs and imaging; (ii) implementing escalation checklists for older adults (triggers for ED evaluation/admission and step-up to high-dose steroids or second-line agents); and (iii) scheduling 48–72 h follow-up (in person or telemedicine) after any grade ≥ 2 toxicity until improvement. Embedding irAE order sets and steroid-taper templates within the electronic record reduces delays and variation [14,15,20]. Because the hazard in older adults relates to outcome severity rather than event frequency, pre-treatment geriatric assessment should guide monitoring intensity and thresholds for intervention. A brief clinic-feasible bundle (mobility/falls, polypharmacy, cognition, nutrition, social support, comorbidity burden) can stratify physiological reserve and help anticipate toxicities that older patients tolerate poorly (pneumonitis, myocarditis, neuro-irAEs). The development and validation of a pragmatic score to estimate fatal/near-fatal irAEs risk in older adults is a priority [20,22,33,34]. CTLA-4-containing schedules require heightened caution: baseline stool history, early GI input, and a “treat-early” steroid stance for diarrhea/abdominal pain to prevent complicated colitis, the dominant cause of ipilimumab-related deaths in prior reports [14,15,28]. For PD-(L)1 monotherapy, the emphasis is on thyroid/adrenal surveillance and prompt work-up of respiratory or hepatic symptoms. For combination regimens, which in our data increased the odds of being classified as serious but did not increase mortality, proactive education and scheduled toxicity check-ins often keep events from escalating, and higher event frequency need not translate into higher lethality when structured management is in place [14,15,36]. A practical cadence is weekly labs during cycle 1 (ALT/AST/bilirubin, ALP, CBC; TSH/FT4 and morning cortisol if symptomatic), then at each infusion through cycle 4, with earlier repetition for symptoms. In ≥70 y with headache, confusion, gait change or focal deficits, adopt a low threshold for brain MRI and neurology consultation; maintain a low threshold for CT chest and pulse-oximetry trending with any new cough or exertional dyspnea in all ages [14,15,20]. Outcomes improved over time, plausibly reflecting better clinician education and earlier intervention [14,15,20,28]. Continuing this trajectory requires patient-centered education (plain-language action plans; wallet cards/app-based alerts; 24/7 contact pathways) and onboarding of primary-care and emergency teams, since first presentations often occur outside oncology clinics. Given the higher case-fatality in older adults, caregivers should be explicitly enlisted to report early neurologic or constitutional changes.
Our analysis underscores the value, and current limitations, of spontaneous reporting. Enhancing pharmacovigilance for ICIs with structured fields (onset date, CTCAE grade, management, outcome) and encouraging reporting of all grades of suspected irAEs would improve signal quality and refine practice benchmarks [24,46]. Prospective registries and patient-reported tools could better capture mild/moderate events that shape quality of life and adherence. As spontaneous reporting lacks a denominator, true incidence cannot be assessed. In practical terms, clinicians should counsel that most older adults will not suffer fatal toxicity, but the margin for delay is smaller. For borderline-fit patients, regimen choice (e.g., PD-1 alone rather than PD-1 + CTLA-4) can meaningfully reduce risk without foreclosing benefit [14,15,28]. As biomarker research matures (HLA, cytokines, microbiome), integration with geriatric metrics may further personalize monitoring and prophylaxis; until then, phenotype-aware surveillance, rapid escalation pathways, and geriatric-informed care are the highest-yield levers to maximize safety while preserving access to life-prolonging ICIs [20,22,33,34,36].
5. Conclusions
In this national pharmacovigilance cohort, chronological age did not increase the odds of experiencing an ICI-related adverse event, supporting the use of ICIs in fit older adults; however, when irAEs occurred in patients ≥70 years, the risk of fatal outcome was higher, underscoring the need for earlier recognition and lower thresholds for escalation in this group. Toxicity phenotype varied by age (more nervous/immune-system disorders in older adults; more hepatobiliary/hematologic events in younger adults), by sex (more endocrine events in women; more respiratory/vascular events in men), and, most strongly, by regimen: CTLA-4-containing schedules showed the severest profiles, whereas PD-1/PD-L1 monotherapy (e.g., in NSCLC) showed a better safety outcome. Combination therapy increased the volume of reported toxicity but did not increase mortality, consistent with effective monitoring and management. Temporal trends suggest improving safety with wider PD-1/PD-L1 adoption and greater clinician experience. Taken together, these findings highlight the complex interplay between age, immune function, and the expression of irAEs, reflecting the biological heterogeneity introduced by age-related immune remodeling. Although immunosenescence may not increase the likelihood of developing an irAE, it may influence how toxicities manifest and how well patients recover once severe inflammation occurs. As far as we are aware, this is also the first national real-world evaluation of ICI safety in Portugal, offering a comprehensive perspective on how these therapies perform outside trial settings. These findings, while influenced by the severity bias of spontaneous reporting, provide actionable signals for practice: maintaining access to ICIs for older adults, implementing front-loaded monitoring and rapid-response pathways, especially for CTLA-4 regimens, and tailoring surveillance by patient phenotype. Reporting of irAEs should be actively encouraged. Prospective registry linkages and development of pragmatic geriatric risk tools should be prioritized to refine risk stratification and further reduce fatal irAEs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ribas A. Wolchok J.D. Cancer immunotherapy using checkpoint blockade Science 20183591350135510.1126/science.aar 406029567705 PMC 7391259 · doi ↗ · pubmed ↗
- 2Bagchi S. Yuan R. Engleman E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance Annu. Rev. Pathol. Mech. Dis.20211622324910.1146/annurev-pathol-042020-04274133197221 · doi ↗ · pubmed ↗
- 3Shiravand Y. Khodadadi F. Kashani S.M.A. Hosseini-Fard S.R. Hosseini S. Sadeghirad H. Ladwa R. O’byrne K. Kulasinghe A. Immune Checkpoint Inhibitors in Cancer Therapy Curr. Oncol.2022293044306010.3390/curroncol 2905024735621637 PMC 9139602 · doi ↗ · pubmed ↗
- 4Shahid K. Khalife M. Dabney R. Phan A.T. Immunotherapy and targeted therapy—The new roadmap in cancer treatment Ann. Transl. Med.2019759510.21037/atm.2019.05.5831807576 PMC 6861781 · doi ↗ · pubmed ↗
- 5Garg P. Pareek S. Kulkarni P. Horne D. Salgia R. Singhal S.S. Next-Generation Immunotherapy: Advancing Clinical Applications in Cancer Treatment J. Clin. Med.202413653710.3390/jcm 1321653739518676 PMC 11546714 · doi ↗ · pubmed ↗
- 6Martins F. Sofiya L. Sykiotis G.P. Lamine F. Maillard M. Fraga M. Shabafrouz K. Ribi C. Cairoli A. Guex-Crosier Y. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance Nat. Rev. Clin. Oncol.20191656358010.1038/s 41571-019-0218-031092901 · doi ↗ · pubmed ↗
- 7Pillai R.N. Behera M. Owonikoko T.K. Kamphorst A.O. Pakkala S. Belani C.P. Khuri F.R. Ahmed R. Ramalingam S.S. Comparison of the toxicity profile of PD-1 versus PD-L 1 inhibitors in non–small cell lung cancer: A systematic analysis of the literature Cancer 201712427127710.1002/cncr.3104328960263 PMC 5761314 · doi ↗ · pubmed ↗
- 8Blum S.M. Rouhani S.J. Sullivan R.J. Effects of immune-related adverse events (ir A Es) and their treatment on antitumor immune responses Immunol. Rev.202331816717810.1111/imr.1326237578634 · doi ↗ · pubmed ↗