Disparities in Non-Small Cell Lung Cancer (NSCLC) by Age, Sex, and Race: A Systematic Review and Meta-Analysis of Immune Checkpoint Inhibitor (ICI) Trials
Maxim Yaskolko, Christopher Liu, Alexander Barsouk, Jonathan H. Sussman, Adam A. Barsouk

TL;DR
This study finds Asian patients with lung cancer have better survival on immunotherapy than White patients, while Black patients are underrepresented in trials.
Contribution
A meta-analysis of immunotherapy trials in NSCLC reveals survival disparities by race and highlights underrepresentation of Black patients.
Findings
Asian patients had higher survival rates on immunotherapy compared to White patients.
Black patients were underrepresented in the trials, limiting analysis of their outcomes.
No significant differences in survival were found by sex or age.
Abstract
We conducted a meta-analysis of all immunotherapy (PD-1, PD-L1, CTLA-4) trials in non-small cell lung cancer (NSCLC) for survival disparities by race, sex, and age. We found that Asian patients had higher rates of survival compared to White patients on immunotherapy and overall. Black patients were underrepresented in the trials. We did not find any difference in survival by sex or age. Furhter research and greater diversity in NSCLC trials is required to ensure optimal outcomes for all patient populations. Background: While immune checkpoint inhibitors (ICIs) have improved survival in mNSCLC, outcomes may be disparate by age, race, and sex. However, given the limited diversity of trial populations, data are limited. Methods: A systematic review and meta-analysis were conducted of phase III prospective trials of ICIs in mNSCLC initiated after 2015, identified from PubMed and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
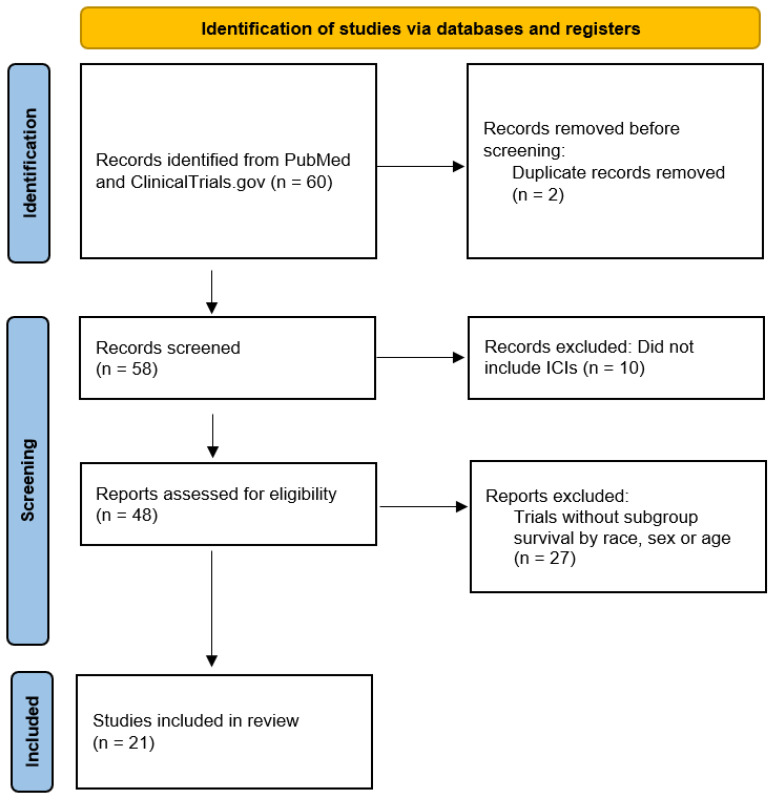 Figure 1
Figure 1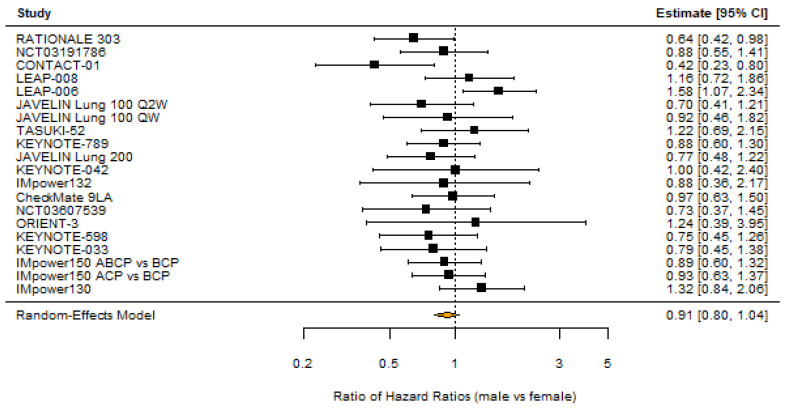 Figure 2
Figure 2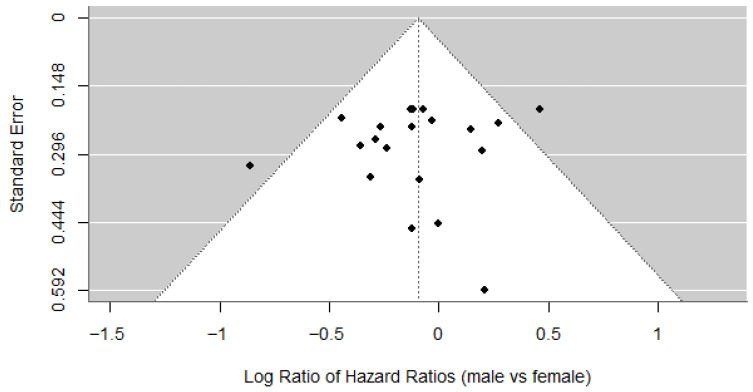 Figure 3
Figure 3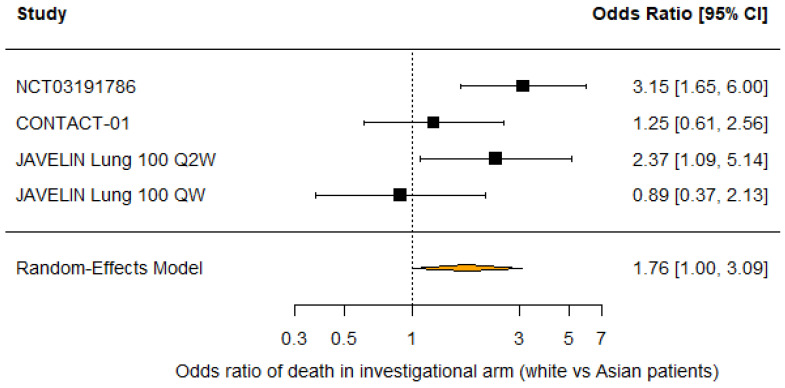 Figure 4
Figure 4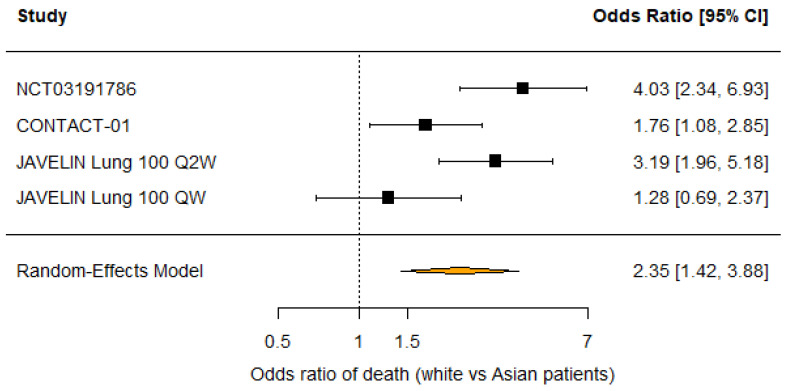 Figure 5
Figure 5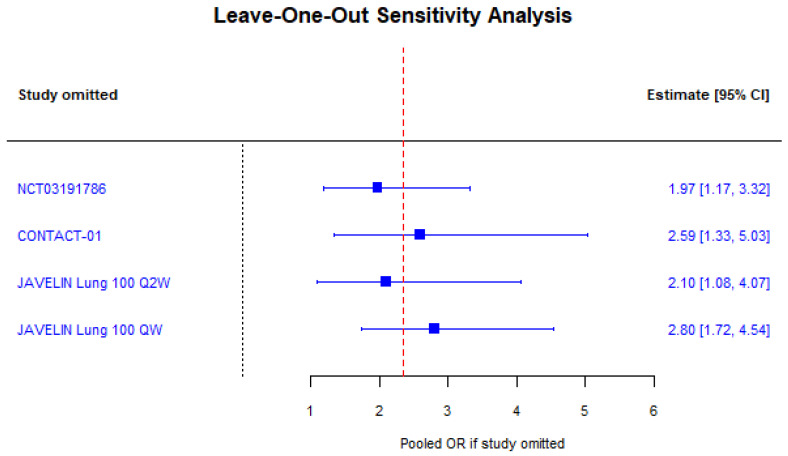 Figure 6
Figure 6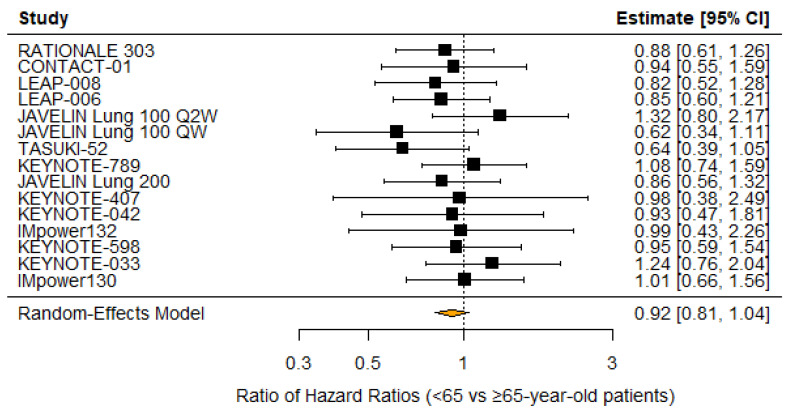 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Lung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment
1. Introduction
Non-small cell lung cancer (NSCLC) remains the leading cause of cancer mortality worldwide, with immune checkpoint inhibitors (ICIs) revolutionizing treatment and improving survival in advanced disease [1,2]. PD-1 and PD-L1 inhibitors pembrolizumab, cemiplimab, atezolizumab, nivolumab (+/−) ipilimumab (a CTLA-4 inhibitor), and durvalumab + tremelimumab (CTLA-4 inhibitor) have all been FDA approved for wild-type 1L mNSCLC, largely in combination with platinum chemotherapy; pembrolizumab, cemipilimab, and atezolizumab are also approved as monotherapies for patients with PDL1 TPS expression >50%. Novel therapeutics in development include PD1xVEGF bispecifics like ivonescimab, antibody drug conjugates like datopotomab deruxtecan and sacituzimab govetecan, and nanotechnology enabled sensitizers. Despite these advances, disparities in clinical outcomes and trial representation persist across age, sex, and racial groups [3].
Older adults are historically underrepresented in ICI trials, yet available evidence suggests comparable efficacy and toxicity profiles to younger patients, though some studies indicate attenuated benefit in the oldest cohorts [4,5,6,7]. Disparities in ICI efficacy by sex have been explored, with most meta-analyses reporting similar survival benefits for men and women. However, some data suggest women may derive greater benefit from combination regimens, and tumor mutational burden may modulate sex disparities [8,9,10,11,12]. Racial disparities are evident in both trial enrollment and real-world access to ICIs. Black and Hispanic patients have remained underrepresented in prospective NSCLC trials in the US [13], limiting conclusions on disparities. While limited meta-analyses indicate similar survival benefits for White and Asian patients [14,15,16], some meta-analyses across tumor types have suggested Asian patients may have superior survival over white patients [17,18].
Prior studies have reported inconsistent findings regarding disparities in enrollment or treatment efficacy by age, sex, and race among NSCLC patients treated with ICI therapy. This comprehensive meta-analysis of phase III clinical trials, those best designed to evaluate efficacy, aims to systematically identify disparities in enrollment and reporting, and to clarify the impact of age, sex, and race on ICI efficacy in NSCLC. These findings can inform clinical decision-making and guide future trial design toward more equitable cancer care.
2. Methods
2.1. Search Strategy
We conducted a systematic review of completed prospective phase III trials in mNSCLC evaluating ICIs (pembrolizumab, atezolizumab, nivolumab +/− ipilimumab, durvalumab +/− tremelimumab) initiated after 2015 using PubMed and ClinicalTrials.gov. This approach selects trials of the highest methodological quality and minimal bias that are most likely to provide complete and relevant evidence in the current therapeutic landscape. The analysis was conducted in September 2025. We used the following search string to identify 60 trials: AREA[ConditionSearch](Non Small Cell Lung Cancer) AND AREA[StartDate] RANGE [1 January 2015, MAX] AND AREAOverallStatus AND AREAPhase AND AREAStudyType AND (AREA[HasResults] true). Two duplicate studies were excluded, and 10 studies that did not investigate ICIs were excluded.
2.2. Inclusion Criteria
Trials were evaluated for inclusion of baseline demographics—age, sex, and race—and for subgroup analyses of overall survival (OS) by age, sex, and race in the published manuscript. Two authors independently conducted the screening, and for any paper identified by one author but not the other, a third author was consulted to determine if the identified report met the inclusion criteria, which was then taken as the final decision.
2.3. Statistical Analysis
One author performed all data extraction, which a second author independently verified. Baseline demographic data for age, sex, and race were extracted from each trial. The primary outcome was the difference in OS benefit between subgroups, estimated by analyzing treatment-by-subgroup interactions using the ratio of hazard ratios (RHRs) for death, calculated from reported hazard ratios. Meta-analyses of these interaction effects were conducted for men vs. women, white vs. Asian, and for patients aged < 65 vs. ≥65. The secondary outcome was the difference in odds of death between subgroups, estimated by calculating odds ratios (ORs) for death events in both investigational and control arms. Meta-analyses of ORs for death were performed for the above subgroup comparisons in the investigational treatment arm and across all study arms. The primary outcome assesses relative treatment effect modification, while the secondary outcome evaluates absolute differences in mortality. For each meta-analysis, only studies with complete data for the relevant subgroup analysis were included. Random-effects models were used to pool results across studies in all meta-analyses to account for the inherent heterogeneity arising from differences in trial design, treatments, aims, and populations. Heterogeneity was also evaluated by Cochran’s Q test and I^2^ values. Significant heterogeneity was further investigated with leave-one-out sensitivity analysis. p values < 0.05 were considered significant. R v4.4.0 was used for statistical analysis (Foundation for Statistical Computing, Vienna, Austria). The meta for R package v4.5.2 was used for all meta-analyses. This systematic review followed the PRISMA 2020 guidelines and was not prospectively registered [19].
2.4. Bias Assessment
Publication bias was evaluated using Egger’s tests and funnel plots. Risk of bias was assessed using the Cochrane risk of bias tool 2, which rates each study on the following domains: randomization, deviations from intended interventions, missing outcome data, measurement of outcome, and selection of reported results.
3. Results
Our literature search identified 21 distinct trials (Figure 1). Two studies were multi-arm, yielding 23 total pairwise comparisons between investigational and control arms. Table 1 presents key characteristics of the trials and the significance of the OS benefit with the investigational treatment versus control across sex, race, and age subgroups. No trials were judged to be at high risk for bias. Some concerns were identified in all trials for bias due to the selection of reported results from limited demographic reporting or exploratory subgroup analyses (n = 23).
3.1. Sex
All trials (n = 10,950) reported sex distribution and OS subgroup analysis by sex. 68.5% of patients were men. 11/23 (47.8%) comparisons between investigational and control arms found that men had a significant overall survival benefit over control, while only 1/23 (4.5%) found that women had a significant overall survival benefit over control. A random-effects meta-analysis of the 20 comparisons that reported overall survival hazard ratios by sex suggested that women had a non-significantly smaller OS benefit with the investigational treatment compared to control (RHR 0.91 [95% CI: 0.80–1.04]; p = 0.17; Figure 2). Heterogeneity was low and not significant (I^2^ = 25.4%; p = 0.21), and there was no evidence of publication bias based on Egger’s test (p = 0.45) and a symmetrical funnel plot (Figure 3). Random-effects meta-analysis of the nine studies that reported deaths by sex in the investigational arms found that men did not have lower odds of death in the investigational arms (OR 0.98 [95% CI: 0.73–1.32]; p = 0.89).
3.2. Race
13/21 (61.9%) trials analyzed reported race distribution with 59.2% white, 34.8% Asian, 2.7% Native American or Alaskan Native patients, and only 1.5% Black patients. 7/21 (33.3%) trials reported OS subgroup analysis by race. 2/8 (25%) comparisons between investigational and control arms found that white patients had a significant overall survival benefit from the investigational treatment, while 1/6 (16.7%) comparisons found that Asian patients had a significant survival benefit. No trials reported subgroup analysis for Black patients due to small sample sizes. A random-effects meta-analysis of the five comparisons that reported overall survival hazard ratios for white and Asian patients suggested no difference in OS benefit with the investigational treatment compared to control (RHR 0.95 [95% CI: 0.73 −1.24]; p = 0.72). However, random-effects meta-analysis of the four comparisons that reported deaths by race in the investigational arm found that white patients had higher odds of death compared to Asian patients (OR 1.76 [95% CI: 1.00–3.09]; p = 0.0496; Figure 4). Similarly, white patients had higher odds of death across both treatment arms compared to Asian patients (OR 2.35 [95% CI: 1.42–3.88]; p < 0.001; Figure 5). Moderate heterogeneity in both analyses (I^2^ = 56.1%; p = 0.08 and I^2^ = 72.2%; p = 0.02) should be interpreted with caution as only four studies were included in each analysis. Furthermore, leave-one-out sensitivity analysis demonstrated that excluding any study did not significantly alter the pooled odds ratio of death among all patients, indicating that our results are robust (Figure 6). There was no evidence of publication bias by Egger’s test (p = 0.25 and p = 0.64).
3.3. Age
18/21 (85.7%) trials reported distribution by age ≥ 65 years vs. <65 years old, with 55.9% of patients <65 years old. 20 comparisons between investigational and control arms reported OS subgroup analysis by the <65 cutoff, while 17 reported death by the ≥65 cutoff. 7/20 (35%) found that patients <65 years old had a significant OS benefit with the investigational treatment, while 4/17 (23.5%) found that patients ≥65 years old had a significant OS benefit. A random-effects meta-analysis of the 15 comparisons that reported overall survival hazard ratios by age suggested that patients ≥65 years old have a non-significantly smaller OS benefit (RHR 0.92 [95% CI: 0.81–1.04]; p = 0.19; Figure 7). Random-effects meta-analysis of the 13 studies that reported deaths by age in the investigational arms found that men did not have lower odds of death in the investigational arms (OR 0.94 [95% CI: 0.77–1.15]; p = 0.54). No heterogeneity (I^2^ = 0; p = 0.84) or publication bias was detected by Egger’s test (p = 1.00).
4. Discussion
4.1. Disparity in Survival by Sex
All but one study failed to demonstrate that women benefited from investigational treatment compared with control. Still, our meta-analyses suggested that men and women had similar OS, and there was no significant difference in the benefit from investigational treatments, although the point estimate was a lower benefit for women (RHR 0.91, p = 0.17). Increased inclusion of women is needed to further explore this potential disparity. These results are in keeping with the existing literature.
Large meta-analyses and real-world studies consistently demonstrate that ICIs improve overall survival (OS) and progression-free survival (PFS) in mNSCLC for both sexes compared to chemotherapy, with most studies reporting no statistically significant difference in the magnitude of benefit between men and women [10,11]. However, some studies and meta-analyses suggest that men may derive greater benefit from ICI monotherapy, while women may benefit more from ICI-chemotherapy combinations [41,42]. For example, Conforti et al. found that women had a significantly greater survival benefit from ICI plus chemotherapy compared to men, whereas men benefited more from ICI monotherapy [9]. Similarly, Yu et al. reported that female patients had markedly better outcomes with PD-1 blockade plus chemotherapy than males, despite lower tumor mutational burden (TMB) in females [43].
Biological factors such as immune microenvironment, cytokine profiles, and TMB may underlie these differences. Females tend to have stronger humoral and cell-mediated immune responses, and sex-specific cytokine signatures (e.g., CXCL10, CCL5) have been linked to differential responses to anti-PD-1 therapy [12,44]. High TMB appears to equalize ICI efficacy between sexes, while low TMB may be associated with poorer outcomes in males, although the etiology remains unclear [13]. Real-world data and registry studies also show that females with advanced NSCLC generally have longer survival than males, even after adjusting for confounders, but the reasons remain incompletely understood, and we did not observe this effect in our analyses [13,44,45].
4.2. Disparity in Survival by Race
We found that Asian patients had decreased odds of death compared to white patients, both in the investigational arm and among all trial patients. While the p value for the comparison in the investigational arm was close to 0.05, indicating a higher chance that the difference in odds of death is due to random chance, the stronger effect size and p value among all trial patients support our conclusion that Asian patients have decreased odds of death compared to white patients. We also found significant underrepresentation of Black patients, which is in keeping with the literature. No studies reported subgroup survival analysis of Black or Native American or Alaskan Native patients. Racial disparities in survival for patients with non-small cell lung cancer (NSCLC) treated with ICIs are primarily driven by differences in access to therapy, but among those who receive ICIs, survival outcomes are generally similar across racial groups, with some studies suggesting equal or even superior outcomes for certain minorities.
Many Asian patients in our meta-analysis came from studies of predominantly or exclusively Asian patient populations that cited the need to explore potential racial differences in ICI response as a rationale for their population selection. This approach of intentional inclusion may be valuable in increasing the representation of Black and other minority groups in clinical trials.
Multiple large registry and database studies show that Black, Hispanic, and Asian patients are less likely to receive ICI therapy compared to White patients, even after adjusting for clinical and socioeconomic factors [46,47]. This disparity in access is a major contributor to overall survival differences at the population level. When minority patients do receive ICIs, most studies report no decrease in overall survival (OS) or progression-free survival (PFS) compared to White patients [48,49,50]. For example, a National Cancer Database analysis found that non-Hispanic Black patients had a lower risk of death than non-Hispanic White patients after adjusting for confounders (HR 0.85) [4,5,6,7]. Similarly, real-world and clinical trial data show comparable efficacy and safety of ICIs in Black and white patients [4]. In one study, Asian patients in the US were reported to exhibit longer survival than white or Black patients with mNSCLC, despite lower rates of receipt of ICIs [51]. Similarly, meta-analyses of ICI use across solid tumors [17], and in bladder cancer [18], have reported longer survival for Asian than White patients when treated with ICIs. While differences in tumor mutation profiles and PD-L1 expression may contribute to outcome variation, these do not fully explain survival disparities and are likely less influential than access and social determinants [52].
4.3. Disparity in Survival by Age
We found older patients ≥65 years old were underrepresented in mNSCLC clinical trials and there was no significant difference in OS benefit from investigational treatments compared with patients <65 years old, although the point estimate indicated a lower benefit for older patients (RHR 0.92, p = 0.19). Patients ≥65 also did not have increased odds of death. ICIs have improved survival for patients with advanced NSCLC across all age groups, but disparities persist in the magnitude of benefit for older adults. Subgroup analyses and meta-analyses consistently demonstrate that patients ≥65 years old experience similar overall survival (OS) and progression-free survival (PFS) benefits from ICIs compared to younger patients, with hazard ratios for OS typically ranging from 0.74 to 0.81 for older adults, indicating a meaningful reduction in risk of death compared to chemotherapy [4,5,6]. However, patients aged ≥75 or ≥80 years may experience attenuated survival gains. Several meta-analyses and real-world studies report that while ICIs remain effective in these age groups, the OS benefit is less pronounced, and some studies fail to show statistically significant improvement over chemotherapy for patients ≥75 years. For example, pooled analyses show HRs for OS approaching 1.0 in patients ≥75 years, and real-world data indicate shorter median OS in patients ≥80 years, often attributed to lower rates of second-line therapy and increased comorbidities [1,52,53].
Performance status and comorbidities are critical determinants of ICI benefit in older adults. 2025 guidelines from the National Comprehensive Cancer Network (NCCN) recommend that older patients with good performance status (Eastern Cooperative Oncology Group 0–2) and manageable comorbidities should receive standard ICI-based regimens, while frail patients or those with poor performance status may benefit from single-agent ICI or supportive care [6]. The IPSOS and CheckMate 817 trials support using single-agent atezolizumab or dual checkpoint inhibition in platinum-ineligible or frail older patients, with improved survival and manageable toxicity [20,54].
Toxicity profiles are generally similar across age groups, but older patients may be at higher risk for severe immune-related adverse events (irAEs). While some studies suggest younger patients are more likely to experience irAEs, others report higher rates of severe irAEs in those over 75, though overall rates remain acceptable and do not preclude ICI use based on age alone [6].
Immunosenescence and distinct tumor microenvironment features in older adults may influence ICI response, but do not preclude efficacy. Studies of patients ≥80 years with PD-L1-high NSCLC show similar objective response rates and PFS to younger patients, though OS may be shorter due to lower use of subsequent therapy and increased comorbidities [55,56,57].
4.4. Limitations
Our meta-analysis was limited by the lack of diversity among trial populations, particularly with poor inclusion of Black patients, women, and older patients (≥65), and a lack of data reporting by subgroups. Multiple analyses of pivotal NSCLC ICI trials show that Black patients typically comprise only 1.9–3% of trial participants, and Hispanic patients about 3–5.9%, despite representing 13% and 18% of the US population, respectively [53,58]. Even when reported, Black and Hispanic patients were underrepresented, causing trials to have insufficient Black patients to include in subgroup analysis. Non-standard age cutoffs (65 vs. 75) also limited data analysis, making it difficult to draw broad conclusions about whether age affects ICI efficacy. Furthermore, since the included studies did not report relevant hazard ratios for subgroup analysis of survival in the investigational treatment, our meta-analyses relied on odds ratios of death to evaluate absolute differences in survival. This approach fails to include time-to-event information. Our work was also restricted to completed trials registered on ClinicalTrials.gov. This approach excludes active studies that may have interim data on subgroup survival. Although only one of our analyses showed significant between-study heterogeneity, the studies we include reflect different populations, treatment combinations, and study designs. Improved trial diversity and standardized subgroup reporting would directly address many of these limitations.
5. Conclusions
This analysis demonstrates that prospective phase III trials of ICIs in mNSCLC have persistent underrepresentation of women, older adults, and racial minorities. Additionally, most trials lack subgroup analysis by age, race, or sex, limiting generalizability and our ability to determine how these factors affect treatment efficacy. Among studies reporting overall survival hazard ratios by subgroup, only 1 demonstrated benefit from the investigational treatment in women, compared with 11 in men. Similarly, a greater proportion of studies found that patients <65 years old benefited from the investigational treatment than patients ≥65 years old. This study did not identify significant differences in overall survival benefit on the investigational treatment across race, sex, or age subgroups. Meta-analyses of overall survival hazard ratios identified a non-significantly smaller benefit for women and patients ≥65 years old. Increased reporting of subgroup analyses and greater representation of women and older patients are needed to further evaluate these disparities. Meta-analyses of odds ratios of death revealed that Asian patients had decreased odds of death compared to white patients, in keeping with the existing literature. Black patients were severely underrepresented, making up only 1.5% of patients with reported race. These findings highlight the need for policy initiatives and trial design strategies that facilitate more representative trials and standardized reporting of subgroup analysis, ensuring generalizable and equitable evaluation of ICIs in mNSCLC treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Xu Y. Wang Q. Xie J. Chen M. Liu H. Zhan P. Lv T. Song Y. The Predictive Value of Clinical and Molecular Characteristics or Immunotherapy in Non-Small Cell Lung Cancer: A Meta-Analysis of Randomized Controlled Trials Front. Oncol.20211173221410.3389/fonc.2021.73221434557415 PMC 8453160 · doi ↗ · pubmed ↗
- 2Thandra K.C. Barsouk A.A. Saginala K. Aluru J.S. Barsouk A. Epidemiology of lung cancer Contemp. Oncol.202125455210.5114/wo.2021.103829 PMC 806389733911981 · doi ↗ · pubmed ↗
- 3Girigoswami A. Girigoswami K. Potential Applications of Nanoparticles in Improving the Outcome of Lung Cancer Treatment Genes 202314137010.3390/genes 1407137037510275 PMC 10379962 · doi ↗ · pubmed ↗
- 4Siciliano M.A. d’Apolito M. Del Giudice T. CaridàG. Grillone F. Porzio G. Giusti R. Tassone P. Barbieri V. Tagliaferri P. Do age and performance status matter? A systematic review and network meta-analysis of immunotherapy studies in untreated advanced/metastatic non-oncogene addicted NSCLC Front. Immunol.202516163505610.3389/fimmu.2025.163505641063998 PMC 12500590 · doi ↗ · pubmed ↗
- 5Ding Y. Lei S. Wang L. Tang L. Zhang Y. Liao Y. Deng X. Li Y. Gong Y. Li Y. Age-related efficacy of immunotherapies in advanced non-small cell lung cancer: A comprehensive meta-analysis Lung Cancer 202419510792510.1016/j.lungcan.2024.10792539146625 · doi ↗ · pubmed ↗
- 6Del Corral-Morales J. Ayala-de Miguel C. Quintana-Cortés L. Sánchez-Vegas A. Aranda-Bellido F. González-Santiago S. Fuentes-Pradera J. Miguel P.A.-D. Real-world data on immune-checkpoint inhibitors in elderly patients with advanced non-small cell lung cancer: A retrospective study Cancers 202517219410.3390/cancers 1713219440647491 PMC 12248468 · doi ↗ · pubmed ↗
- 7Sun Y.M. Wang Y. Sun X.X. Chen J. Gong Z.-P. Meng H.-Y. Clinical efficacy of immune checkpoint inhibitors in older non-small-cell lung cancer patients: A meta-analysis Front. Oncol.20201055845410.3389/fonc.2020.55845433072584 PMC 7538790 · doi ↗ · pubmed ↗
- 8Yang F. Markovic S.N. Molina J.R. Halfdanarson T.R. Pagliaro L.C. Chintakuntlawar A.V. Li R. Wei J. Wang L. Liu B. Association of sex, age, and Eastern Cooperative Oncology Group performance status with survival benefit of cancer immunotherapy in randomized clinical trials: A systematic review and meta-analysis JAMA Netw. Open.20203 e 201253410.1001/jamanetworkopen.2020.1253432766800 PMC 7414387 · doi ↗ · pubmed ↗