Correction: Dhillon et al. Molecular Insights and Therapeutic Advances in Low-Risk Myelodysplastic Neoplasms: A Clinical Review. Cancers 2025, 17, 3610
Vikram Dhillon, Jaroslaw Maciejewski, Suresh Kumar Balasubramanian

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
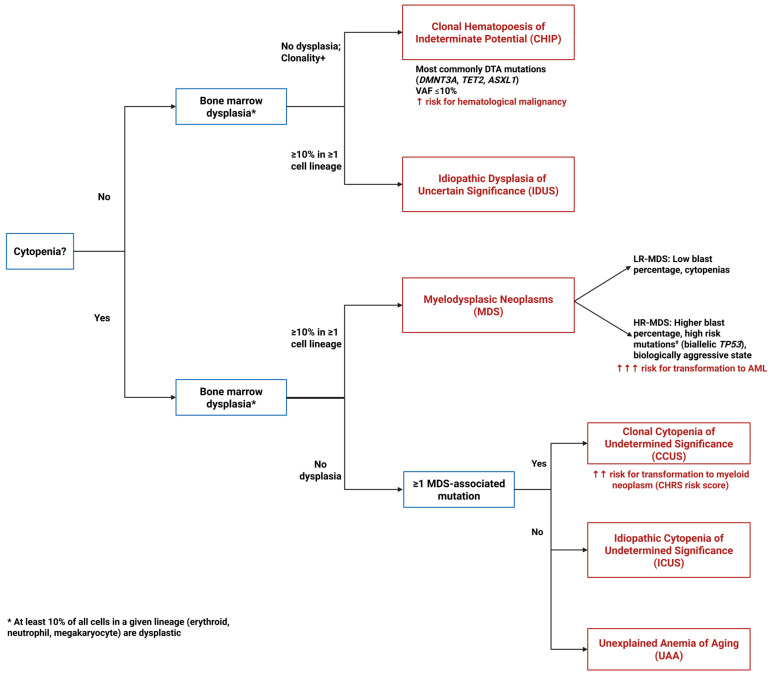 Figure 1
Figure 1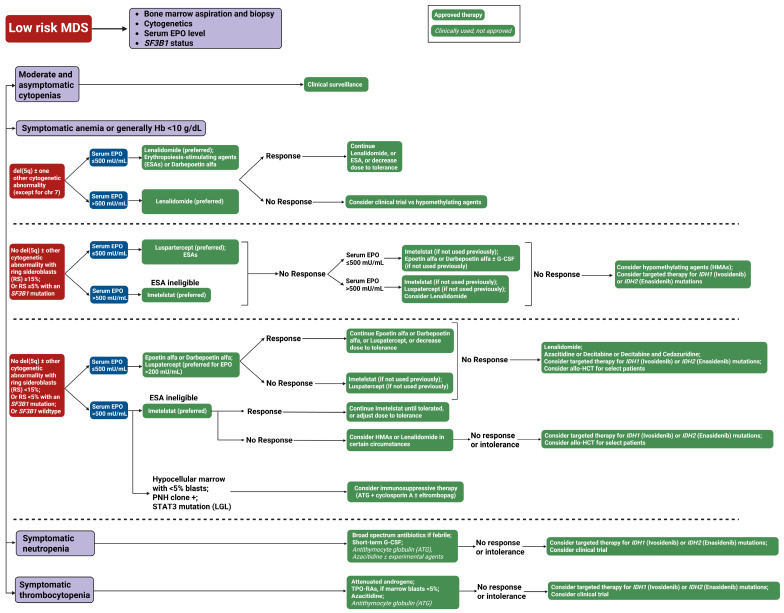 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Chronic Myeloid Leukemia Treatments · Myeloproliferative Neoplasms: Diagnosis and Treatment
Error in Figure 1 Legend
In the original publication [1], there was an error in the legend for Figure 1 as published. An incorrect version of the Figure 1 legend was inadvertently included in the revised manuscript. The correct legend appears below.
Figure 1. Diagnostic algorithm for pre-MDS conditions. This flowchart illustrates the diagnostic pathway for distinguishing between clonal and non-clonal cytopenias and dysplasia that can precede or may progress to MDS. The algorithm differentiates four key entities based on the presence or absence of cytopenias, dysplastic features, and clonal mutations: ICUS (Idiopathic Cytopenias of Uncertain Significance)—cytopenia without clonal mutations or dysplasia; CCUS (Clonal Cytopenias of Uncertain Significance)—cytopenia with clonal mutations but without dysplasia; CHIP (Clonal Hematopoiesis of Indeterminate Potential)—clonal mutations without cytopenia or dysplasia; and IDUS (Idiopathic Dysplasia of Unknown Significance)—morphologic dysplasia without cytopenia or clonal mutations. ^#^ High risk mutations include ASXL1, CBL, DNMT3A, ETV6, EZH2, IDH2, KRAS, NPM1, NRAS, RUNX1, SF3B1, SRSF2, and U2AF1.
Error in Figure 1
In the original publication, there was an error in Figure 1 as published. An incorrect version of Figure 1 was inadvertently included in the revised manuscript. The corrected Figure 1 appears below.
Error in Figure 3 Legend
In the original publication, there was an error in the legend for Figure 3 as published. An incorrect version of the Figure 3 legend was inadvertently included in the revised manuscript. The correct legend appears below.
Figure 3. Our treatment approach to low-risk myelodysplastic syndrome (LR-MDS). This flowchart outlines the therapeutic approach to low-risk MDS based on clinical presentation and laboratory parameters. The algorithm stratifies patients into four categories: Moderate and asymptomatic cytopenias (observation only), symptomatic anemia, symptomatic neutropenia, and symptomatic thrombocytopenia. Green boxes with solid backgrounds indicate FDA-approved therapies; green boxes with italicized text denote clinically used but not formally approved treatments. Blue boxes represent clinical decision points. Abbreviations: ATG, antithymocyte globulin; del(5q), deletion of chromosome 5q; chr, chromosome; EPO, erythropoietin; G-CSF, granulocyte colony-stimulating factor; Hb, hemoglobin; MDS, myelodysplastic syndrome; RBC, red blood cell; RS, ring sideroblasts; SF3B1, splicing factor 3B subunit 1 gene; TPO-RAs, thrombopoietin receptor agonists; and U/L, units per liter.
Error in Figure 3
In the original publication, there was an error in Figure 3 as published. An incorrect version of Figure 3 was inadvertently included in the revised manuscript. The corrected Figure 3 appears below.
Error in Table 1
In the original publication, there was an error in Table 1 as published. Under Imetelstat efficacy outcomes, the RBC-TI percentage was incorrectly listed as 40% when it should be 39.8%. The corrected Table 1 appears below.
Text Correction
There was an error in the original publication. Under Section 3.6. Telomerase inhibitor: Imetelstat, the RBC-TI percentage was incorrectly listed as 40% when it should be 39.8%. A correction has been made to Section 3.6, second paragraph:
Follow-up phase-II studies demonstrated durable transfusion independence in 42% of LR-MDS patients ineligible for ESA therapy [48]. The Phase-III IMerge trial (NCT02598661) enrolled 178 patients randomized to imetelstat or placebo [49]. In the treatment arm, about 40% achieved RBC-transfusion independence with durable responses lasting 52 weeks. Molecular profiling revealed SF3B1 as the most frequently mutated gene (75.8%), with SF3B1-mutant patients demonstrating superior transfusion independence rates with Imetelstat versus placebo (48.8% vs. 16.3% at 8 weeks) [49]. Responses varied across SF3B1 hotspots, with T663P and A744P mutations achieving 100% response rates, while the most common K700E hotspot achieved 43.9% response. Other frequently mutated genes also responded: TET2-mutant patients achieved 50% transfusion independence versus 21.4% with placebo, and ASXL1-mutant patients achieved 27.8% response versus 0% with placebo [49]. Notably, higher mutational burden (>2 mutations) was associated with enhanced response rates (45.5% versus 6.7% with placebo), and even patients harboring traditionally poor-prognosis mutations (TP53, ETV6, RUNX1, ASXL1, or EZH2) achieved 31.8% transfusion independence with Imetelstat versus 0% with placebo [50]. Neutropenia was the most serious adverse event (91% treatment arm vs. 47% placebo), though it is manageable with dose delays and reductions, and based on this trial, Imetelstat has received FDA approval for LR-MDS in heavily TD patients.
The authors state that the scientific conclusions are unaffected. This correction was approved by the Academic Editor. The original publication has also been updated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.